

STDs in Men Who Have Sex with Men
 ShareCompartir
ShareCompartir
Public Health Impact
The incidence of many STDs in gay, bisexual, and other men who have sex with men (collectively referred to as MSM) – including primary and secondary (P&S) syphilis and antimicrobial-resistant gonorrhea – is greater than that reported in women and men who have sex with women only (MSW).1-6 In addition to the negative effects of untreated STDs, elevated STD burden is of concern because it may indicate high risk for subsequent HIV infection. Annual increases in reported STD cases could reflect increased frequency of behaviors that transmit both STDs and HIV (e.g., condomless anal sex), and having an STD increases the risk of acquisition or transmission of HIV.7-14
The relatively high incidence of STD infection among MSM may be related to multiple factors, including individual behaviors and sexual network characteristics.15-17 The number of lifetime or recent sex partners, rate of partner exchange, and frequency of condomless sex each influence an individual’s probability of exposure to STDs.15 However, MSM network characteristics such as high prevalence of STDs, interconnectedness and concurrency of sex partners, and possibly limited access to health care also affect the risk of acquiring an STD.15, 18 Furthermore, experiences of stigma – verbal harassment, discrimination, or physical assault based on attraction to men – are associated with increased sexual risk behavior among MSM.19
Disparities among MSM reflect those observed in the general population, with disproportionate incidence of STDs reported among racial and ethnic minority MSM, MSM of lower socioeconomic status, and young MSM.20-24 The higher burden of STDs among MSM with these characteristics, relative to the general population of MSM, may suggest distinct mixing patterns in their sexual networks, reduced access to screening and treatment, and differential experiences of stigma and discrimination, rather than greater numbers of sexual partners or frequency of condomless sex.15, 21-22, 24-26 Disparities may also be more pronounced for racial and ethnic minority MSM who are also unemployed, young, and/or of lower socioeconomic status.26-27
With the exception of reported syphilis cases, nationally notifiable STD surveillance data do not routinely include information on sexual behaviors and these data are missing for the majority of gonorrhea and chlamydia cases reported to CDC. Therefore, trends in STDs among MSM in the United States are based on findings from sentinel and enhanced surveillance systems. Testing strategies are also evolving to include more extragenital STD screening, which may increase detection of asymptomatic infections. Until recently, testing for gonorrhea and chlamydia in MSM largely focused on detecting urethral infections, which are more likely to be symptomatic than pharyngeal or rectal infections.28
For data reported in this chapter, MSM were defined as men who either reported having one or more male sex partners or who self-reported as gay/ homosexual or bisexual. MSW were defined as men who reported having sex with women only or who did not report the sex of their sex partner, but reported that they considered themselves straight/heterosexual. Data presented in this chapter are derived from the National Notifiable Diseases Surveillance System (NNDSS), the Gonococcal Isolate Surveillance Project (GISP), and the STD Surveillance Network (SSuN), a sentinel and enhanced surveillance project established in 2005 to provide supplemental information on STDs.
Nationally Notifiable Syphilis Surveillance Data
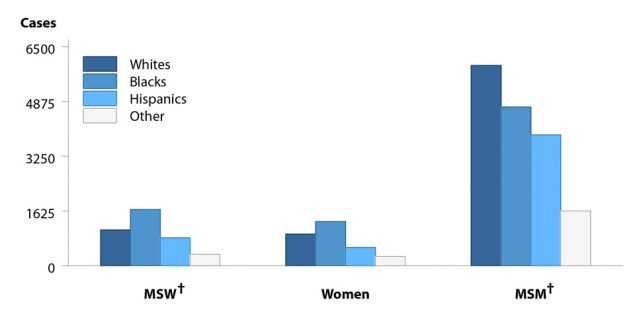
MSM accounted for 80.6% of male P&S syphilis cases with information about sex of sex partners in 2016 (Figure 36). Of MSM P&S syphilis cases, 36.8% were White, 29.1% were Black, and 24.0% were Hispanic (Figure X). Relative to the percentage of the US population that is White (62.3%), Black (12.3%), and Hispanic (17.1%), this represents a significant inequality in the burden of disease for non-White MSM, which was also evident among MSW and women.30 In addition, among MSM P&S syphilis cases with known HIV status in 2016, 47.0% were also reported to be HIV-positive (Figure 41).
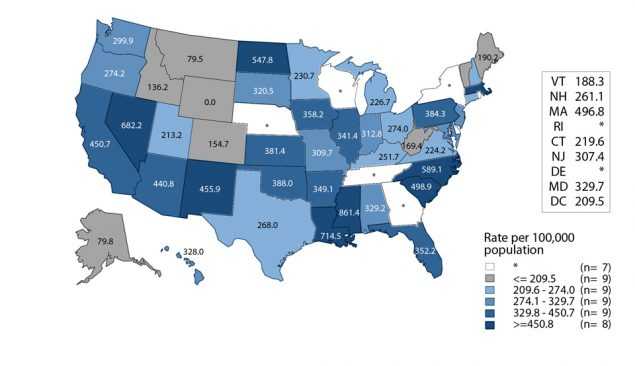
In 2016, 44 areas (43 states and the District of Columbia) provided data to classify at least 70% of cases as MSM, MSW, or women. Among these areas, estimated rates of P&S syphilis cases in MSM ranged from 0 cases per 100,000 MSM in Wyoming to 861 cases per 100,000 MSM in Mississippi, with 26 states (59%) estimated to have rates between 200 and 400 cases per 100,000 MSM (Figure Y).
When examining reported P&S syphilis cases over time, 36 states were able to classify at least 70% of reported P&S syphilis cases as MSM, MSW, or women each year during 2012–2016. In these states, cases among MSM increased 16.4% during 2015–2016 and 63.7% during 2012–2016 (Figure 35). However, the percentage of P&S syphilis cases that were attributed to MSM in those states fell slightly in 2012 to 68.6% in 2016.
A description of the methods for estimating MSM population sizes for rate denominators can be found in Section A1.2 of the Appendix. More information about syphilis can be found in the Syphilis section of the National Profile.
Gonococcal Isolate Surveillance Project
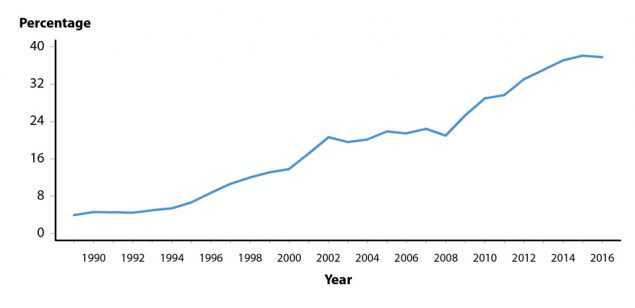
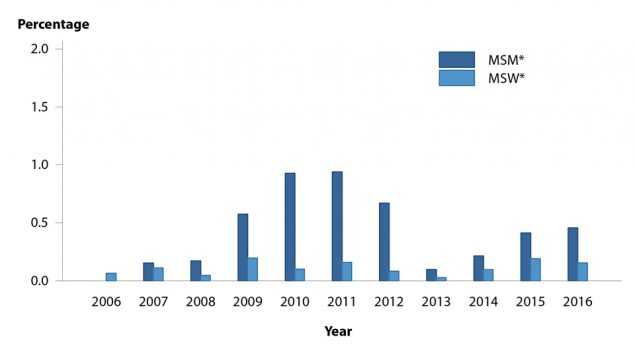
GISP is a national sentinel surveillance system designed to monitor trends in antimicrobial susceptibilities of Neisseria gonorrhoeae strains in the United States.31 Overall, the proportion of isolates collected in selected STD clinics participating in GISP that were from MSM increased steadily, from 3.9% in 1989 to 38.1% in 2015 and decreased to 37.8% in 2016 (Figure Z). The reason for this increase over time is unclear, but might reflect changes in the epidemiology of gonorrhea or in health care seeking behavior of men infected with gonorrhea. GISP has demonstrated that gonococcal isolates from MSM are more likely to exhibit antimicrobial resistance than isolates from MSW.3, 4 During 2007–2016, the proportion of isolates with elevated ceftriaxone minimum inhibitory concentrations (MICs) (≥0.125 µg/ ml) was higher in isolates from MSM than from MSW (Figure AA). Information on the antimicrobial susceptibility criteria used in GISP can be found in Section A2.3 of the Appendix. More information about GISP and additional data can be found at https://www.cdc.gov/std/GISP.
STD Surveillance Network
SSuN is an ongoing collaboration of state, county and city health departments collecting enhanced provider- and patient-based information among a random sample of reported gonorrhea cases, as well as clinical and behavioral information among all patients attending STD clinics in collaborating jurisdictions.29 Data for 2016 were obtained from 29 STD clinics in SSuN jurisdictions.
Additional information about SSuN found in Section A2.2 of the Appendix.
Gonorrhea, 2010–2015
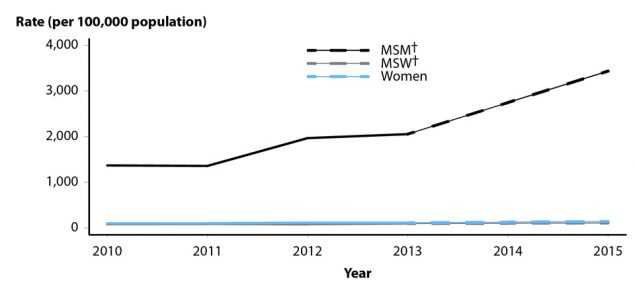
The number of diagnosed and reported gonorrhea cases among MSM was estimated at the county level based on patient interviews conducted among a random sample of all cases reported to six health departments continuously collaborating in the STD Surveillance Network between January 2010 and June 2013, and again July through December 2015. Estimates of the size of the MSM population in each county were obtained from published estimates and used to estimate the incidence of reported gonorrhea by year among MSM in the six collaborating SSuN sites.32, 33 Estimated gonorrhea incidence among MSM increased 151.0% across the study period from 1,368.6 cases per 100,000 MSM in 2010 to 3,434.7 cases per 100,000 MSM in 2015 (Figure BB). Over the same time period, estimated gonorrhea rates among women and MSW also increased, but by a significantly smaller proportion (39.8% and 31.7%, respectively).33
Gonorrhea and Chlamydia in STD Clinics, 2016
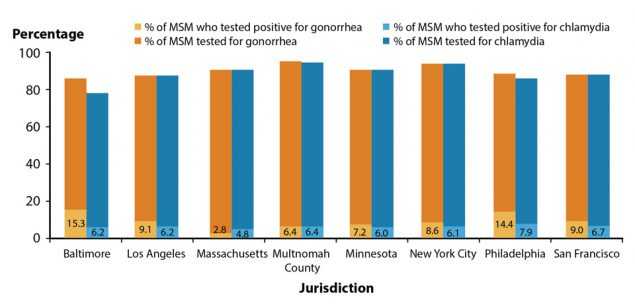
In 2016, 25,880 unique MSM presented for care in the 29 STD clinics in nine SSuN jurisdictions. In total, 22,418 unique MSM were tested for urogenital gonorrhea and/ or chlamydia (22,404 for gonorrhea, 22,152 for chlamydia). The proportion of men tested for urogenital infections was similar across SSuN jurisdictions, though the proportion who tested positive (positivity) varied by SSuN jurisdiction (Figure CC). In general, urogenital gonorrhea positivity was higher than urogenital chlamydia positivity (except in Massachusetts and Multnomah County); median site-specific positivity for gonorrhea was 8.8% (range by jurisdiction: 2.8%–15.3%) and for chlamydia was 6.3% (range: 4.8%–10.3%).
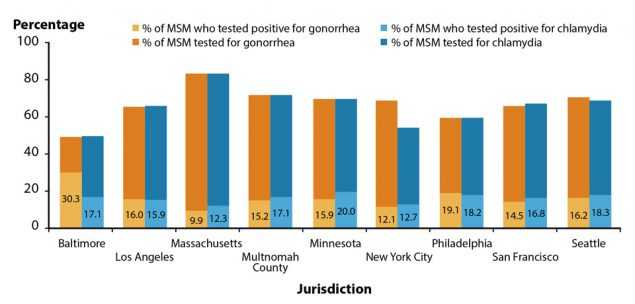
A total of 17,489 unique MSM were tested for rectal gonorrhea and/or chlamydia in 2016 (17,467 for gonorrhea, 17,445 for chlamydia) (Figure DD). In most jurisdictions, similar proportions of MSM were tested for rectal gonorrhea and chlamydia, likely reflecting use of dual diagnostic tests. Compared to urogenital testing, a lower proportion of MSM were tested for rectal infection. The median site-specific positivity for rectal gonorrhea was 15.9% (range: 9.9%–30.3%) and for rectal chlamydia was 17.2% (range: 12.3%–20.0%).
During 2016, 15,680 MSM were tested at the oropharyngeal site for gonorrhea (Figure EE). The median site-specific positivity for oropharyngeal gonorrhea was 8.8% (range by jurisdiction: 1.0%–16.1%). Oropharyngeal chlamydia data are not shown as some of the SSuN jurisdictions do not offer routine testing for oropharyngeal chlamydia infections.

HIV Status and STDs in STD Clinics, 2016
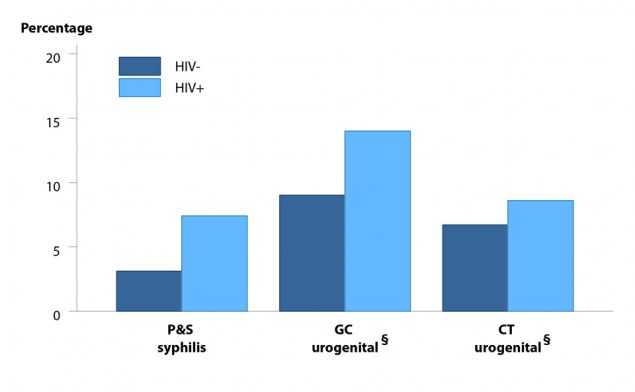
Among HIV-positive MSM visiting SSuN STD clinics in 2016, urogenital chlamydia positivity was 8.6% and urogenital gonorrhea positivity was 14.0% (compared to 6.7% and 9.0%, respectively, among HIV-negative MSM) (Figure FF). Among HIV- positive MSM, 7.4% were diagnosed with P&S syphilis compared to 3.1% of HIV-negative MSM. Percentages represent the overall average of the mean value by jurisdiction.
Summary
The number of reported P&S syphilis cases among MSM continued to rise in 2016 and the majority of P&S syphilis cases remained among MSM. Estimated rates of reported gonorrhea incidence increased among MSM in SSuN jurisdictions in recent years. Furthermore, the proportion of GISP isolates with elevated MICs to antimicrobials currently used to treat gonorrhea was higher among MSM than among MSW.
Beyond STD burden in the general MSM population, the data indicated heterogeneity of STD prevalence among MSM according to geography, race and ethnicity, and HIV status. State-specific P&S syphilis rate estimates among MSM varied from 0 to over 800 cases per 100,000 MSM and the prevalence of diagnosed STDs among MSM differed by SSuN jurisdiction. Reported P&S syphilis was disproportionately prevalent among Black and Hispanic MSM, and data from MSM who attended SSuN clinics suggested that P&S syphilis, urogenital gonorrhea, and urogenital chlamydia may be more prevalent among MSM living with diagnosed HIV infection than among HIV-negative MSM.
References
- An Q, Wejnert C, Bernstein K, et al. Syphilis screening and diagnosis among men who have sex with men, 2008–2014, 20 US cities. JAIDS 2017; 75(Suppl 3):S363–S369.
- de Voux A, Kidd S, Grey JA, et al. State-specific rates of primary and secondary syphilis among men who have sex with men — United States, 2015. MMWR Morb Mortal Wkly Rep 2017; 66(13):349–354. https://www.cdc.gov/mmwr/volumes/66/wr/pdfs/mm6613a1.pdf
-
Kirkcaldy RD, Harvey A, Papp JR, et al. Neisseria gonorrhoeae antimicrobial susceptibility surveillance — the Gonococcal Isolate Surveillance Project, 27 sites, United States, 2014. MMWR Surveill Summ 2016; 65(SS-7):1–19.
https://www.cdc.gov/mmwr/volumes/65/ss/ss6507a1.htm - Kirkcaldy RD, Zaidi A, Hook EW 3rd, et al. Neisseria gonorrhoeae antimicrobial resistance among men who have sex with men and men who have sex exclusively with women: The Gonococcal Isolate Surveillance Project, 2005–2010. Ann Intern Med 2013; 158(5 Pt 1):321–328.
-
Patton ME, Su JR, Nelson R, et al. Primary and secondary syphilis — United States, 2005– 2013. MMWR Morb Mortal Wkly Rep 2014; 63(18):402–406.
https://www.cdc.gov/mmwr/preview/mmwrhtml/mm6318a4.htm - Peterman TA, Su J, Bernstein KT, et al. Syphilis in the United States: on the rise? Expert Rev Anti Infect Ther 2015; 13(2):161–168.
- Solomon MM, Mayer KH. Evolution of the syphilis epidemic among men who have sex with men. Sex Health 2014; 12(2):96–102.
- Buchacz K, Patel P, Taylor M, et al. Syphilis increases HIV viral load and decreases CD4 cell counts in HIV-infected patients with new syphilis infections. AIDS 2004; 18(15):2075– 2079.
- Fleming DT, Wasserheit JN. From epidemiologic synergy to public health policy and practice: the contribution of other sexually transmitted diseases to sexual transmission of HIV infection. Sex Transm Infect 1999; 75(1):3–17.
- Jarzebowski W, Caumes E, Dupin N, et al. Effect of early syphilis infection on plasma viral load and CD4 cell count in human immunodeficiency virus- infected men: results from the FHDH-ANRS CO4 cohort. Arch Intern Med 2012; 172(16):1237–1243.
- Katz DA, Dombrowski JC, Bell TR, et al. HIV incidence among men who have sex with men after diagnosis with sexually transmitted infections. Sex Transm Dis 2016; 43(4):249– 254.
- Kelley CF, Vaughan AS, Luisi N, et al. The effect of high rates of bacterial sexually transmitted infections on HIV incidence in a cohort of black and white men who have sex with men in Atlanta, Georgia. AIDS Res Hum Retroviruses 2015; 31(6):587–592.
- Pathela P, Braunstein SL, Blank S, et al. HIV incidence among men with and those without sexually transmitted rectal infections: estimates and HIV case registry. Clin Infect Dis 2013; 57(8):1203–1209.
- Solomon MM, Mayer KH, Glidden DV, et al. Syphilis predicts HIV incidence among men and transgender women who have sex with men in a preexposure prophylaxis trial. Clin Infect Dis 2014; 59(7):1020–1026.
- Glick SN, Morris M, Foxman B, et al. A comparison of sexual behavior patterns among men who have sex with men and heterosexual men and women. J Acquir Immune Defic Syndr 2012; 60(1):83–90.
- Paz-Bailey G, Mendoza MCB, Finlayson T, et al. Trends in condom use among MSM in the United States: the role of antiretroviral therapy and seroadaptive strategies. AIDS 2016; 30(12):1985–1990.
- Spicknall IH, Gift TL, Bernstein KT, et al. Sexual networks and infection transmission networks among men who have sex with men as causes of disparity and targets of prevention. Sex Transm Infect 2017; 93(5):307–308.
- Alvy LM, McKirnan DJ, Du Bois SN, et al. Health care disparities and behavioral health among men who have sex with men. J Gay Lesbian Soc Serv 2011; 23(4):507–522.
- Balaji AB, Bowles KE, Hess KL, et al. Association between enacted stigma and HIV- related risk behavior among MSM, National HIV Behavioral Surveillance System, 2011. AIDS Behav 2017; 21(1):227–237.
- Brewer TH, Schillinger J, Lewis FM, et al. Infectious syphilis among adolescent and young adult men: implications for human immunodeficiency virus transmission and public health interventions. Sex Transm Dis 2011; 38(5):367–371.
- Jeffries WL, Marks G, Lauby J. Homophobia is associated with sexual behavior that increases risk of acquiring and transmitting HIV infection among black men who have sex with men. AIDS Behav 2013; 17(4):1442–1453.
- McKirnan DJ, Du Bois SN, Alvy LM, et al. Health care access and health behaviors among men who have sex with men: the cost of health disparities. Health Educ Behav 2013; 40(1):32– 41.
- Su JR, Beltrami JF, Zaidi AA, et al. Primary and secondary syphilis among black and Hispanic men who have sex with men: case report data from 27 States. Ann Intern Med 2011; 155(3):145–151.
- Díaz RM, Ayala G, Bein E. Sexual risk as an outcome of social oppression: data from a probability sample of Latino gay men in three US cities. Cultur Divers Ethnic Minor Psychol 2004; 10(3):255–267.
- Millett GA, Flores SA, Peterson JL, et al. Explaining disparities in HIV infection among black and white men who have sex with men: a meta-analysis of HIV risk behaviors. AIDS 2007; 21(15):2083–2091.
- Sullivan PS, Peterson J, Rosenberg ES, et al. Understanding racial HIV/STI disparities in black and white men who have sex with men: a multilevel approach. PLoS One 2014; 9(3):e90514.
- Mayer KH, Wang L, Koblin B, et al. Concomitant socioeconomic, behavioral, and biological factors associated with the disproportionate HIV infection burden among black men who have sex with men in 6 US cities. PLoS One 2014; 9(1):e87298.
- Patton ME, Kidd S, Llata E, et al. Extragenital gonorrhea and chlamydia testing and infection among men who have sex with men — STD Surveillance Network, United States, 2010– 2012. Clin Infect Dis 2014; 58(11):1564–1570.
- Rietmeijer K, Donnelly J, Bernstein K, et al. Here comes the SSuN — early experiences with the STD Surveillance Network. Pub Health Rep 2009; 124(Suppl 2):72–77.
- 2011–2015 American Community Survey 5-Year Summary File. Table DP05 — ACS demographic and housing estimates. Washington, DC: US Census Bureau; 2016.
- Schwarcz S, Zenilman J, Schnell D, et al. National surveillance of antimicrobial resistance in Neisseria gonorrhoeae. JAMA 1990; 264(11):1413–1417.
- Grey JA, Bernstein KT, Sullivan PS, et al. Estimating the population sizes of men who have sex with men in US states and counties using data from the American Community Survey. JMIR Public Health Surveill 2016; 2(1):e14.
- Stenger M, Pathela P, Anschuetz G, et al. Increases in the rate of Neisseria gonorrhoeae among gay, bisexual and other men who have sex with men (MSM) — findings from the STD Surveillance Network 2010–2015. Sex Transm Dis 2017; 44(7):393–397.
- Page last reviewed: August 18, 2017
- Page last updated: August 18, 2017
- Content source: