Melanoma
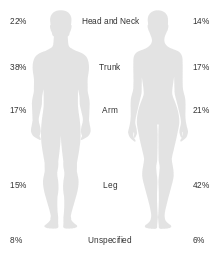
Melanoma, also known as malignant melanoma, is a type of cancer that develops from the pigment-containing cells known as melanocytes.[1] Melanomas typically occur in the skin, but may rarely occur in the mouth, intestines, or eye (uveal melanoma).[1][2] In women, they most commonly occur on the legs, while in men they are most common on the back.[2] About 25% of melanomas develop from moles.[2] Changes in a mole that can indicate melanoma include an increase in size, irregular edges, change in color, itchiness, or skin breakdown.[1]
| Melanoma | |
|---|---|
| Other names | Malignant melanoma |
 | |
| A melanoma of approximately 2.5 cm (1 in) by 1.5 cm (0.6 in) | |
| Pronunciation |
|
| Specialty | Oncology and dermatology |
| Symptoms | Mole that is increasing in size, has irregular edges, change in color, itchiness, or skin breakdown.[1] |
| Causes | Ultraviolet light (Sun, tanning devices)[2] |
| Risk factors | Family history, many moles, poor immune function[1] |
| Diagnostic method | Tissue biopsy[1] |
| Differential diagnosis | Seborrheic keratosis, lentigo, blue nevus, dermatofibroma[3] |
| Prevention | Sunscreen, avoiding UV light[2] |
| Treatment | Surgery[1] |
| Prognosis | Five-year survival rates in USA 99% (localized), 25% (disseminated)[4] |
| Frequency | 3.1 million (2015)[5] |
| Deaths | 59,800 (2015)[6] |
The primary cause of melanoma is ultraviolet light (UV) exposure in those with low levels of skin pigment.[2][7] The UV light may be from the sun or other sources, such as tanning devices.[2] Those with many moles, a history of affected family members, and who have poor immune function are at greater risk.[1] A number of rare genetic defects such as xeroderma pigmentosum also increase risk.[8] Diagnosis is by biopsy and analysis of any skin lesion that has signs of being potentially cancerous.[1]
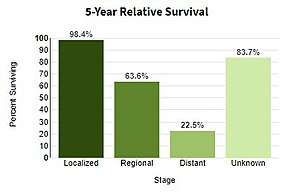
Using sunscreen and avoiding UV light may prevent melanoma.[2] Treatment is typically removal by surgery.[1] In those with slightly larger cancers, nearby lymph nodes may be tested for spread (metastasis).[1] Most people are cured if spread has not occurred.[1] For those in whom melanoma has spread, immunotherapy, biologic therapy, radiation therapy, or chemotherapy may improve survival.[1][9] With treatment the five-year survival rates in the United States is 99% among those with localized disease, 65% when spread has occurred to lymph nodes, and 25% among those with distant spread.[4] The likelihood that it will come back or spread depends how thick the melanoma is, how fast the cells are dividing, and whether or not the overlying skin has broken down.[2]
Melanoma is the most dangerous type of skin cancer.[2] Globally, in 2012, it newly occurred in 232,000 people.[2] In 2015 there were 3.1 million with active disease which resulted in 59,800 deaths.[5][6] Australia and New Zealand have the highest rates of melanoma in the world.[2] There are also high rates in Northern Europe and North America, while it is less common in Asia, Africa, and Latin America.[2] Melanoma is more common in men than women.[8] Melanoma has become more common since the 1960s in areas which are mostly populated with white people.[2][8]
Signs and symptoms
Early signs of melanoma are changes to the shape or color of existing moles or, in the case of nodular melanoma, the appearance of a new lump anywhere on the skin. At later stages, the mole may itch, ulcerate or bleed. Early signs of melanoma are summarized by the mnemonic "ABCDEF":[10][11]
- Asymmetry
- Borders (irregular with edges and corners)
- Color (variegated)
- Diameter (greater than 6 mm (0.24 in), about the size of a pencil eraser)
- Evolving over time
- Funny looking
This classification does not apply to nodular melanoma, which has its own classifications:[12]
- Elevated above the skin surface
- Firm to the touch
- Growing
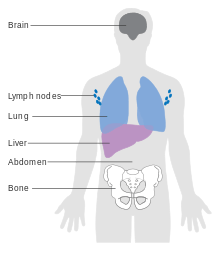
Metastatic melanoma may cause nonspecific paraneoplastic symptoms, including loss of appetite, nausea, vomiting and fatigue. Metastasis (spread) of early melanoma is possible, but relatively rare: less than a fifth of melanomas diagnosed early become metastatic. Brain metastases are particularly common in patients with metastatic melanoma.[13] It can also spread to the liver, bones, abdomen or distant lymph nodes.
Cause
Melanomas are usually caused by DNA damage resulting from exposure to ultraviolet light from the sun. Genetics also plays a role.[14][15] Melanoma can also occur in skin areas with little sun exposure (i.e. mouth, soles of feet, palms of hands, genital areas).[16] People with dysplastic nevus syndrome, also known as familial atypical multiple mole melanoma (FAMMM), are at increased risk for the development of melanoma.[17]
Having more than fifty moles indicates an increased risk melanoma might arise. A weakened immune system makes it easier for cancer to arise due to the body's weakened ability to fight cancer cells.[14]
UV radiation
The ultraviolet radiation from tanning beds increases the risk of melanoma.[18] The International Agency for Research on Cancer finds that tanning beds are "carcinogenic to humans" and that people who begin using tanning devices before the age of thirty years are 75% more likely to develop melanoma.[19]
Those who work in airplanes also appear to have an increased risk, believed to be due to greater exposure to UV.[20]
Ultraviolet UVB light (wavelengths between 315–280 nm) from the sun is absorbed by skin cell DNA and results in a type of direct DNA damage called cyclobutane pyrimidine dimers (CPDs). Thymine-thymine, cytosine-cytosine or cytosine-thymine dimers are formed by the joining of two adjacent pyrimidine bases within a DNA strand. Somewhat similarly to UVB, UVA light (longer wavelengths between 400–315 nm) from the sun or from tanning beds can also be directly absorbed by skin DNA (at about 100 to 1000 fold lower efficiency than UVB is absorbed).[21]
Exposure to ultraviolet radiation (UVA and UVB) is one of the major contributors to the development of melanoma.[22] Occasional extreme sun exposure (resulting in "sunburn") is causally related to melanoma.[23] Melanoma is most common on the back in men and on legs in women (areas of intermittent sun exposure). The risk appears to be strongly influenced by socioeconomic conditions rather than indoor versus outdoor occupations; it is more common in professional and administrative workers than unskilled workers.[24][25] Other factors are mutations in or total loss of tumor suppressor genes. Use of sunbeds (with deeply penetrating UVA rays) has been linked to the development of skin cancers, including melanoma.[26]
Possible significant elements in determining risk include the intensity and duration of sun exposure, the age at which sun exposure occurs, and the degree of skin pigmentation. Melanoma rates tend to be highest in countries settled by migrants from northern Europe that have a large amount of direct, intense sunlight that the skin of the settlers is not adapted to, most notably Australia. Exposure during childhood is a more important risk factor than exposure in adulthood. This is seen in migration studies in Australia.[27]
Having multiple severe sunburns increases the likelihood that future sunburns develop into melanoma due to cumulative damage.[14] The sun and tanning beds are the main sources of UV radiation that increase the risk for melanoma and living close to the equator increases exposure to UV radiation.[14]
Genetics
A number of rare mutations, which often run in families, greatly increase melanoma susceptibility. Several genes increase risks. Some rare genes have a relatively high risk of causing melanoma; some more common genes, such as a gene called MC1R that causes red hair, have a relatively lower elevated risk. Genetic testing can be used to search for the mutations.
One class of mutations affects the gene CDKN2A. An alternative reading frame mutation in this gene leads to the destabilization of p53, a transcription factor involved in apoptosis and in fifty percent of human cancers. Another mutation in the same gene results in a nonfunctional inhibitor of CDK4, a cyclin-dependent kinase that promotes cell division. Mutations that cause the skin condition xeroderma pigmentosum (XP) also increase melanoma susceptibility. Scattered throughout the genome, these mutations reduce a cell's ability to repair DNA. Both CDKN2A and XP mutations are highly penetrant (the chances of a carrier to express the phenotype is high).
Familial melanoma (FAMMM) is genetically heterogeneous,[15] and loci for familial melanoma appear on the chromosome arms 1p, 9p and 12q. Multiple genetic events have been related to melanoma's pathogenesis (disease development).[28] The multiple tumor suppressor 1 (CDKN2A/MTS1) gene encodes p16INK4a – a low-molecular weight protein inhibitor of cyclin-dependent protein kinases (CDKs) – which has been localised to the p21 region of human chromosome 9.[29] FAMMM is typically characterized by having 50 or more combined moles in addition to a family history of melanoma.[16] It is transmitted autosomal dominantly and mostly associated with the CDKN2A mutations.[16] People who have CDKN2A mutation associated FAMMM have a 38 fold increased risk of pancreatic cancer.[30]
Other mutations confer lower risk, but are more common in the population. People with mutations in the MC1R gene are two to four times more likely to develop melanoma than those with two wild-type (typical unaffected type) copies. MC1R mutations are very common; and all red-haired people have a mutated copy. Mutation of the MDM2 SNP309 gene is associated with increased risks for younger women.[31]
Fair- and red-haired people, persons with multiple atypical nevi or dysplastic nevi and persons born with giant congenital melanocytic nevi are at increased risk.[32]
A family history of melanoma greatly increases a person's risk because mutations in several genes have been found in melanoma-prone families.[33] People with a history of one melanoma are at increased risk of developing a second primary tumor.[34]
Fair skin is the result of having less melanin in the skin, which means there is less protection from UV radiation.[14] A family history could indicate a genetic predisposition to melanoma.[14]
Pathophysiology
The earliest stage of melanoma starts when melanocytes begin out-of-control growth. Melanocytes are found between the outer layer of the skin (the epidermis) and the next layer (the dermis). This early stage of the disease is called the radial growth phase, when the tumor is less than 1 mm thick. Because the cancer cells have not yet reached the blood vessels deeper in the skin, it is very unlikely that this early-stage melanoma will spread to other parts of the body. If the melanoma is detected at this stage, then it can usually be completely removed with surgery.
When the tumor cells start to move in a different direction – vertically up into the epidermis and into the papillary dermis – cell behaviour changes dramatically.[35]
The next step in the evolution is the invasive radial growth phase, in which individual cells start to acquire invasive potential. From this point on the melanoma is capable of spreading. The Breslow's depth of the lesion is usually less than 1 mm (0.04 in), while the Clark level is usually 2.
The vertical growth phase (VGP) following is the invasive melanoma. The tumor becomes able to grow into the surrounding tissue and can spread around the body through blood or lymph vessels. The tumor thickness is usually more than 1 mm (0.04 in), and the tumor involves the deeper parts of the dermis.
The host elicits an immunological reaction against the tumor during the VGP,[36] which is judged by the presence and activity of the tumor infiltrating lymphocytes (TILs). These cells sometimes completely destroy the primary tumor; this is called regression, which is the latest stage of development. In certain cases, the primary tumor is completely destroyed and only the metastatic tumor is discovered. About 40% of human melanomas contain activating mutations affecting the structure of the B-Raf protein, resulting in constitutive signaling through the Raf to MAP kinase pathway.[37]
An insult common to most cancers is damage to DNA.[38] UVA light mainly causes thymine dimers.[39] UVA also produces reactive oxygen species and these inflict other DNA damage, primarily single-strand breaks, oxidized pyrimidines and the oxidized purine 8-oxoguanine (a mutagenic DNA change) at 1/10th, 1/10th and 1/3rd the frequencies of UVA-induced thymine dimers, respectively.
If unrepaired, CPD photoproducts can lead to mutations by inaccurate translesion synthesis during DNA replication or repair. The most frequent mutations due to inaccurate synthesis past CPDs are cytosine to thymine (C>T) or CC>TT transition mutations. These are commonly referred to as UV fingerprint mutations, as they are the most specific mutation caused by UV, being frequently found in sun-exposed skin but rarely found in internal organs.[40] Errors in DNA repair of UV photoproducts, or inaccurate synthesis past these photoproducts, can also lead to deletions, insertions and chromosomal translocations.
The entire genomes of 25 melanomas were sequenced.[41] On average, about 80,000 mutated bases (mostly C>T transitions) and about 100 structural rearrangements were found per melanoma genome. This is much higher than the approximately 70 mutations across generations (parent to child).[42][43] Among the 25 melanomas, about 6,000 protein-coding genes had missense, nonsense, or splice site mutations. The transcriptomes of over 100 melanomas has also been sequenced and analyzed. Almost 70% of all human protein coding genes are expressed in melanoma. Most of these genes are also expressed in other normal and cancer tissues, with some 200 genes showing a more specific expression pattern in melanoma compared to other forms of cancer. Examples of melanoma specific genes are tyrosinase, MLANA, and PMEL.[44][45]
UV radiation causes damage to the DNA of cells, typically thymine dimerization, which when unrepaired can create mutations in the cell's genes. This strong mutagenic factor makes cutaneous melanoma the tumor type with the highest number of mutations.[46] When the cell divides, these mutations are propagated to new generations of cells. If the mutations occur in protooncogenes or tumor suppressor genes, the rate of mitosis in the mutation-bearing cells can become uncontrolled, leading to the formation of a tumor. Data from patients suggest that aberrant levels of activating transcription factor in the nucleus of melanoma cells are associated with increased metastatic activity of melanoma cells;[47][48][49] studies from mice on skin cancer tend to confirm a role for activating transcription factor-2 in cancer progression.[50][51]
Cancer stem cells may also be involved.[52]
Gene mutations
Large scale studies such as The Cancer Genome Atlas have characterized recurrent somatic alterations likely driving initiation and development of cutaneous melanoma.[53]
The most frequent mutation occurs in the 600th codon of BRAF (50% of cases). BRAF is normally involved in cell growth and this specific mutation renders the protein constitutively active and independent of normal physiological regulation, thus fostering tumor growth.[54] RAS genes (NRAS, HRAS and KRAS) are also recurrently mutated (30% of TCGA cases) and mutations in the 61st or 12th codons trigger oncogenic activity. Loss-of-function mutations often affect tumor suppressor genes such as NF1, TP53 and CDKN2A. BRAF, RAS and NF1 mutations are remarkably mutually-exclusive, as they occur in different subsets of patients. Assessment of mutation status can therefore improve patient stratification and inform targeted therapy with specific inhibitors.
In some cases (3-7%) mutated versions of BRAF and NRAS undergo copy number amplification.[53]
Diagnosis
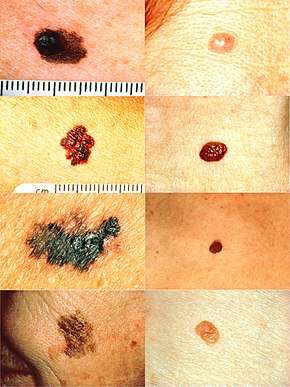
Looking at the area in question is the most common method of suspecting a melanoma.[55] Moles that are irregular in color or shape are typically treated as candidates. To detect melanomas (and increase survival rates), it is recommended to learn to recognize them (see "ABCDE" mnemonic), to regularly examine moles for changes (shape, size, color, itching or bleeding) and to consult a qualified physician when a candidate appears.[56][57]
However, many melanomas present as lesions smaller than 6 mm in diameter; and all melanomas are malignant when they first appear as a small dot. Physicians typically examine all moles, including those less than 6 mm in diameter. Seborrheic keratosis may meet some or all of the ABCD criteria, and can lead to false alarms. Doctors can generally distinguish seborrheic keratosis from melanoma upon examination, or with dermatoscopy.
Some advocate replacing enlarging with evolution. Certainly moles that change and evolve will be a concern. Alternatively, some practitioners prefer elevation. Elevation can help identify a melanoma, but lack of elevation does not mean that the lesion is not a melanoma. Most melanomas in the US are detected before they become elevated. By the time elevation is visible, they may have progressed to the more dangerous invasive stage.
In person inspection of suspicious skin lesions is more accurate than visual inspection of images of suspicious skin lesions.[58] When used by trained specialists, dermoscopy is more helpful to identify malignant lesions than use of the naked eye alone.[59]
_at_thigh_Case_01.jpg) Melanoma in skin biopsy with H&E stain – this case may represent superficial spreading melanoma.
Melanoma in skin biopsy with H&E stain – this case may represent superficial spreading melanoma. Lymph node with almost complete replacement by metastatic melanoma. The brown pigment is focal deposition of melanin.
Lymph node with almost complete replacement by metastatic melanoma. The brown pigment is focal deposition of melanin.
Ugly duckling
One method is the "ugly duckling sign".[60] Correlation of common lesion characteristics is made. Lesions that deviate from the common characteristics are labeled an "Ugly Duckling", and a further professional exam is required. The "Little Red Riding Hood" sign[60] suggests that individuals with fair skin and light-colored hair might have difficult-to-diagnose amelanotic melanomas. Extra care is required when examining such individuals, as they might have multiple melanomas and severely dysplastic nevi. A dermatoscope must be used to detect "ugly ducklings", as many melanomas in these individuals resemble non-melanomas or are considered to be "wolves in sheep's clothing".[61] These fair-skinned individuals often have lightly pigmented or amelanotic melanomas that do not present easy-to-observe color changes and variations. Their borders are often indistinct, complicating visual identification without a dermatoscope.
Amelanotic melanomas and melanomas arising in fair-skinned individuals are very difficult to detect, as they fail to show many of the characteristics in the ABCD rule, break the "Ugly Duckling" sign and are hard to distinguish from acne scarring, insect bites, dermatofibromas, or lentigines.
Biopsy
Following a visual examination and a dermatoscopic exam,[61] or in vivo diagnostic tools such as a confocal microscope, the doctor may biopsy the suspicious mole. A skin biopsy performed under local anesthesia is often required to assist in making or confirming the diagnosis and in defining severity. Elliptical excisional biopsies may remove the tumor, followed by histological analysis and Breslow scoring. Incisional biopsies such as punch biopsies are usually contraindicated in suspected melanomas, because of the possibility of sampling error[62] or local implantation causing misestimation of tumour thickness.[63][64] However, fears that such biopsies may increase the risk of metastatic disease seem unfounded.[65][66]
Total body photography, which involves photographic documentation of as much body surface as possible, is often used during follow-up for high-risk patients. The technique has been reported to enable early detection and provides a cost-effective approach (with any digital camera), but its efficacy has been questioned due to its inability to detect macroscopic changes.[55] The diagnosis method should be used in conjunction with (and not as a replacement for) dermoscopic imaging, with a combination of both methods appearing to give extremely high rates of detection.
Classification

Melanoma is divided into the following types:[67]
- Lentigo maligna
- Lentigo maligna melanoma
- Superficial spreading melanoma
- Acral lentiginous melanoma
- Mucosal melanoma
- Nodular melanoma
- Polypoid melanoma
- Desmoplastic melanoma
See also:[68]
Laboratory
Lactate dehydrogenase (LDH) tests are often used to screen for metastases, although many patients with metastases (even end-stage) have a normal LDH; extraordinarily high LDH often indicates metastatic spread of the disease to the liver.
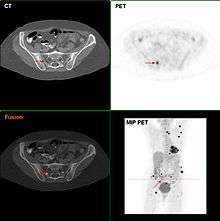
It is common for patients diagnosed with melanoma to have chest X-rays and an LDH test, and in some cases CT, MRI, PET, and/or PET/CT scans. Although controversial, sentinel lymph node biopsies and examination of the lymph nodes are also performed in patients to assess spread to the lymph nodes. A diagnosis of melanoma is supported by the presence of the S-100 protein marker.
HMB-45 is a monoclonal antibody that reacts against an antigen present in melanocytic tumors such as melanomas. It is used in anatomic pathology as a marker for such tumors. The antibody was generated to an extract of melanoma. It reacts positively against melanocytic tumors but not other tumors, thus demonstrating specificity and sensitivity. The antibody also reacts positively against junctional nevus cells but not intradermal nevi, and against fetal melanocytes but not normal adult melanocytes.
HMB-45 is nonreactive with almost all non-melanoma human malignancies, with the exception of rare tumors showing evidence of melanogenesis (e.g., pigmented schwannoma, clear cell sarcoma) or tumors associated with tuberous sclerosis complex (angiomyolipoma and lymphangiomyoma).
Staging
Further context on cancer staging is available at TNM.
Also of importance are the "Clark level" and "Breslow's depth", which refer to the microscopic depth of tumor invasion.[69]
Melanoma stages[70] and 5-year survival rates:

- Stage 0
- Melanoma in situ (Clark Level I), 99.9% survival.
- Stage I / II
- Invasive melanoma, 89–95% survival.
- T1a
- Less than 1.0 mm primary tumor thickness, without ulceration, and mitosis < 1/mm2.
- T1b
- Less than 1.0 mm primary tumor thickness, with ulceration or mitoses ≥ 1/mm2.
- T2a
- 1.01–2.0 mm primary tumor thickness, without ulceration.
- Stage II
- High risk melanoma, 45–79% survival
- T2b
- 1.01–2.0 mm primary tumor thickness, with ulceration
- T3a
- 2.01–4.0 mm primary tumor thickness, without ulceration
- T3b
- 2.01–4.0 mm primary tumor thickness, with ulceration
- T4a
- Greater than 4.0 mm primary tumor thickness, without ulceration
- T4b
- Greater than 4.0 mm primary tumor thickness, with ulceration
- Stage III
- Regional metastasis, 24–70% survival
- N1
- Single positive lymph
- N2
- Two to three positive lymph nodes or regional skin/in-transit metastasis
- N2
- Two to three positive lymph nodes or regional skin/in-transit metastasis
- N3
- Four positive lymph nodes or one lymph node and regional skin/in-transit metastases
- Stage IV
- Distant metastasis, 7–19% survival
- M1a
- Distant skin metastasis, normal LDH
- M1b
- Lung metastasis, normal LDH
- M1c
- Other distant metastasis or any distant metastasis with elevated LDH
Based upon AJCC five-year survival from initial melanoma diagnosis with proper treatment.
Prevention
Avoiding ultraviolet radiation
Minimizing exposure to sources of ultraviolet radiation (the sun and sunbeds),[71] following sun protection measures and wearing sun protective clothing (long-sleeved shirts, long trousers, and broad-brimmed hats) can offer protection.
Using artificial light for tanning was once believed to help prevent skin cancers, but it can actually lead to an increased incidence of melanomas.[72]
UV nail lamps, which are used in nail salons to dry nail polish, are another common and widespread source of UV radiation that could be avoided.[73][74] Although the risk of developing skin cancer through UV nail lamp use is low, it is still recommended to wear fingerless gloves and/or apply SPF 30 or greater sunscreen to the hands before using a UV nail lamp.[73][74]
The body uses UV light to generate vitamin D so there is a need to balance getting enough sunlight to maintain healthy vitamin D levels and reducing the risk of melanoma; it takes around a half hour of sunlight for the body to generate its vitamin D for the day and this is about the same amount of time it takes for fair-skinned people to get a sunburn. Exposure to sunlight can be intermittent instead of all at one time.[75]
Sunscreen
Sunscreen appears to be effective in preventing melanoma.[2][76] In the past, use of sunscreens with a sun protection factor (SPF) rating of 50 or higher on exposed areas were recommended; as older sunscreens more effectively blocked UVA with higher SPF.[77] Currently, newer sunscreen ingredients (avobenzone, zinc oxide, and titanium dioxide) effectively block both UVA and UVB even at lower SPFs. Sunscreen also protects against squamous cell carcinoma, another skin cancer.[78]
Concerns have been raised that sunscreen might create a false sense of security against sun damage.[79]
Treatment

Confirmation of the clinical diagnosis is done with a skin biopsy. This is usually followed up with a wider excision of the scar or tumor. Depending on the stage, a sentinel lymph node biopsy may be performed. Controversy exists around trial evidence for sentinel lymph node biopsy;[82] with unclear evidence of benefit as of 2015.[83] Treatment of advanced malignant melanoma is performed from a multidisciplinary approach.
Surgery
Excisional biopsies may remove the tumor, but further surgery is often necessary to reduce the risk of recurrence. Complete surgical excision with adequate surgical margins and assessment for the presence of detectable metastatic disease along with short- and long-term followup is standard. Often this is done by a wide local excision (WLE) with 1–2 cm (0.4–0.8 in) margins. Melanoma-in-situ and lentigo malignas are treated with narrower surgical margins, usually 0.2–0.5 cm (0.1–0.2 in). Many surgeons consider 0.5 cm (0.2 in) the standard of care for standard excision of melanoma-in-situ,[84] but 0.2 cm (0.1 in) margin might be acceptable for margin controlled surgery (Mohs surgery, or the double-bladed technique with margin control). The wide excision aims to reduce the rate of tumor recurrence at the site of the original lesion. This is a common pattern of treatment failure in melanoma. Considerable research has aimed to elucidate appropriate margins for excision with a general trend toward less aggressive treatment during the last decades.[85] A 2009 meta-analysis of randomized controlled trials found a small difference in survival rates favoring wide excision of primary cutaneous melanomas, but these results were not statistically significant.[86]
Mohs surgery has been reported with cure rate as low as 77%[87] and as high as 98.0% for melanoma-in-situ.[88] CCPDMA and the "double scalpel" peripheral margin controlled surgery is equivalent to Mohs surgery in effectiveness on this "intra-epithelial" type of melanoma.
Melanomas that spread usually do so to the lymph nodes in the area of the tumor before spreading elsewhere. Attempts to improve survival by removing lymph nodes surgically (lymphadenectomy) were associated with many complications, but no overall survival benefit. Recently, the technique of sentinel lymph node biopsy has been developed to reduce the complications of lymph node surgery while allowing assessment of the involvement of nodes with tumor.[89]
Biopsy of sentinel lymph nodes is a widely used procedure when treating cutaneous melanoma.[90][91]
Neither sentinel lymph node biopsy nor other diagnostic tests should be performed to evaluate early, thin melanoma, including melanoma in situ, T1a melanoma or T1b melanoma ≤ 0.5mm.[92] People with these conditions are unlikely to have the cancer spread to their lymph nodes or anywhere else and have a 5-year survival rate of 97%.[92] Because of these considerations, sentinel lymph node biopsy is considered unnecessary health care for them.[92] Furthermore, baseline blood tests and radiographic studies should not be performed only based on identifying this kind of melanoma, as there are more accurate tests for detecting cancer and these tests have high false-positive rates.[92] To potentially correct false positives, gene expression profiling may be used as auxiliary testing for ambiguous and small lesions.[93][94]
Sentinel lymph node biopsy is often performed, especially for T1b/T2+ tumors, mucosal tumors, ocular melanoma and tumors of the limbs. A process called lymphoscintigraphy is performed in which a radioactive tracer is injected at the tumor site to localize the sentinel node(s). Further precision is provided using a blue tracer dye, and surgery is performed to biopsy the node(s). Routine hematoxylin and eosin (H&E) and immunoperoxidase staining will be adequate to rule out node involvement. Polymerase chain reaction (PCR) tests on nodes, usually performed to test for entry into clinical trials, now demonstrate that many patients with a negative sentinel lymph node actually had a small number of positive cells in their nodes. Alternatively, a fine-needle aspiration biopsy may be performed and is often used to test masses.
If a lymph node is positive, depending on the extent of lymph node spread, a radical lymph node dissection will often be performed. If the disease is completely resected, the patient will be considered for adjuvant therapy. Excisional skin biopsy is the management of choice. Here, the suspect lesion is totally removed with an adequate (but minimal, usually 1 or 2 mm) ellipse of surrounding skin and tissue.[95] To avoid disruption of the local lymphatic drainage, the preferred surgical margin for the initial biopsy should be narrow (1 mm). The biopsy should include the epidermal, dermal, and subcutaneous layers of the skin. This enables the histopathologist to determine the thickness of the melanoma by microscopic examination. This is described by Breslow's thickness (measured in millimeters). However, for large lesions, such as suspected lentigo maligna, or for lesions in surgically difficult areas (face, toes, fingers, eyelids), a small punch biopsy in representative areas will give adequate information and will not disrupt the final staging or depth determination. In no circumstances should the initial biopsy include the final surgical margin (0.5 cm, 1.0 cm, or 2 cm), as a misdiagnosis can result in excessive scarring and morbidity from the procedure. A large initial excision will disrupt the local lymphatic drainage and can affect further lymphangiogram-directed lymphnode dissection. A small punch biopsy can be used at any time where for logistical and personal reasons a patient refuses more invasive excisional biopsy. Small punch biopsies are minimally invasive and heal quickly, usually without noticeable scarring.
Add on treatment
High-risk melanomas may require adjuvant treatment, although attitudes to this vary in different countries. In the United States, most patients in otherwise good health will begin up to a year of high-dose interferon treatment, which has severe side effects, but may improve the patient's prognosis slightly.[96] However, the British Association of Dermatologists guidelines on melanoma state that interferon is not recommended as a standard adjuvant treatment for melanoma.[97] A 2013 meta-analysis suggested that the addition of interferon alpha increased disease-free and overall survival for people with AJCC TNM stage II-III cutaneous melanoma.[98] A 2011 meta-analysis showed that interferon could lengthen the time before a melanoma comes back but increased survival by only 3% at 5 years. The unpleasant side effects also greatly decrease quality of life.[99]
In Europe, interferon is usually not used outside the scope of clinical trials.[100][101]
Metastatic melanomas can be detected by X-rays, CT scans, MRIs, PET and PET/CTs, ultrasound, LDH testing and photoacoustic detection.[102]
Chemotherapy
Chemotherapy drugs such as Dacarbazine have been the backbone of metastatic melanoma treatment since FDA approval in 1975 however, its efficacy in terms of survival has never been proven in an RCT.[103]
In people with locally advanced cutaneous malignancies and sarcoma, isolated limb infusion (ILI) has been found to be a minimally invasive and well-tolerated procedure for delivering regional chemotherapy.[104][105]
Targeted therapy
Melanoma cells have mutations that allow them to survive and grow indefinitely in the body.[103] Small-molecule targeted therapies work by blocking the genes involved in pathways for tumor proliferation and survival.[103] The main treatments are BRAF, C-Kit and NRAS inhibitors.[106] These inhibitors work to inhibit the downstream pathways involved in cell proliferation and tumour development due to specific gene mutations.[107] People can be treated with small-molecule targeted inhibitors if they are positive for the specific mutation.[103] BRAF inhibitors, such as vemurafenib and dabrafenib and a MEK inhibitor trametinib are the most effective, approved treatments for BRAF positive melanoma.[108][103] Melanoma tumors can develop resistance during therapy which can make therapy no longer effective, but combining the use of BRAF and MEK inhibitors may create a fast and lasting melanoma therapy response.[109]
A number of treatments improve survival over traditional chemotherapy.[103] Biochemotherapy (chemotherapy with cytokines IL-2 and IFN-α) combined with BRAF inhibitors improved survival for people with BRAF positive melanoma.[103] Biochemotherapy alone did not improve overall survival and had higher toxicity than chemotherapy.[103] Combining multiple chemotherapy agents (polychemotherapy) did not improve survival over monochemotherapy.[103]
Immunotherapy
Immunotherapy is aimed at stimulating the person's immune system against the tumor, by enhancing the body's own ability to recognize and kill cancer cells.[110] The current approach to treating melanoma with immunotherapy includes three broad categories of treatments including cytokines, immune check point inhibitors, and adoptive cell transfer.[110] These treatment options are most often used in people with metastatic melanoma and significantly improves overall survival.[103] However, these treatments are often costly. For example, one immune check point inhibitor treatment, pembrolizumab, costs $10,000 to US$12,000 for a single dose administered every 3 weeks.[111]
Cytokine therapies used for melanoma include IFN-a and IL-2.[112] IL-2 (Proleukin) was the first new therapy approved (1990 Europe, 1992 USA) for the treatment of metastatic melanoma in 20 years. IL-2 may offer the possibility of a complete and long-lasting remission in this disease in a small percentage of people with melanoma.[113] Intralesional IL-2 for in-transit metastases has a high complete response rate ranging from 40 to 100%.[108] Similarly, IFN-a has shown only modest survival benefits and high toxicity, limiting its use as a stand-alone therapy.[103][112]
Immune check point inhibitors include anti-CTLA-4 monoclonal antibodies (ipilimumab and tremelimumab), toll-like receptor (TLR) agonists, CD40 agonists, anti-PD-1 (pembrolizumab, pidilizumab, and nivolumab) and PD-L1 antibodies.[110][112] Evidence suggests that anti-PD-1 antibodies are more effective than anti-CTLA4 antibodies with less systemic toxicity.[103] A therapeutic approach that includes the combination of different therapies improves overall survival and progression-free survival compared to treatment with the separate immunotherapy drugs alone.[103]
Ongoing research is looking at treatment by adoptive cell transfer.[114] Adoptive cell transfer refers to the application of pre-stimulated, modified T cells or dendritic cells and is presently used to minimize complications from graft-versus-host disease.[112][115]
Lentigo maligna
Standard excision is still being done by most surgeons. Unfortunately, the recurrence rate is exceedingly high (up to 50%). This is due to the ill-defined visible surgical margin, and the facial location of the lesions (often forcing the surgeon to use a narrow surgical margin). The narrow surgical margin used, combined with the limitation of the standard "bread-loafing" technique of fixed tissue histology – result in a high "false negative" error rate, and frequent recurrences. Margin control (peripheral margins) is necessary to eliminate the false negative errors. If bread loafing is used, distances from sections should approach 0.1 mm to assure that the method approaches complete margin control. A meta-analysis of the literature in 2014 found no randomized controlled trials of surgical interventions to treat lentigo maligna or melanoma in-situ, even though surgery is the most widely used treatment.[116]
Mohs surgery has been done with cure rate reported to be as low as 77%,[87] and as high as 95% by another author.[88] The "double scalpel" peripheral margin controlled excision method approximates the Mohs method in margin control, but requires a pathologist intimately familiar with the complexity of managing the vertical margin on the thin peripheral sections and staining methods.[117]
Some melanocytic nevi, and melanoma-in-situ (lentigo maligna) have resolved with an experimental treatment, imiquimod (Aldara) topical cream, an immune enhancing agent. Some dermasurgeons are combining the 2 methods: surgically excising the cancer and then treating the area with Aldara cream postoperatively for three months. While some studies have suggested the adjuvant use of topical tazarotene, the current evidence is insufficient to recommend it and suggests that it increases topical inflammation, leading to lower patient compliance.[116]
Radiation
Radiation therapy is often used after surgical resection for patients with locally or regionally advanced melanoma or for patients with unresectable distant metastases. Kilovoltage x-ray beams are often used for these treatments and have the property of the maximum radiation dose occurring close to the skin surface.[118] It may reduce the rate of local recurrence but does not prolong survival.[119] Radioimmunotherapy of metastatic melanoma is currently under investigation. Radiotherapy has a role in the palliation of metastatic melanoma.[120]
Prognosis
Factors that affect prognosis include:
- tumor thickness in millimeters (Breslow's depth),
- depth related to skin structures (Clark level),
- type of melanoma,
- presence of ulceration,
- presence of lymphatic/perineural invasion,
- presence of tumor-infiltrating lymphocytes (if present, prognosis is better),
- location of lesion,
- presence of satellite lesions, and
- presence of regional or distant metastasis.[121]
Certain types of melanoma have worse prognoses but this is explained by their thickness. Less invasive melanomas even with lymph node metastases carry a better prognosis than deep melanomas without regional metastasis at time of staging. Local recurrences tend to behave similarly to a primary unless they are at the site of a wide local excision (as opposed to a staged excision or punch/shave excision) since these recurrences tend to indicate lymphatic invasion.
When melanomas have spread to the lymph nodes, one of the most important factors is the number of nodes with malignancy. Extent of malignancy within a node is also important; micrometastases in which malignancy is only microscopic have a more favorable prognosis than macrometastases. In some cases micrometastases may only be detected by special staining, and if malignancy is only detectable by a rarely employed test known as the polymerase chain reaction (PCR), the prognosis is better. Macrometastases in which malignancy is clinically apparent (in some cases cancer completely replaces a node) have a far worse prognosis, and if nodes are matted or if there is extracapsular extension, the prognosis is worse still. In addition to these variables, expression levels and copy number variations of a number of relevant genes may be used to support assessment of malignant melanoma prognosis.[93][94]
When there is distant metastasis, the cancer is generally considered incurable. The five-year survival rate is less than 10%.[70] The median survival is 6–12 months. Treatment is palliative, focusing on life extension and quality of life. In some cases, patients may live many months or even years with metastatic melanoma (depending on the aggressiveness of the treatment). Metastases to skin and lungs have a better prognosis. Metastases to brain, bone and liver are associated with a worse prognosis. Survival is better with metastasis in which the location of the primary tumor is unknown.[122]
There is not enough definitive evidence to adequately stage, and thus give a prognosis for, ocular melanoma and melanoma of soft parts, or mucosal melanoma (e.g., rectal melanoma), although these tend to metastasize more easily. Even though regression may increase survival, when a melanoma has regressed, it is impossible to know its original size and thus the original tumor is often worse than a pathology report might indicate.
About 200 genes are prognostic in melanoma, with both unfavorable genes where high expression is correlated to poor survival and favorable genes where high expression is associated with longer survival times. Examples of unfavorable genes are MCM6 and TIMELESS; an example of a favorable gene is WIPI1.[44][45]
Epidemiology
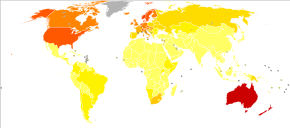
Globally, in 2012, melanoma occurred in 232,000 people and resulted in 55,000 deaths.[2] Australia and New Zealand have the highest rates of melanoma in the world.[2] It has become more common in the last 20 years in areas that are mostly Caucasian.[2]
The rate of melanoma has increased in the recent years, but it is not clear to what extent changes in behavior, in the environment, or in early detection are involved.[124]
Australia
Australia has a very high – and increasing – rate of melanoma. In 2012, deaths from melanoma occurred in 7.3–9.8 per 100,000 population. In Australia, melanoma is the third most common cancer in either sex; indeed, its incidence is higher than for lung cancer, although the latter accounts for more deaths. It is estimated that in 2012, more than 12,000 Australians were diagnosed with melanoma: given Australia's modest population, this is better expressed as 59.6 new cases per 100,000 population per year; >1 in 10 of all new cancer cases were melanomas.[125] Melanoma incidence in Australia is matter of significance, for the following reasons:
- Australian melanoma incidence has increased by more than 30 per cent between 1991 and 2009.
- Australian melanoma age-standardised incidence rates were, as of 2008, at least 12 times higher than the world average.
- Australian melanoma incidence is, by some margin, the highest in the world.
- Overall age-standardised cancer incidence in Australia is the highest in the world, and this is attributable to melanoma alone. Age-standardised overall cancer incidence is similar to New Zealand, but there is a statistically-significant difference between Australia and all other parts of the developed world including North America, Western Europe, and the Mediterranean.
United States
In the United States about 9,000 people die from melanoma a year.[126] In 2011 it affected 19.7 per 100,000, and resulted in death in 2.7 per 100,000.[126]
In 2013:
- 71,943 people in the United States were diagnosed with melanomas of the skin, including 42,430 men and 29,513 women.
- 9,394 people in the United States died from melanomas of the skin, including 6,239 men and 3,155 women.[127]
The American Cancer Society's estimates for melanoma incidence in the United States for 2017 are:
- About 87,110 new melanomas will be diagnosed (about 52,170 in men and 34,940 in women).
- About 9,730 people are expected to die of melanoma (about 6,380 men and 3,350 women).
Melanoma is more than 20 times more common in whites than in African Americans. Overall, the lifetime risk of getting melanoma is about 2.5% (1 in 40) for whites, 0.1% (1 in 1,000) for African Americans, and 0.5% (1 in 200) for Hispanics.
The risk of melanoma increases as people age. The average age of people when the disease is diagnosed is 63.[128]
History
Although melanoma is not a new disease, evidence for its occurrence in antiquity is rather scarce. However, one example lies in a 1960s examination of nine Peruvian mummies, radiocarbon dated to be approximately 2400 years old, which showed apparent signs of melanoma: melanotic masses in the skin and diffuse metastases to the bones.[129]
John Hunter is reported to be the first to operate on metastatic melanoma in 1787. Although not knowing precisely what it was, he described it as a "cancerous fungous excrescence". The excised tumor was preserved in the Hunterian Museum of the Royal College of Surgeons of England. It was not until 1968 that microscopic examination of the specimen revealed it to be an example of metastatic melanoma.[130]
The French physician René Laennec was the first to describe melanoma as a disease entity. His report was initially presented during a lecture for the Faculté de Médecine de Paris in 1804 and then published as a bulletin in 1806.[131]
The first English-language report of melanoma was presented by an English general practitioner from Stourbridge, William Norris in 1820.[132] In his later work in 1857 he remarked that there is a familial predisposition for development of melanoma (Eight Cases of Melanosis with Pathological and Therapeutical Remarks on That Disease). Norris was also a pioneer in suggesting a link between nevi and melanoma and the possibility of a relationship between melanoma and environmental exposures, by observing that most of his patients had pale complexions.[133] He also described that melanomas could be amelanotic and later showed the metastatic nature of melanoma by observing that they can disseminate to other visceral organs.
The first formal acknowledgment of advanced melanoma as untreatable came from Samuel Cooper in 1840. He stated that the only chance for a cure depends upon the early removal of the disease (i.e., early excision of the malignant mole) ...'[134]
More than one and a half centuries later this situation remains largely unchanged.
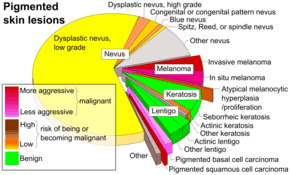
Terminology
The word melanoma came to English from 19th-century New Latin[135] and uses combining forms derived from ancient Greek roots: melano- (denoting melanin) + -oma (denoting a tissue mass and especially a neoplasm), in turn from Greek μέλας melas, "dark",[136] and -ωμα oma, "process". The word melanoma has a long history of being used in a broader sense to refer to any melanocytic tumor, benign or malignant but usually malignant,[137][138] but today the narrower sense referring only to malignant types has become so dominant that benign tumors are usually not called melanomas anymore and the word melanoma is now usually taken to mean malignant melanoma unless otherwise specified. Terms such as "benign melanocytic tumor" unequivocally label the benign types, and modern histopathologic tumor classifications used in medicine do not use the word for benign tumors.
Research
Pharmacotherapy research for unresectable or metastatic malignant melanoma is ongoing.[139]
Targeted therapies
In clinical research, adoptive cell therapy and gene therapy, are being tested.[140]
Two kinds of experimental treatments developed at the National Cancer Institute (NCI), have been used in metastatic melanoma with tentative success.[35]
The first treatment involves adoptive cell therapy (ACT) using TILs immune cells (tumor-infiltrating lymphocytes) isolated from a person's own melanoma tumor.[108] These cells are grown in large numbers in a laboratory and returned to the patient after a treatment that temporarily reduces normal T cells in the patient's body. TIL therapy following lymphodepletion can result in durable complete response in a variety of setups.[141][142]
The second treatment, adoptive transfer of genetically altered autologous lymphocytes, depends on delivering genes that encode so called T cell receptors (TCRs), into patient's lymphocytes.[108] After that manipulation lymphocytes recognize and bind to certain molecules found on the surface of melanoma cells and kill them.[143]
A cancer vaccine showed modest benefit in late-stage testing in 2009 against melanoma.[144][145]
BRAF inhibitors
About 60% of melanomas contain a mutation in the B-Raf gene. Early clinical trials suggested that B-Raf inhibitors including Plexxicon's vemurafenib could lead to substantial tumor regression in a majority of patients if their tumor contain the B-Raf mutation.[146] In June 2011, a large clinical trial confirmed the positive findings from those earlier trials.[147][148]
In August 2011 Vemurafenib received FDA approval for the treatment of late-stage melanoma. In May 2013 the US FDA approved dabrafenib as a single agent treatment for patients with BRAF V600E mutation-positive advanced melanoma.[149]
Some researchers believe that combination therapies that simultaneously block multiple pathways may improve efficacy by making it more difficult for the tumor cells to mutate before being destroyed. In October 2012 a study reported that combining Dabrafenib with a MEK inhibitor trametinib led to even better outcomes. Compared to Dabrafenib alone, progression-free survival was increased to 41% from 9%, and the median progression-free survival increased to 9.4 months versus 5.8 months. Some side effects were, however, increased in the combined study.[150][151]
In January 2014, the FDA approved the combination of dabrafenib and trametinib for the treatment of patients with BRAF V600E/K-mutant metastatic melanoma.[152]
Eventual resistance to BRAF and MEK inhibitors may be due to a cell surface protein known as EphA2 which is now being investigated.[153]
Ipilimumab
At the American Society of Clinical Oncology Conference in June 2010, the Bristol-Myers Squibb pharmaceutical company reported the clinical findings of their drug ipilimumab. The study found an increase in median survival from 6.4 to 10 months in patients with advanced melanomas treated with the monoclonal ipilimumab, versus an experimental vaccine. It also found a one-year survival rate of 25% in the control group using the vaccine, 44% in the vaccine and ipilimumab group, and 46% in the group treated with ipilimumab alone.[154] However, some have raised concerns about this study for its use of the unconventional control arm, rather than comparing the drug against a placebo or standard treatment.[155][156] The criticism was that although Ipilimumab performed better than the vaccine, the vaccine has not been tested before and may be causing toxicity, making the drug appear better by comparison.
Ipilimumab was approved by the FDA in March 2011 to treat patients with late-stage melanoma that has spread or cannot be removed by surgery.[157][158][159]
In June 2011, a clinical trial of ipilimumab plus dacarbazine combined this immune system booster with the standard chemotherapy drug that targets cell division. It showed an increase in median survival for these late stage patients to 11 months instead of the 9 months normally seen. Researchers were also hopeful of improving the five year survival rate, though serious adverse side-effects were seen in some patients. A course of treatment costs $120,000. The drug's brandname is Yervoy.[147][160]
Surveillance methods
Advances in high resolution ultrasound scanning have enabled surveillance of metastatic burden to the sentinel lymph nodes.[161] The Screening and Surveillance of Ultrasound in Melanoma trial (SUNMEL) is evaluating ultrasound as an alternative to invasive surgical methods.[162]
Oncolytic virotherapy
In some countries oncolytic virotherapy methods are studied and used to treat melanoma. Oncolytic virotherapy is a promising branch of virotherapy, where oncolytic viruses are used to treat diseases; viruses can increase metabolism, reduce anti-tumor immunity and disorganize vasculature.[163] Talimogene laherparepvec (T-VEC) (which is a herpes simplex virus type 1–derived oncolytic immunotherapy), was shown to be useful against metastatic melanoma in 2015 with an increased survival of 4.4 months.[164][9]
References
- "Melanoma Treatment–for health professionals (PDQ®)". National Cancer Institute. June 26, 2015. Archived from the original on 4 July 2015. Retrieved 30 June 2015.
- World Cancer Report 2014 (PDF). World Health Organization. 2014. pp. Chapter 5.14. ISBN 978-9283204299. Archived (PDF) from the original on 2014-05-30.
- Goldstein BG, Goldstein AO (April 2001). "Diagnosis and management of malignant melanoma". American Family Physician. 63 (7): 1359–68, 1374. PMID 11310650.
- "SEER Stat Fact Sheets: Melanoma of the Skin". NCI. Archived from the original on 2014-07-06.
- GBD 2015 Disease and Injury Incidence and Prevalence, Collaborators. (8 October 2016). "Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015". Lancet. 388 (10053): 1545–1602. doi:10.1016/S0140-6736(16)31678-6. PMC 5055577. PMID 27733282.
- GBD 2015 Mortality and Causes of Death, Collaborators. (8 October 2016). "Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: a systematic analysis for the Global Burden of Disease Study 2015". Lancet. 388 (10053): 1459–1544. doi:10.1016/s0140-6736(16)31012-1. PMC 5388903. PMID 27733281.
- Kanavy HE, Gerstenblith MR (December 2011). "Ultraviolet radiation and melanoma". Semin Cutan Med Surg. 30 (4): 222–28. doi:10.1016/j.sder.2011.08.003. PMID 22123420.
- Azoury SC, Lange JR (October 2014). "Epidemiology, risk factors, prevention, and early detection of melanoma". The Surgical Clinics of North America. 94 (5): 945–62, vii. doi:10.1016/j.suc.2014.07.013. PMID 25245960.
- Syn NL, Teng MW, Mok TS, Soo RA (December 2017). "De-novo and acquired resistance to immune checkpoint targeting". The Lancet. Oncology. 18 (12): e731–e741. doi:10.1016/s1470-2045(17)30607-1. PMID 29208439.
- "CDC - What Are the Symptoms of Skin Cancer?". www.cdc.gov. 2018-06-26. Retrieved 2019-02-01.
- Daniel Jensen J, Elewski BE (February 2015). "The ABCDEF Rule: Combining the "ABCDE Rule" and the "Ugly Duckling Sign" in an Effort to Improve Patient Self-Screening Examinations". The Journal of Clinical and Aesthetic Dermatology. 8 (2): 15. PMC 4345927. PMID 25741397.
- "The EFG of Nodular Melanomas | MoleMap New Zealand". The EFG of Nodular Melanomas | MoleMap New Zealand. Retrieved 2019-02-01.
- Fiddler IJ (October 1995). "Melanoma Metastasis". Cancer Control. 2 (5): 398–404. doi:10.1177/107327489500200503. PMID 10862180.
- "Melanoma Risk factors". Mayo Clinic. Archived from the original on 2017-04-10. Retrieved 2017-04-10.
- Greene MH (December 1999). "The genetics of hereditary melanoma and nevi. 1998 update". Cancer. 86 (11 Suppl): 2464–77. doi:10.1002/(SICI)1097-0142(19991201)86:11+<2464::AID-CNCR3>3.0.CO;2-F. PMID 10630172.
- Goydos JS, Shoen SL (2016). "Acral Lentiginous Melanoma". Cancer Treatment and Research. 167: 321–9. doi:10.1007/978-3-319-22539-5_14. ISBN 978-3-319-22538-8. PMID 26601870.
- Perkins A, Duffy RL (June 2015). "Atypical moles: diagnosis and management". American Family Physician. 91 (11): 762–7. PMID 26034853.
- Boniol M, Autier P, Boyle P, Gandini S (July 2012). "Cutaneous melanoma attributable to sunbed use: systematic review and meta-analysis". BMJ (Clinical Research Ed.). 345: e4757. doi:10.1136/bmj.e4757. PMC 3404185. PMID 22833605.
- WHO International Agency for Research on Cancer Monograph Working Group (August 2009). "A Review of Human Carcinogens – Part D: Radiation". The Lancet Oncology. 10 (8): 751–52. doi:10.1016/S1470-2045(09)70213-X. PMID 19655431.
- Sanlorenzo M, Wehner MR, Linos E, Kornak J, Kainz W, Posch C, Vujic I, Johnston K, Gho D, Monico G, McGrath JT, Osella-Abate S, Quaglino P, Cleaver JE, Ortiz-Urda S (January 2015). "The risk of melanoma in airline pilots and cabin crew: a meta-analysis". JAMA Dermatology. 151 (1): 51–8. doi:10.1001/jamadermatol.2014.1077. PMC 4482339. PMID 25188246.
- Rünger TM, Farahvash B, Hatvani Z, Rees A (January 2012). "Comparison of DNA damage responses following equimutagenic doses of UVA and UVB: a less effective cell cycle arrest with UVA may render UVA-induced pyrimidine dimers more mutagenic than UVB-induced ones". Photochem. Photobiol. Sci. 11 (1): 207–15. doi:10.1039/c1pp05232b. PMID 22005748.
- Wang S, Setlow R, Berwick M, Polsky D, Marghoob A, Kopf A, Bart R (2001). "Ultraviolet A and melanoma: a review". J Am Acad Dermatol. 44 (5): 837–46. doi:10.1067/mjd.2001.114594. PMID 11312434.
- Oliveria S, Saraiya M, Geller A, Heneghan M, Jorgensen C (2006). "Sun exposure and risk of melanoma". Arch Dis Child. 91 (2): 131–38. doi:10.1136/adc.2005.086918. PMC 2082713. PMID 16326797.
- Lee J, Strickland D (1980). "Malignant melanoma: social status and outdoor work". Br J Cancer. 41 (5): 757–63. doi:10.1038/bjc.1980.138. PMC 2010319. PMID 7426301.
- Pion IA, Rigel DS, Garfinkel L, Silverman MK, Kopf AW (January 1995). "Occupation and the risk of malignant melanoma". Cancer. 75 (2 Suppl): 637–44. doi:10.1002/1097-0142(19950115)75:2+<637::aid-cncr2820751404>3.0.co;2-#. PMID 7804988.
- "WHO | The World Health Organization recommends that no person under 18 should use a sunbed". WHO. Archived from the original on June 16, 2009.
- Khlat M, Vail A, Parkin M, Green A (1992). "Mortality from melanoma in migrants to Australia: variation by age at arrival and duration of stay". Am J Epidemiol. 135 (10): 1103–13. doi:10.1093/oxfordjournals.aje.a116210. PMID 1632422.
- Halachmi S, Gilchrest BA (March 2001). "Update on genetic events in the pathogenesis of melanoma". Current Opinion in Oncology. 13 (2): 129–36. doi:10.1097/00001622-200103000-00008. PMID 11224711.
- CDKN2A cyclin-dependent kinase inhibitor 2A (melanoma, p16, inhibits CDK4) Archived 2004-11-17 at the Wayback Machine from Entrez Gene
- Soura E, Eliades PJ, Shannon K, Stratigos AJ, Tsao H (March 2016). "Hereditary melanoma: Update on syndromes and management: Genetics of familial atypical multiple mole melanoma syndrome". Journal of the American Academy of Dermatology. 74 (3): 395–407, quiz 408–10. doi:10.1016/j.jaad.2015.08.038. PMC 4761105. PMID 26892650.
- Firoz EF, Warycha M, Zakrzewski J, Pollens D, Wang G, Shapiro R, Berman R, Pavlick A, Manga P, Ostrer H, Celebi JT, Kamino H, Darvishian F, Rolnitzky L, Goldberg JD, Osman I, Polsky D (April 2009). "Association of MDM2 SNP309, age of onset, and gender in cutaneous melanoma". Clinical Cancer Research. 15 (7): 2573–80. doi:10.1158/1078-0432.CCR-08-2678. PMC 3881546. PMID 19318491.
- Bliss J, Ford D, Swerdlow A, Armstrong B, Cristofolini M, Elwood J, Green A, Holly E, Mack T, MacKie R (1995). "Risk of cutaneous melanoma associated with pigmentation characteristics and freckling: systematic overview of 10 case-control studies. The International Melanoma Analysis Group (IMAGE)". Int J Cancer. 62 (4): 367–76. doi:10.1002/ijc.2910620402. PMID 7635560.
- Miller A, Mihm M (2006). "Melanoma". N Engl J Med. 355 (1): 51–65. doi:10.1056/NEJMra052166. PMID 16822996.
- Rhodes A, Weinstock M, Fitzpatrick T, Mihm M, Sober A (1987). "Risk factors for cutaneous melanoma. A practical method of recognizing predisposed individuals". JAMA. 258 (21): 3146–54. doi:10.1001/jama.258.21.3146. PMID 3312689.
- Hershkovitz L, Schachter J, Treves AJ, Besser MJ (2010). "Focus on adoptive T cell transfer trials in melanoma". Clin. Dev. Immunol. 2010: 260267. doi:10.1155/2010/260267. PMC 3018069. PMID 21234353.
- "ASCO Annual Meeting Proceedings Part I. Abstract: Protective effect of a brisk tumor infiltrating lymphocyte infiltrate in melanoma: An EORTC melanoma group study". Journal of Clinical Oncology. 25 (18S): 8519. 2007. Archived from the original on 2011-07-25.
- Davies MA, Samuels Y (October 2010). "Analysis of the genome to personalize therapy for melanoma". Oncogene. 29 (41): 5545–55. doi:10.1038/onc.2010.323. PMC 3169242. PMID 20697348.
- Barrett, J. Carl (1991). "Mutagenesis and Carcinogenesis". In Brugge, Joan; Curran, Tom; Harlow, Ed; McCormick, Frank (eds.). Origins of Human Cancer. Cold Spring Harbor Press. ISBN 0-87969-404-1 – via Internet Archive.
- Sage E, Girard PM, Francesconi S (January 2012). "Unravelling UVA-induced mutagenesis". Photochem. Photobiol. Sci. 11 (1): 74–80. doi:10.1039/c1pp05219e. PMID 21901217.
- Budden T, Bowden NA (2013). "The Role of Altered Nucleotide Excision Repair and UVB-Induced DNA Damage in Melanomagenesis". Int J Mol Sci. 14 (1): 1132–51. doi:10.3390/ijms14011132. PMC 3565312. PMID 23303275.
- Berger MF, Hodis E, Heffernan TP, Deribe YL, Lawrence MS, Protopopov A, Ivanova E, Watson IR, Nickerson E, Ghosh P, Zhang H, Zeid R, Ren X, Cibulskis K, Sivachenko AY, Wagle N, Sucker A, Sougnez C, Onofrio R, Ambrogio L, Auclair D, Fennell T, Carter SL, Drier Y, Stojanov P, Singer MA, Voet D, Jing R, Saksena G, Barretina J, Ramos AH, Pugh TJ, Stransky N, Parkin M, Winckler W, Mahan S, Ardlie K, Baldwin J, Wargo J, Schadendorf D, Meyerson M, Gabriel SB, Golub TR, Wagner SN, Lander ES, Getz G, Chin L, Garraway LA (May 2012). "Melanoma genome sequencing reveals frequent PREX2 mutations". Nature. 485 (7399): 502–06. Bibcode:2012Natur.485..502B. doi:10.1038/nature11071. PMC 3367798. PMID 22622578.
- Roach JC, Glusman G, Smit AF, et al. (April 2010). "Analysis of genetic inheritance in a family quartet by whole-genome sequencing". Science. 328 (5978): 636–39. Bibcode:2010Sci...328..636R. doi:10.1126/science.1186802. PMC 3037280. PMID 20220176.
- Campbell CD, Chong JX, Malig M, et al. (November 2012). "Estimating the human mutation rate using autozygosity in a founder population". Nat. Genet. 44 (11): 1277–81. doi:10.1038/ng.2418. PMC 3483378. PMID 23001126.
- "The human pathology proteome in melanoma – The Human Protein Atlas". www.proteinatlas.org. Retrieved 2017-10-02.
- Uhlen M, Zhang C, Lee S, Sjöstedt E, Fagerberg L, Bidkhori G, Benfeitas R, Arif M, Liu Z, Edfors F, Sanli K, von Feilitzen K, Oksvold P, Lundberg E, Hober S, Nilsson P, Mattsson J, Schwenk JM, Brunnström H, Glimelius B, Sjöblom T, Edqvist PH, Djureinovic D, Micke P, Lindskog C, Mardinoglu A, Ponten F (August 2017). "A pathology atlas of the human cancer transcriptome". Science. 357 (6352): eaan2507. doi:10.1126/science.aan2507. PMID 28818916.
- Ellrott, Kyle; Bailey, Matthew H.; Saksena, Gordon; Covington, Kyle R.; Kandoth, Cyriac; Stewart, Chip; Hess, Julian; Ma, Singer; Chiotti, Kami E. (March 2018). "Scalable Open Science Approach for Mutation Calling of Tumor Exomes Using Multiple Genomic Pipelines". Cell Systems. 6 (3): 271–281.e7. doi:10.1016/j.cels.2018.03.002. PMC 6075717. PMID 29596782.
- Leslie MC, Bar-Eli M (January 2005). "Regulation of gene expression in melanoma: new approaches for treatment". J. Cell. Biochem. 94 (1): 25–38. doi:10.1002/jcb.20296. PMID 15523674.
- Bhoumik A, Singha N, O'Connell MJ, Ronai ZA (June 2008). "Regulation of TIP60 by ATF2 modulates ATM activation". J. Biol. Chem. 283 (25): 17605–14. doi:10.1074/jbc.M802030200. PMC 2427333. PMID 18397884.
- Bhoumik A, Jones N, Ronai Z (March 2004). "Transcriptional switch by activating transcription factor 2-derived peptide sensitizes melanoma cells to apoptosis and inhibits their tumorigenicity". Proc. Natl. Acad. Sci. U.S.A. 101 (12): 4222–27. Bibcode:2004PNAS..101.4222B. doi:10.1073/pnas.0400195101. PMC 384722. PMID 15010535.
- Vlahopoulos SA, Logotheti S, Mikas D, Giarika A, Gorgoulis V, Zoumpourlis V (April 2008). "The role of ATF-2 in oncogenesis". BioEssays. 30 (4): 314–27. doi:10.1002/bies.20734. PMID 18348191.
- Huang Y, Minigh J, Miles S, Niles RM (2008). "Retinoic acid decreases ATF-2 phosphorylation and sensitizes melanoma cells to taxol-mediated growth inhibition". J Mol Signal. 3: 3. doi:10.1186/1750-2187-3-3. PMC 2265711. PMID 18269766.
- Parmiani, G (11 March 2016). "Melanoma Cancer Stem Cells: Markers and Functions". Cancers. 8 (3): 34. doi:10.3390/cancers8030034. PMC 4810118. PMID 26978405.
- Akbani, Rehan; Akdemir, Kadir C.; Aksoy, B. Arman; Albert, Monique; Ally, Adrian; Amin, Samirkumar B.; Arachchi, Harindra; Arora, Arshi; Auman, J. Todd (June 2015). "Genomic Classification of Cutaneous Melanoma". Cell. 161 (7): 1681–1696. doi:10.1016/j.cell.2015.05.044. PMC 4580370. PMID 26091043.
- Ascierto, Paolo A; Kirkwood, John M; Grob, Jean-Jacques; Simeone, Ester; Grimaldi, Antonio M; Maio, Michele; Palmieri, Giuseppe; Testori, Alessandro; Marincola, Francesco M (December 2012). "The role of BRAF V600 mutation in melanoma". Journal of Translational Medicine. 10 (1): 85. doi:10.1186/1479-5876-10-85. ISSN 1479-5876. PMC 3391993. PMID 22554099.
- Wurm EM, Soyer HP (October 2010). "Scanning for melanoma". Australian Prescriber (33): 150–55. Archived from the original on 2010-10-19.
- "Prevention: ABCD's of Melanoma". American Melanoma Foundation. Archived from the original on 2003-04-23.
- Friedman R, Rigel D, Kopf A (1985). "Early detection of malignant melanoma: the role of physician examination and self-examination of the skin". CA Cancer J Clin. 35 (3): 130–51. doi:10.3322/canjclin.35.3.130. PMID 3921200.
- Group, Cochrane Skin Cancer Diagnostic Test Accuracy; Williams, Hywel C.; Walter, Fiona M.; Godfrey, Kathie; Davenport, Clare; Takwoingi, Yemisi; Bayliss, Susan E.; Fawzy, Monica; Abbott, Rachel (2018). "Visual inspection for diagnosing cutaneous melanoma in adults". Cochrane Database of Systematic Reviews. 12 (12): CD013194. doi:10.1002/14651858.CD013194. ISSN 1465-1858. PMC 6492463. PMID 30521684.
- Dinnes, Jacqueline (December 2018). "Dermoscopy, with and without visual inspection, for diagnosing melanoma in adults". Cochrane Database of Systematic Reviews. doi:10.1002/14651858.CD011902.pub2. PMID 30521682.
- Mascaro JM, Mascaro JM (November 1998). "The dermatologist's position concerning nevi: a vision ranging from "the ugly duckling" to "little red riding hood"". Arch Dermatol. 134 (11): 1484–85. doi:10.1001/archderm.134.11.1484. PMID 9828892.
- "Introduction to Dermoscopy". DermNet New Zealand. Archived from the original on 2009-05-07.
- Montgomery BD, Sadler GM (January 2009). "Punch biopsy of pigmented lesions is potentially hazardous". Can Fam Physician. 55 (1): 24. PMC 2628830. PMID 19155361.
- Luk PP, Vilain R, Crainic O, McCarthy SW, Thompson JF, Scolyer RA (August 2015). "Punch biopsy of melanoma causing tumour cell implantation: another peril of utilising partial biopsies for melanocytic tumours". Australas J Dermatol. 56 (3): 227–31. doi:10.1111/ajd.12333. PMID 25827527.
- Lin SW, Kaye V, Goldfarb N, Rawal A, Warshaw E (July 2012). "Melanoma tumor seeding after punch biopsy". Dermatol Surg. 38 (7 pt 1): 1083–85. doi:10.1111/j.1524-4725.2012.02384.x. PMID 22471244.
- Martin RC 2nd, Scoggins CR, Ross MI, Reintgen DS, Noyes RD, Edwards MJ, McMasters KM (December 2005). "Is incisional biopsy of melanoma harmful?". Am J Surg. 190 (6): 913–17. doi:10.1016/j.amjsurg.2005.08.020. PMID 16307945.
- Yamashita Y, Hashimoto I, Abe Y, Seike T, Okawa K, Senzaki Y, Murao K, Kubo Y, Nakanishi H (March 2014). "Effect of biopsy technique on the survival rate of malignant melanoma patients". Arch Plast Surg. 41 (2): 122–25. doi:10.5999/aps.2014.41.2.122. PMC 3961608. PMID 24665419.
- James, William D.; Berger, Timothy G.; et al. (2006). Andrews' Diseases of the Skin: clinical Dermatology. Saunders Elsevier. pp. 694–99. ISBN 978-0-7216-2921-6.
- Rapini, Ronald P.; Bolognia, Jean L.; Jorizzo, Joseph L. (2007). Dermatology. Mosby. ISBN 978-1-4160-2999-1.
- "Malignant Melanoma: staging". Collaborative Hypertext of Radiology. Medical College of Wisconsin. 1 September 2006. Archived from the original on 2010-07-18.
- Balch CM, Buzaid AC, Soong SJ, Atkins MB, Cascinelli N, Coit DG, Fleming ID, Gershenwald JE, Houghton A, Kirkwood JM, McMasters KM, Mihm MF, Morton DL, Reintgen DS, Ross MI, Sober A, Thompson JA, Thompson JF (August 2001). "Final version of the American Joint Committee on Cancer staging system for cutaneous melanoma". Journal of Clinical Oncology. 19 (16): 3635–48. CiteSeerX 10.1.1.475.6560. doi:10.1200/JCO.2001.19.16.3635. PMID 11504745. Archived from the original on 2006-03-05.
- Autier P (2005). "Cutaneous malignant melanoma: facts about sunbeds and sunscreen". Expert Rev Anticancer Ther. 5 (5): 821–33. doi:10.1586/14737140.5.5.821. PMID 16221052.
- Clough-Gorr KM, Titus-Ernstoff L, Perry AE, Spencer SK, Ernstoff MS (September 2008). "Exposure to sunlamps, tanning beds, and melanoma risk". Cancer Causes Control. 19 (7): 659–69. doi:10.1007/s10552-008-9129-6. PMC 6367654. PMID 18273687.
- Shihab N, Lim HW (November 2018). "Potential cutaneous carcinogenic risk of exposure to UV nail lamp: A review". Photodermatology, Photoimmunology & Photomedicine. 34 (6): 362–365. doi:10.1111/phpp.12398. PMID 29882991.
- O'Sullivan NA, Tait CP (May 2014). "Tanning bed and nail lamp use and the risk of cutaneous malignancy: a review of the literature". The Australasian Journal of Dermatology. 55 (2): 99–106. doi:10.1111/ajd.12145. PMID 24592921.
- Greinert R, de Vries E, Erdmann F, Espina C, Auvinen A, Kesminiene A, Schüz J (December 2015). "European Code against Cancer 4th Edition: Ultraviolet radiation and cancer". Cancer Epidemiology. 39 Suppl 1 (Suppl 1): S75–83. doi:10.1016/j.canep.2014.12.014. PMID 26096748.
- Kanavy HE, Gerstenblith MR (December 2011). "Ultraviolet radiation and melanoma". Semin Cutan Med Surg. 30 (4): 222–28. doi:10.1016/j.sder.2011.08.003. PMID 22123420.
- "Can Melanoma Be Prevented?". Archived from the original on June 27, 2006.
- Burnett M.E.; Wang S.Q. (April 2011). "Current sunscreen controversies: a critical review". Photodermatology, Photoimmunology & Photomedicine. 27 (2): 58–67. doi:10.1111/j.1600-0781.2011.00557.x. PMID 21392107.
- Planta MB (2011-11-01). "Sunscreen and melanoma: is our prevention message correct?". Journal of the American Board of Family Medicine. 24 (6): 735–9. doi:10.3122/jabfm.2011.06.100178. PMID 22086817.
- Dellavalle RP, Drake A, Graber M, Heilig LF, Hester EJ, Johnson KR, McNealy K, Schilling L (October 2005). "Statins and fibrates for preventing melanoma". The Cochrane Database of Systematic Reviews (4): CD003697. doi:10.1002/14651858.CD003697.pub2. PMID 16235336.
- Freeman SR, Drake AL, Heilig LF, Graber M, McNealy K, Schilling LM, Dellavalle RP (November 2006). "Statins, fibrates, and melanoma risk: a systematic review and meta-analysis". Journal of the National Cancer Institute. 98 (21): 1538–46. doi:10.1093/jnci/djj412. PMID 17077356.
- "The Sentinel Node Biopsy Procedure in Melanoma does not offer a survival advantage". Malignant Melanoma. 2008-01-08. Archived from the original on 2012-07-11. Retrieved 2012-08-13.
- Kyrgidis A, Tzellos T, Mocellin S, Apalla Z, Lallas A, Pilati P, Stratigos A (May 2015). "Sentinel lymph node biopsy followed by lymph node dissection for localised primary cutaneous melanoma". The Cochrane Database of Systematic Reviews (5): CD010307. doi:10.1002/14651858.CD010307.pub2. PMC 6461196. PMID 25978975.
- Clark GS, Pappas-Politis EC, Cherpelis BS, Messina JL, Möller MG, Cruse CW, Glass LF (July 2008). "Surgical management of melanoma in situ on chronically sun-damaged skin". Cancer Control. 15 (3): 216–24. doi:10.1177/107327480801500304. PMID 18596673.
- Balch CM, Urist MM, Karakousis CP, Smith TJ, Temple WJ, Drzewiecki K, Jewell WR, Bartolucci AA, Mihm MC, Barnhill R (September 1993). "Efficacy of 2-cm surgical margins for intermediate-thickness melanomas (1 to 4 mm). Results of a multi-institutional randomized surgical trial". Annals of Surgery. 218 (3): 262–7, discussion 267–9. doi:10.1097/00000658-199309000-00005. PMC 1242959. PMID 8373269.
- Sladden MJ, Balch C, Barzilai DA, Berg D, Freiman A, Handiside T, Hollis S, Lens MB, Thompson JF (October 2009). "Surgical excision margins for primary cutaneous melanoma". The Cochrane Database of Systematic Reviews. 129 (4): 56. doi:10.1002/14651858.CD004835.pub2. PMID 19821334.
- Mohs FE, Mikhail GR (January 1991). Mohs micrographic surgery. W.B. Saunders. pp. 13–14. ISBN 978-0-7216-3415-9. Archived from the original on 2016-01-07.
- Bene NI, Healy C, Coldiron BM (May 2008). "Mohs micrographic surgery is accurate 95.1% of the time for melanoma in situ: a prospective study of 167 cases". Dermatologic Surgery. 34 (5): 660–4. doi:10.1111/j.1524-4725.2007.34124.x. PMID 18261099.
Cure rate as high as 98% for small melanoma in situ, and as high as 95% noted for lentigo maligna variant of melanona in situ has been reported with Mohs surgery.
- "The Screening and Surveillance of Ultrasound in Melanoma trial (SUNMEL)". Archived from the original on 2009-01-06.
- Crowson AN, Haskell H (October 2013). "The role of sentinel lymph-node biopsy in the management of cutaneous melanoma". Giornale Italiano di Dermatologia e Venereologia. 148 (5): 493–9. PMID 24005142.
- Ross MI, Gershenwald JE (May–Jun 2013). "Sentinel lymph node biopsy for melanoma: a critical update for dermatologists after two decades of experience". Clinics in Dermatology. 31 (3): 298–310. doi:10.1016/j.clindermatol.2012.08.004. PMID 23608449.
- American Academy of Dermatology (February 2013), "Five Things Physicians and Patients Should Question", Choosing Wisely: an initiative of the ABIM Foundation, American Academy of Dermatology, archived from the original on 1 December 2013, retrieved 5 December 2013, which cites:
- Bichakjian CK, Halpern AC, Johnson TM, Foote Hood A, Grichnik JM, Swetter SM, Tsao H, Barbosa VH, Chuang TY, Duvic M, Ho VC, Sober AJ, Beutner KR, Bhushan R, Smith Begolka W (November 2011). "Guidelines of care for the management of primary cutaneous melanoma. American Academy of Dermatology". Journal of the American Academy of Dermatology. 65 (5): 1032–47. doi:10.1016/j.jaad.2011.04.031. PMID 21868127.
- American Joint Committee on Cancer (2010). Edge SB (ed.). AJCC cancer staging manual (7th ed.). Springer. ISBN 978-0-387-88440-0.
- National Comprehensive Cancer Network (2012), National Comprehensive Cancer Network clinical practice guidelines in oncology (NCCN Guidelines): melanoma (PDF), Fort Washington, Pennsylvania: National Comprehensive Cancer Network, archived from the original (PDF) on 28 December 2013, retrieved 5 December 2013

- van Kempen LC, Redpath M, Robert C, Spatz A (November 2014). "Molecular pathology of cutaneous melanoma". Melanoma Management. 1 (2): 151–164. doi:10.2217/mmt.14.23. PMC 6094595. PMID 30190820.
- Brunner G, Reitz M, Heinecke A, Lippold A, Berking C, Suter L, Atzpodien J (February 2013). "A nine-gene signature predicting clinical outcome in cutaneous melanoma". Journal of Cancer Research and Clinical Oncology. 139 (2): 249–58. doi:10.1007/s00432-012-1322-z. PMID 23052696.
- Swanson N, Lee K, Gorman A, Lee H (2002). "Biopsy techniques. Diagnosis of melanoma". Intensive 2011: The Third International Conference on Resource Intensive Applications and Services. 20 (4): 677–80. doi:10.1016/S0733-8635(02)00025-6. PMID 12380054.
- Kirkwood JM, Strawderman MH, Ernstoff MS, Smith TJ, Borden EC, Blum RH (January 1996). "Interferon alfa-2b adjuvant therapy of high-risk resected cutaneous melanoma: the Eastern Cooperative Oncology Group Trial EST 1684". Journal of Clinical Oncology. 14 (1): 7–17. doi:10.1200/JCO.1996.14.1.7. PMID 8558223.
- English (2010). Neil H. Cox; John S.C. (eds.). British Association of Dermatologists' management guidelines. Wiley-Blackwell. ISBN 978-1-4443-3552-1. Retrieved 19 August 2013.
- Mocellin S, Lens MB, Pasquali S, Pilati P, Chiarion Sileni V (June 2013). "Interferon alpha for the adjuvant treatment of cutaneous melanoma". The Cochrane Database of Systematic Reviews (6): CD008955. doi:10.1002/14651858.CD008955.pub2. PMID 23775773.
- Wheatley K, Ives N, Eggermont A, Kirkwood J, Cascinelli N, Markovic SN, Hancock B, Lee S, Suciu S (2007). "Interferon-α as an adjuvant therapy for melanoma: an individual patient meta-analysis of randomised trials". J Clin Oncol. 25 (18 Suppl): 8526. doi:10.1200/jco.2007.25.18_suppl.8526 (inactive 2019-08-02).
- Kirkwood JM, Ibrahim JG, Sondak VK, Richards J, Flaherty LE, Ernstoff MS, Smith TJ, Rao U, Steele M, Blum RH (June 2000). "High- and low-dose interferon alfa-2b in high-risk melanoma: first analysis of intergroup trial E1690/S9111/C9190". Journal of Clinical Oncology. 18 (12): 2444–58. doi:10.1200/JCO.2000.18.12.2444. PMID 10856105.
- Kirkwood JM, Ibrahim JG, Sondak VK, Ernstoff MS, Ross M (March 2002). "Interferon alfa-2a for melanoma metastases". Lancet. 359 (9310): 978–9. doi:10.1016/S0140-6736(02)08001-7. PMID 11918944.
- Weight RM, Viator JA, Dale PS, Caldwell CW, Lisle AE (2006). "Photoacoustic detection of metastatic melanoma cells in the human circulatory system". Opt. Lett. 31 (20): 2998–3000. Bibcode:2006OptL...31.2998W. doi:10.1364/OL.31.002998. PMID 17001379.
- Pasquali S, Hadjinicolaou AV, Chiarion Sileni V, Rossi CR, Mocellin S (February 2018). "Systemic treatments for metastatic cutaneous melanoma". The Cochrane Database of Systematic Reviews. 2: CD011123. doi:10.1002/14651858.CD011123.pub2. PMC 6491081. PMID 29405038.
- O'Donoghue C, Perez MC, Mullinax JE, Hardman D, Sileno S, Naqvi SM, Kim Y, Gonzalez RJ, Zager JS (December 2017). "Isolated Limb Infusion: A Single-Center Experience with Over 200 Infusions". Annals of Surgical Oncology. 24 (13): 3842–3849. doi:10.1245/s10434-017-6107-9. PMID 29019175.
- Giles MH, Coventry BJ (August 2013). "Isolated limb infusion chemotherapy for melanoma: an overview of early experience at the Adelaide Melanoma Unit". Cancer Management and Research. 5: 243–9. doi:10.2147/cmar.s45746. PMC 3753062. PMID 23990731.
- Berger M, Richtig G, Kashofer K, Aigelsreiter A, Richtig E (June 2018). "The window of opportunities for targeted therapy in BRAFwt/NRASwt/KITwt melanoma: biology and clinical implications of fusion proteins and other mutations". Giornale Italiano di Dermatologia e Venereologia. 153 (3): 349–360. doi:10.23736/S0392-0488.18.05970-9. PMID 29600692.
- Broussard L, Howland A, Ryu S, Song K, Norris D, Armstrong CA, Song PI (September 2018). "Melanoma Cell Death Mechanisms". Chonnam Medical Journal. 54 (3): 135–142. doi:10.4068/cmj.2018.54.3.135. PMC 6165917. PMID 30288368.
- Maverakis E, Cornelius LA, Bowen GM, Phan T, Patel FB, Fitzmaurice S, He Y, Burrall B, Duong C, Kloxin AM, Sultani H, Wilken R, Martinez SR, Patel F (May 2015). "Metastatic melanoma - a review of current and future treatment options". Acta Dermato-Venereologica. 95 (5): 516–24. doi:10.2340/00015555-2035. PMID 25520039.
- Kuske M, Westphal D, Wehner R, Schmitz M, Beissert S, Praetorius C, Meier F (October 2018). "Immunomodulatory effects of BRAF and MEK inhibitors: Implications for Melanoma therapy". Pharmacological Research. 136: 151–159. doi:10.1016/j.phrs.2018.08.019. PMID 30145328.
- Sanlorenzo M, Vujic I, Posch C, Dajee A, Yen A, Kim S, Ashworth M, Rosenblum MD, Algazi A, Osella-Abate S, Quaglino P, Daud A, Ortiz-Urda S (June 2014). "Melanoma immunotherapy". Cancer Biology & Therapy. 15 (6): 665–74. doi:10.4161/cbt.28555. PMC 4049781. PMID 24651672.
- Dranitsaris G, Zhu X, Adunlin G, Vincent MD (August 2018). "Cost effectiveness vs. affordability in the age of immuno-oncology cancer drugs". Expert Review of Pharmacoeconomics & Outcomes Research. 18 (4): 351–357. doi:10.1080/14737167.2018.1467270. PMID 29681201.
- West HJ (April 2015). "JAMA Oncology Patient Page. Immune Checkpoint Inhibitors". JAMA Oncology. 1 (1): 115. doi:10.1001/jamaoncol.2015.0137. PMID 26182315.
- Buzaid AC (October 2004). "Management of metastatic cutaneous melanoma". Oncology. 18 (11): 1443–50, discussion 1457–9. PMID 15609471.
- Rosenberg SA, Restifo NP (April 2015). "Adoptive cell transfer as personalized immunotherapy for human cancer". Science. 348 (6230): 62–8. Bibcode:2015Sci...348...62R. doi:10.1126/science.aaa4967. PMC 6295668. PMID 25838374.
- Zang YW, Gu XD, Xiang JB, Chen ZY (June 2014). "Clinical application of adoptive T cell therapy in solid tumors". Medical Science Monitor. 20: 953–9. doi:10.12659/msm.890496. PMC 4063985. PMID 24912947.
- Tzellos T, Kyrgidis A, Mocellin S, Chan AW, Pilati P, Apalla Z (December 2014). "Interventions for melanoma in situ, including lentigo maligna". The Cochrane Database of Systematic Reviews (12): CD010308. doi:10.1002/14651858.CD010308.pub2. PMID 25526608.
- Johnson TM, Headington JT, Baker SR, Lowe L (November 1997). "Usefulness of the staged excision for lentigo maligna and lentigo maligna melanoma: the "square" procedure". J. Am. Acad. Dermatol. 37 (5 Pt 1): 758–64. doi:10.1016/S0190-9622(97)70114-2. PMID 9366823.
- Hill R, Healy B, Holloway L, Kuncic Z, Thwaites D, Baldock C (March 2014). "Advances in kilovoltage x-ray beam dosimetry". Physics in Medicine and Biology. 59 (6): R183–231. Bibcode:2014PMB....59R.183H. doi:10.1088/0031-9155/59/6/r183. PMID 24584183.
- Bastiaannet E, Beukema JC, Hoekstra HJ (February 2005). "Radiation therapy following lymph node dissection in melanoma patients: treatment, outcome and complications". Cancer Treatment Reviews. 31 (1): 18–26. doi:10.1016/j.ctrv.2004.09.005. PMID 15707701.
- Boyer (1999). Primary Care Oncology. Ford.
- Homsi J, Kashani-Sabet M, Messina J, Daud A (2005). "Cutaneous melanoma: prognostic factors" (PDF). Cancer Control. 12 (4): 223–29. doi:10.1177/107327480501200403. PMID 16258493. Archived from the original (PDF) on 2008-02-16.
- Bae JM, Choi YY, Kim DS, Lee JH, Jang HS, Lee JH, Kim H, Oh BH, Roh MR, Nam KA, Chung KY (January 2015). "Metastatic melanomas of unknown primary show better prognosis than those of known primary: a systematic review and meta-analysis of observational studies". Journal of the American Academy of Dermatology. 72 (1): 59–70. doi:10.1016/j.jaad.2014.09.029. PMID 25440435.
- "CANCERMondial (GLOBOCAN)". GLOBOCAN. 2010. Archived from the original on 17 February 2012. Retrieved 12 August 2010.
- Berwick M, Wiggins C (2006). "The current epidemiology of cutaneous malignant melanoma". Front Biosci. 11: 1244–54. doi:10.2741/1877. PMID 16368510.
- "Cancer in Australia: an overview 2012". AIHW. Archived from the original on 2014-06-02.
- Guy GP, Thomas CC, Thompson T, Watson M, Massetti GM, Richardson LC (2015). "Vital signs: melanoma incidence and mortality trends and projections – United States, 1982–2030". MMWR Morb. Mortal. Wkly. Rep. 64 (21): 591–6. PMC 4584771. PMID 26042651. Archived from the original on 2017-05-31.
- "CDC – Skin Cancer Statistics". www.cdc.gov. Archived from the original on 2017-04-10. Retrieved 2017-04-10.
- "Key Statistics for Melanoma Skin Cancer". www.cancer.org. Archived from the original on 2017-04-10. Retrieved 2017-04-10.
- Urteaga O, Pack G (1966). "On the antiquity of melanoma". Cancer. 19 (5): 607–10. doi:10.1002/1097-0142(196605)19:5<607::AID-CNCR2820190502>3.0.CO;2-8. PMID 5326247.
- Bodenham D (1968). "A study of 650 observed malignant melanomas in the South-West region". Annals of the Royal College of Surgeons of England. 43 (4): 218–39. PMC 2312310. PMID 5698493.
- Laennec RTH (1806). "Sur les melanoses". Bulletin de la Faculte de Medecine de Paris. 1: 24–26.
- Norris W (October 1820). "Case of Fungoid Disease". Edinburgh Medical and Surgical Journal. 16 (65): 562–565. PMC 5830209. PMID 30332089.
- Norris W. Eight cases of Melanosis with pathological and therapeutical remarks on that disease. London: Longman; 1857.
- Cooper S (1844). The First Lines of the Theory and Practice of Surgery: Including the Principle Operations. S.S. and W. Wood.
- Merriam-Webster, Merriam-Webster's Collegiate Dictionary, Merriam-Webster.
- μέλας Archived 2011-06-05 at the Wayback Machine, Henry George Liddell, Robert Scott, A Greek-English Lexicon, on Perseus
- Elsevier, Dorland's Illustrated Medical Dictionary, Elsevier.
- Houghton Mifflin Harcourt, The American Heritage Dictionary of the English Language, Houghton Mifflin Harcourt.
- "Drugs in Clinical Development for Melanoma". Pharmaceutical Medicine. 26 (3): 171–83. 23 December 2012. doi:10.1007/BF03262391.
- Sotomayor M, Yu H, Antonia S, Sotomayor E, Pardoll D (2002). "Advances in gene therapy for malignant melanoma". Cancer Control. 9 (1): 39–48. doi:10.1177/107327480200900106. PMID 11907465.
- Dudley ME, Yang JC, Sherry R, et al. (November 2008). "Adoptive cell therapy for patients with metastatic melanoma: evaluation of intensive myeloablative chemoradiation preparative regimens". J. Clin. Oncol. 26 (32): 5233–39. doi:10.1200/JCO.2008.16.5449. PMC 2652090. PMID 18809613.
- Besser MJ, Shapira-Frommer R, Treves AJ, et al. (May 2010). "Clinical responses in a phase II study using adoptive transfer of short-term cultured tumor infiltration lymphocytes in metastatic melanoma patients". Clin. Cancer Res. 16 (9): 2646–55. doi:10.1158/1078-0432.CCR-10-0041. PMID 20406835.
- "New Method of Gene Therapy Alters Immune Cells for Treatment of Advanced Melanoma; Technique May Also Apply to Other Common Cancers". 30 December 2015. Archived from the original on 28 September 2006.
- "Immune System Taught To Fight Melanoma". CBSNews. 30 May 2009. Archived from the original on 29 October 2010.
- Schwartzentruber DJ, Lawson DH, Richards JM, Conry RM, Miller DM, Treisman J, Gailani F, Riley L, Conlon K, Pockaj B, Kendra KL, White RL, Gonzalez R, Kuzel TM, Curti B, Leming PD, Whitman ED, Balkissoon J, Reintgen DS, Kaufman H, Marincola FM, Merino MJ, Rosenberg SA, Choyke P, Vena D, Hwu P (June 2011). "gp100 peptide vaccine and interleukin-2 in patients with advanced melanoma". The New England Journal of Medicine. 364 (22): 2119–27. doi:10.1056/NEJMoa1012863. PMC 3517182. PMID 21631324.
- Harmon A (February 21, 2010). "A Roller Coaster Chase for a Cure". The New York Times. Archived from the original on February 10, 2017.
- Andrew Pollack (June 5, 2011). "Drugs Show Promise Slowing Advanced Melanoma". New York Times. Archived from the original on January 31, 2017.
- Chapman PB, Hauschild A, Robert C, Haanen JB, Ascierto P, Larkin J, Dummer R, Garbe C, Testori A, Maio M, Hogg D, Lorigan P, Lebbe C, Jouary T, Schadendorf D, Ribas A, O'Day SJ, Sosman JA, Kirkwood JM, Eggermont AM, Dreno B, Nolop K, Li J, Nelson B, Hou J, Lee RJ, Flaherty KT, McArthur GA, BRIM-3 Study Group (30 June 2011). "Improved Survival with Vemurafenib in Melanoma with BRAF V600E Mutation". New England Journal of Medicine. 364 (26): 2507–16. doi:10.1056/NEJMoa1103782. PMC 3549296. PMID 21639808.
- "GSK melanoma drugs add to tally of U.S. drug approvals". Reuters. May 30, 2013. Archived from the original on September 24, 2015.
- "Combination of dabrafenib and trametinib delays development of treatment resistance in MM patients". News Medical. October 1, 2012. Archived from the original on May 14, 2013.
- Flaherty KT, Infante JR, Daud A, Gonzalez R, Kefford RF, Sosman J, Hamid O, Schuchter L, Cebon J, Ibrahim N, Kudchadkar R, Burris HA 3rd, Falchook G, Algazi A, Lewis K, Long GV, Puzanov I, Lebowitz P, Singh A, Little S, Sun P, Allred A, Ouellet D, Kim KB, Patel K, Weber J (1 November 2012). "Combined BRAF and MEK Inhibition in Melanoma with BRAF V600 Mutations". New England Journal of Medicine. 367 (18): 1694–1703. doi:10.1056/NEJMoa1210093. PMC 3549295. PMID 23020132.
- "Dabrafenib/Trametinib Combination Approved for Advanced Melanoma". OncLive. January 9, 2014. Archived from the original on January 25, 2014.
- "Counteracting Drug Resistance in Melanoma". 2015. Archived from the original on 2015-02-04.
- "Bristol drug cuts death risk in advanced melanoma". Reuters. June 5, 2010. Archived from the original on November 9, 2010.
- "The Risk For Bristol". Forbes. Archived from the original on 2011-03-15.
- "Phase 3 clinical study: Ipilimumab boosts, sustains immune system responses against melanoma tumors". News-medical.net. 2010-06-09. Archived from the original on 2012-10-19. Retrieved 2012-08-13.
- Jefferson E (2011-03-25). "FDA approves new treatment for a type of late-stage skin cancer" (Press release). U.S. Food and Drug Administration (FDA). Archived from the original on 2011-03-27. Retrieved 2011-03-25.
- Pollack, Andrew (2011-03-25). "Approval for Drug That Treats Melanoma". The New York Times. Archived from the original on 2011-04-01. Retrieved 2011-03-27.
- Drugs.com: Yervoy Archived 2011-08-09 at the Wayback Machine
- Robert C, Thomas L, Bondarenko I, et al. (June 2011). "Ipilimumab plus dacarbazine for previously untreated metastatic melanoma". N. Engl. J. Med. 364 (26): 2517–26. doi:10.1056/NEJMoa1104621. PMID 21639810.
- Voit C, Van Akkooi AC, Schäfer-Hesterberg G, et al. (February 2010). "Ultrasound morphology criteria predict metastatic disease of the sentinel nodes in patients with melanoma". J. Clin. Oncol. 28 (5): 847–52. doi:10.1200/JCO.2009.25.7428. PMID 20065175.
- "malignant-melanoma.org". Archived from the original on 2011-10-14.
- Forbes NE, Abdelbary H, Lupien M, Bell JC, Diallo JS (September 2013). "Exploiting tumor epigenetics to improve oncolytic virotherapy". Frontiers in Genetics. 4: 184. doi:10.3389/fgene.2013.00184. PMC 3778850. PMID 24062768.
- Andtbacka RH, Kaufman HL, Collichio F, Amatruda T, Senzer N, Chesney J, Delman KA, Spitler LE, Puzanov I, Agarwala SS, Milhem M, Cranmer L, Curti B, Lewis K, Ross M, Guthrie T, Linette GP, Daniels GA, Harrington K, Middleton MR, Miller WH, Zager JS, Ye Y, Yao B, Li A, Doleman S, VanderWalde A, Gansert J, Coffin RS (September 2015). "Talimogene Laherparepvec Improves Durable Response Rate in Patients With Advanced Melanoma". Journal of Clinical Oncology. 33 (25): 2780–8. doi:10.1200/JCO.2014.58.3377. PMID 26014293.
External links
| Classification | |
|---|---|
| External resources |
| Look up melanoma in Wiktionary, the free dictionary. |
| Wikimedia Commons has media related to Melanoma. |
- Melanoma at Curlie
| Authority control |
|
|---|