Toremifene
Toremifene, sold under the brand name Fareston among others, is a medication which is used in the treatment of advanced breast cancer in postmenopausal women.[5][6][3] It is taken by mouth.[5]
 | |
 | |
| Clinical data | |
|---|---|
| Pronunciation | /ˈtɔːrəmɪfiːn/ |
| Trade names | Fareston, others |
| Other names | (Z)-Toremifene; 4-Chlorotamoxifen; Acapodene; CCRIS-8745; FC-1157; FC-1157a; GTx-006; NK-622; NSC-613680 |
| AHFS/Drugs.com | Monograph |
| MedlinePlus | a608003 |
| License data | |
| Routes of administration | By mouth |
| Drug class | Selective estrogen receptor modulator |
| ATC code | |
| Pharmacokinetic data | |
| Bioavailability | Good[1] |
| Protein binding | >99%[1] |
| Metabolism | Liver (CYP3A4)[2][1] |
| Metabolites | N-Desmethyltoremifene; 4-Hydroxytoremifene; Ospemifene[3][4] |
| Elimination half-life | Toremifene: 5–6 days[3][1] Metabolites: 4–21 days[1][4] |
| Excretion | Feces: 70% (as metabolites)[1] |
| Identifiers | |
IUPAC name
| |
| CAS Number |
|
| PubChem CID | |
| IUPHAR/BPS | |
| DrugBank | |
| ChemSpider | |
| UNII | |
| KEGG | |
| ChEBI | |
| ChEMBL | |
| PDB ligand | |
| CompTox Dashboard (EPA) | |
| ECHA InfoCard | 100.125.139 |
| Chemical and physical data | |
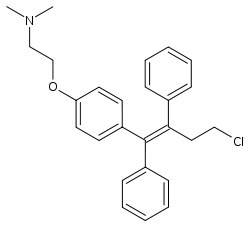
| Formula | C26H28ClNO |
| Molar mass | 405.97 g·mol−1 |
| 3D model (JSmol) | |
SMILES
| |
InChI
| |
| (verify) | |
Side effects of toremifene include hot flashes, sweating, nausea, vomiting, dizziness, vaginal discharge, and vaginal bleeding.[2][7] It can also cause blood clots, irregular heartbeat, cataracts, visual disturbances, elevated liver enzymes, endometrial hyperplasia, and endometrial cancer.[2] High blood calcium levels can occur in women with bone metastases.[2]
The medication is a selective estrogen receptor modulator (SERM) and hence is a mixed agonist–antagonist of the estrogen receptor (ER), the biological target of estrogens like estradiol.[2][7] It has estrogenic effects in bone, the liver, and the uterus and antiestrogenic effects in the breasts.[6][8][9][2] It is a triphenylethylene derivative and is closely related to tamoxifen.[10]
Toremifene was introduced for medical use in 1997.[11][12] It was the first antiestrogen to be introduced since tamoxifen in 1978.[13] It is available as a generic medication in the United States.[14]
Medical uses
Toremifene is approved for the treatment of metastatic breast cancer in postmenopausal women with estrogen receptor-positive or unknown-status tumors.[5][6] This is its only approved use in the United States.[4] It shows equivalent effectiveness to tamoxifen for this indication.[6] Toremifene has been found to be effective in the treatment of breast pain and may be a better drug than tamoxifen for this indication.[15] Toremifene has been reported to significantly improve symptoms of gynecomastia in men.[16]
Side effects
The side effects of toremifene are similar to those of tamoxifen.[2] The most common side effect is hot flashes.[2] Other side effects include sweating, nausea, vomiting, dizziness, vaginal discharge, and vaginal bleeding.[2][7] In women with bone metastases, hypercalcemia may occur.[2] Toremifene has a small risk of thromboembolic events.[2] Cataracts, vision changes, and elevation of liver enzymes have been reported.[2][7] The drug prolongs the QT interval and hence has a risk of potentially fatal dysrhythmias.[2] The risk of dysrhythmias can be reduced by avoiding use in patients with hypokalemia, hypomagnesemia, pre-existing QT prolongation, and in those taking other QT-prolonging drugs.[2] Because toremifene has estrogenic actions in the uterus, it can increase the risk of endometrial hyperplasia and endometrial cancer.[2]
Interactions
Toremifene is a substrate of CYP3A4, a cytochrome P450 enzyme, and hence drugs that induce or inhibit this enzyme can respectively decrease or increase levels of toremifene in the body.[2]
Pharmacology
Pharmacodynamics
Toremifene is a competitive ligand of the estrogen receptor and has mixed agonistic and antagonistic actions in a tissue-selective manner.[2][7] It has estrogenic activity in bone, partial estrogenic activity in the uterus and liver, and pure antiestrogenic activity in the breasts.[6][8][9][2] The drug is very similar to tamoxifen and shares most of its properties.[6][8][9][2] There are some indications that it may be safer than tamoxifen as it is not a hepatocarcinogen in animals and may have less potential for genotoxicity.[6][3] However, clinical studies have found no significant differences between toremifene and tamoxifen, including in terms of effectiveness, tolerability, and safety, and hence the clinical use of toremifene has been somewhat limited.[6][3]
Toremifene has been found to have antigonadotropic effects in postmenopausal women,[19] progonadotropic effects in men,[20] to increase sex hormone-binding globulin levels,[19] and to decrease insulin-like growth factor 1 levels by about 20% in postmenopausal women and men.[21]
Toremifene has about one-third of the potency of tamoxifen; i.e., 60 mg toremifene is roughly equivalent to 20 mg tamoxifen in the treatment of breast cancer.[22]
| Medication | Breast | Bone | Liver | Uterus | Vagina | Brain | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Lipids | Coagulation | SHBG | IGF-1 | Hot flashes | Gonadotropins | |||||||||
| Estradiol | + | + | + | + | + | + | + | + | + | + | ||||
| "Ideal SERM" | – | + | + | ± | ± | ± | – | + | + | ± | ||||
| Bazedoxifene | – | + | + | + | + | ? | – | ± | – | ? | ||||
| Clomifene | – | + | + | ? | + | + | – | ? | – | ± | ||||
| Lasofoxifene | – | + | + | + | ? | ? | ± | ± | – | ? | ||||
| Ospemifene | – | + | + | + | + | + | ± | ± | – | ± | ||||
| Raloxifene | – | + | + | + | + | + | ± | – | – | ± | ||||
| Tamoxifen | – | + | + | + | + | + | + | – | – | ± | ||||
| Toremifene | – | + | + | + | + | + | + | – | – | ± | ||||
| Effect: + = Estrogenic / agonistic. ± = Mixed or neutral. – = Antiestrogenic / antagonistic. Sources: See template. | ||||||||||||||
Pharmacokinetics
The bioavailability of toremifene has not been precisely determined but is known to be good.[1] The drug is more than 99% bound to plasma proteins.[1] It is metabolized in the liver primarily by CYP3A4 and then undergoes secondary hydroxylation.[1] The metabolites of toremifene include N-desmethyltoremifene and 4-hydroxytoremifene and are less active than toremifene itself.[1][23] Ospemifene (deaminohydroxytoremifene) is also a major metabolite of toremifene.[4] Toremifene and 4-hydroxytoremifene have a very long elimination half-life of 5 to 6 days, while N-desmethyltoremifene has an even longer elimination half-life of 6 to 21 days and ospemifene has an elimination half-life of 4 days.[1][4] The long elimination half-lives of toremifene and its metabolites can be attributed to enterohepatic recirculation.[2] Toremifene is eliminated 70% in the feces, as metabolites.[1]
Unlike tamoxifen, toremifene is not a prodrug and does not depend on metabolism by CYP2D6 for bioactivation; hence, it may be preferable to tamoxifen in CYP2D6 poor metabolizers or in patients who are taking a drug that inhibits CYP2D6.[24]
Chemistry
Toremifene, also known as 4-chlorotamoxifen, is a derivative of triphenylethylene and a close analogue of tamoxifen.[10] It is also closely related to afimoxifene (4-hydroxytamoxifen) and ospemifene (deaminohydroxytoremifene).[24][25]
History
Toremifene was introduced in the United States in 1997.[11][12] It was the first antiestrogen to be introduced in this country since tamoxifen in 1978.[13]
Society and culture
Research
Toremifene was also evaluated for prevention of prostate cancer and had the tentative brand name Acapodene.[30]
In 2007 the pharmaceutical company GTx, Inc was conducting two different phase 3 clinical trials; First, a pivotal Phase clinical trial for the treatment of serious side effects of androgen deprivation therapy (ADT) (especially vertebral/spine fractures and hot flashes, lipid profile, and gynecomastia) for advanced prostate cancer, and second, a pivotal Phase III clinical trial for the prevention of prostate cancer in high risk men with high grade prostatic intraepithelial neoplasia, or PIN. Results of these trials are expected by first quarter of 2008[31]
An NDA for the first application (relief of prostate cancer ADT side effects) was submitted in Feb 2009,[32] and in Oct 2009 the FDA said they would need more clinical data, e.g. another phase III trial.[33]
Ultimately, development was discontinued and toremifene was never marketed for complications associated with ADT or the treatment or prevention of prostate cancer.[34]
Phase III Trial Results
A double-blind, placebo-controlled, randomized, 3 year clinical trial of toremifene was conducted using a sample of 1,260 men. Subjects had a median age of 64 years and were diagnosed with high-grade prostatic intraepithelial neoplasia (HGPIN), which is considered premalignant, though Thompson and Leach feel a low grade PIN could also be deemed premalignant. [35]
The sponsor, GTx, who designed and managed the study, found 34.7% of the placebo and 32.3% of the toremifene groups had cancer events. No distinction was found in Gleason scores of either group.[36]
Previous murine studies using transgenic adenocarcinoma of mouse prostate (TRAMP) mice showed toremifene prevented palpable tumors in 60% of the animals. This study used toremifene as an early prophylactic, which differentiates it from the phase III human studies. [37]
References
- Vincent T. DeVita Jr.; Theodore S. Lawrence; Steven A. Rosenberg (7 January 2015). DeVita, Hellman, and Rosenberg's Cancer: Principles & Practice of Oncology. Wolters Kluwer Health. pp. 1126–. ISBN 978-1-4698-9455-3.
- Laura Rosenthal; Jacqueline Burchum (17 February 2017). Lehne's Pharmacotherapeutics for Advanced Practice Providers - E-Book. Elsevier Health Sciences. pp. 931–. ISBN 978-0-323-44779-9.
- Bruce A. Chabner; Dan L. Longo (7 December 2011). Cancer Chemotherapy and Biotherapy: Principles and Practice. Lippincott Williams & Wilkins. pp. 659–. ISBN 978-1-4511-4820-6.
- https://www.accessdata.fda.gov/drugsatfda_docs/label/2011/020497s006lbl.pdf
- https://www.accessdata.fda.gov/drugsatfda_docs/label/2011/020497s006lbl.pdf
- William R. Miller; James N. Ingle (8 March 2002). Endocrine Therapy in Breast Cancer. CRC Press. pp. 55–57. ISBN 978-0-203-90983-6.
- David Schiff; Isabel Arrillaga; Patrick Y. Wen (16 September 2017). Cancer Neurology in Clinical Practice: Neurological Complications of Cancer and its Treatment. Humana Press. pp. 296–. ISBN 978-3-319-57901-6.
- Monica Morrow; Virgil Craig Jordan (2003). Managing Breast Cancer Risk. PMPH-USA. pp. 192–. ISBN 978-1-55009-260-8.
- Selective Estrogen Receptor Modulators—Advances in Research and Application: 2013 Edition: ScholarlyBrief. ScholarlyEditions. 1 May 2013. pp. 51–. ISBN 978-1-4901-0447-8.
- Antonio Cano; Joacquim Calaf i Alsina; Jose Luis Duenas-Diez (22 September 2006). Selective Estrogen Receptor Modulators: A New Brand of Multitarget Drugs. Springer Science & Business Media. pp. 52–. ISBN 978-3-540-34742-2.
- Orlando E. Silva; Stefano Zurrida (2005). Breast Cancer: A Practical Guide. Elsevier Health Sciences. pp. 355–. ISBN 0-7020-2744-8.
- Wayne R. Bidlack; Stanley T. Omaye; Mark S. Meskin; Debra K.W. Topham (16 March 2000). Phytochemicals as Bioactive Agents. CRC Press. pp. 26–. ISBN 978-1-56676-788-0.
- Philip J. DiSaia; William T. Creasman; Robert S Mannel; D. Scott McMeekin, David G Mutch (4 February 2017). Clinical Gynecologic Oncology E-Book. Elsevier Health Sciences. pp. 124–. ISBN 978-0-323-44316-6.
- "Generic Fareston Availability - Drugs.com". Drugs.com. Retrieved 2019-04-19.
- Kirby I. Bland; Edward M. Copeland; V. Suzanne Klimberg; William J Gradishar (29 June 2017). The Breast E-Book: Comprehensive Management of Benign and Malignant Diseases. Elsevier Health Sciences. pp. 86–. ISBN 978-0-323-51187-2.
- Tabbal, Mahmoud; Fuleihan, Ghada El-Hajj (2010). "Future Therapies". Osteoporosis in Men. pp. 713–732. doi:10.1016/B978-0-12-374602-3.00057-2. ISBN 9780123746023.
- Mari J. Wirfs, PhD, MN, APRN, ANP-BC, FNP-BC, CNE (9 May 2019). The APRN and PA's Complete Guide to Prescribing Drug Therapy 2020. Springer Publishing Company. pp. 60–. ISBN 978-0-8261-7934-0.CS1 maint: multiple names: authors list (link)
- Casciato; Mary C. Territo (2012). Manual of Clinical Oncology. Lippincott Williams & Wilkins. pp. 122–. ISBN 978-1-4511-1560-4.
- Ellmén J, Hakulinen P, Partanen A, Hayes DF (November 2003). "Estrogenic effects of toremifene and tamoxifen in postmenopausal breast cancer patients" (PDF). Breast Cancer Res. Treat. 82 (2): 103–11. doi:10.1023/B:BREA.0000003957.54851.11. hdl:2027.42/44217. PMID 14692654.
- Tsourdi E, Kourtis A, Farmakiotis D, Katsikis I, Salmas M, Panidis D (April 2009). "The effect of selective estrogen receptor modulator administration on the hypothalamic-pituitary-testicular axis in men with idiopathic oligozoospermia". Fertil. Steril. 91 (4 Suppl): 1427–30. doi:10.1016/j.fertnstert.2008.06.002. PMID 18692782.
- Roelfsema F, Yang RJ, Takahashi PY, Erickson D, Bowers CY, Veldhuis JD (February 2018). "Effects of Toremifene, a Selective Estrogen Receptor Modulator, on Spontaneous and Stimulated GH Secretion, IGF-I, and IGF-Binding Proteins in Healthy Elderly Subjects". J Endocr Soc. 2 (2): 154–165. doi:10.1210/js.2017-00457. PMC 5789038. PMID 29383334.
- MacGregor JI, Jordan VC (June 1998). "Basic guide to the mechanisms of antiestrogen action". Pharmacol. Rev. 50 (2): 151–96. PMID 9647865.
- George M. Brenner; Craig Stevens (28 September 2017). Brenner and Stevens' Pharmacology E-Book. Elsevier Health Sciences. pp. 394–. ISBN 978-0-323-39172-6.
- Georg F. Weber (22 July 2015). Molecular Therapies of Cancer. Springer. pp. 304–. ISBN 978-3-319-13278-5.
- Philipp Y. Maximov; Russell E. McDaniel; V. Craig Jordan (23 July 2013). Tamoxifen: Pioneering Medicine in Breast Cancer. Springer Science & Business Media. pp. 170–. ISBN 978-3-0348-0664-0.
- J. Elks (14 November 2014). The Dictionary of Drugs: Chemical Data: Chemical Data, Structures and Bibliographies. Springer. pp. 1222–. ISBN 978-1-4757-2085-3.
- Index Nominum 2000: International Drug Directory. Taylor & Francis. 2000. pp. 1048–. ISBN 978-3-88763-075-1.
- I.K. Morton; Judith M. Hall (6 December 2012). Concise Dictionary of Pharmacological Agents: Properties and Synonyms. Springer Science & Business Media. pp. 277–. ISBN 978-94-011-4439-1.
- "Toremifene - Drugs.com". Drugs.com. Retrieved 2018-02-08.
- Price N, Sartor O, Hutson T, Mariani S. Role of 5a-reductase inhibitors and selective estrogen receptor modulators as potential chemopreventive agents for prostate cancer. Clin Prostate Cancer 2005;3:211-4. PMID 15882476
- "GTx's Phase III Clinical Development of ACAPODENE on Course Following Planned Safety Review" (Press release). GTx Inc. 2007-07-12. Retrieved 2006-07-14.
- "GTx Announces Toremifene 80 mg NDA Accepted for Review by FDA" (Press release).
- "GTx and Ipsen End Prostate Cancer Collaboration due to Costs of FDA-Requested Phase III Study". 2 Mar 2011.
- "Toremifene - AdisInsight". adisinsight.springer.com. Retrieved 2018-02-08.
- Thompson Jr, I. M., and Leach, R., Prostate cancer and prostatic intraepithelial neoplasia: true, true, and unrelated? J Clin Oncol, 2013;31:515-6. https://ascopubs.org/doi/full/10.1200/JCO.2012.46.6151= Retrieved 31 July 2019
- Taneja, S. S., Morton, R., Barnette, G., Sieber, P., Hancock, M. L., and Steiner, M., Prostate cancer diagnosis among men with isolated high-grade intraepithelial neoplasia enrolled onto a 3-year prospective phase III clinical trial of oral toremifene J Clin Oncol, 2013;31:523-9. https://ascopubs.org/doi/abs/10.1200/JCO.2012.41.7634= Retrieved 31 July 2019
- Raghow, S., Hooshdaran, M. Z., Katiyar, S., and Steiner, M. S., Toremifene prevents prostate cancer in the transgenic adenocarcinoma of mouse prostate model. Cancer Research 2002;62:1370-6. http://cancerres.aacrjournals.org/content/62/5/1370= Retrieved 31 July 2019
Further reading
- Taras TL, Wurz GT, Linares GR, DeGregorio MW (2000). "Clinical pharmacokinetics of toremifene". Clin Pharmacokinet. 39 (5): 327–34. doi:10.2165/00003088-200039050-00002. PMID 11108432.
- Harvey HA, Kimura M, Hajba A (2006). "Toremifene: an evaluation of its safety profile". Breast. 15 (2): 142–57. doi:10.1016/j.breast.2005.09.007. PMID 16289904.
- Taneja SS, Smith MR, Dalton JT, Raghow S, Barnette G, Steiner M, Veverka KA (2006). "Toremifene--a promising therapy for the prevention of prostate cancer and complications of androgen deprivation therapy". Expert Opin Investig Drugs. 15 (3): 293–305. doi:10.1517/13543784.15.3.293. PMID 16503765.
- Zhou WB, Ding Q, Chen L, Liu XA, Wang S (2011). "Toremifene is an effective and safe alternative to tamoxifen in adjuvant endocrine therapy for breast cancer: results of four randomized trials". Breast Cancer Res. Treat. 128 (3): 625–31. doi:10.1007/s10549-011-1556-5. PMID 21553116.
- Gennari L, Merlotti D, Stolakis K, Nuti R (2012). "Pharmacokinetic evaluation of toremifene and its clinical implications for the treatment of osteoporosis". Expert Opin Drug Metab Toxicol. 8 (4): 505–13. doi:10.1517/17425255.2012.665873. PMID 22356442.
- Mao C, Yang ZY, He BF, Liu S, Zhou JH, Luo RC, Chen Q, Tang JL (2012). "Toremifene versus tamoxifen for advanced breast cancer". Cochrane Database Syst Rev (7): CD008926. doi:10.1002/14651858.CD008926.pub2. PMID 22786516.
- Vogel CL, Johnston MA, Capers C, Braccia D (2014). "Toremifene for breast cancer: a review of 20 years of data". Clin. Breast Cancer. 14 (1): 1–9. doi:10.1016/j.clbc.2013.10.014. PMID 24439786.
- Mustonen MV, Pyrhönen S, Kellokumpu-Lehtinen PL (2014). "Toremifene in the treatment of breast cancer". World J Clin Oncol. 5 (3): 393–405. doi:10.5306/wjco.v5.i3.393. PMC 4127610. PMID 25114854.