

Algorithm to assist in the interpretation of influenza testing results and clinical decision-making during periods when influenza viruses are circulating in the community
 ShareCompartir
ShareCompartir
Back to Clinical Description & Lab Diagnosis of Influenza
Figure: Algorithm to assist in the interpretation of influenza testing results and clinical decision-making during periods when influenza viruses are circulating in the community1
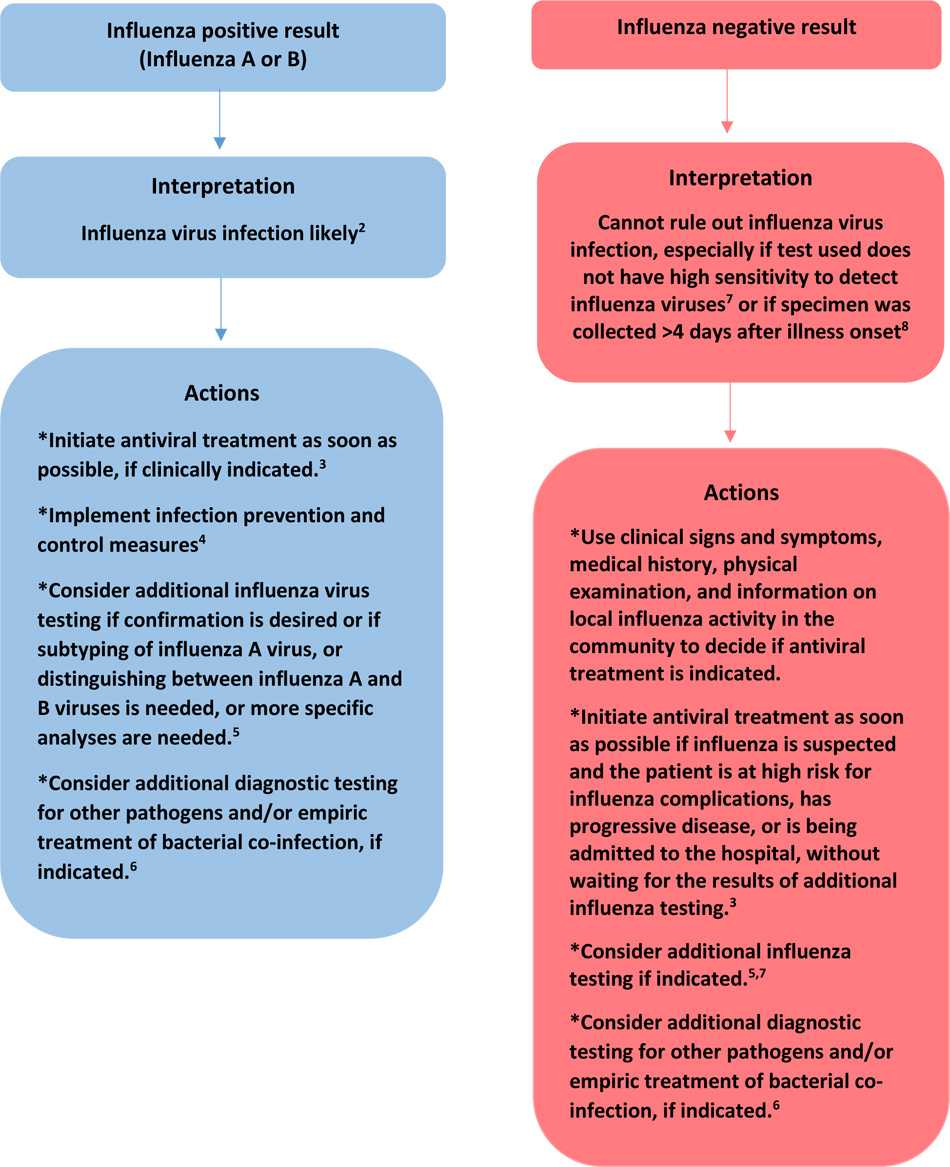
1. During periods when influenza activity is high and influenza viruses are circulating among persons in the community, the positive predictive value of a test result is high (that is, the chance that a positive result indicates that the patient has influenza is high – likely true positive result), and the negative predictive value of a test result is low (the chance that a negative result indicates that the patients does not have influenza – consider potential for a false negative result) if the influenza test used has suboptimal sensitivity (such as a rapid influenza diagnostic test or immunofluorescence assay) to detect influenza virus in respiratory specimens compared to a “gold standard test” such as RT-PCR or viral culture.
2. A positive result of an antigen detection test (rapid influenza diagnostic test, immunofluorescence assay) or a molecular assay likely means that the patient has or has recently had influenza virus infection, but does not always mean that the patient is still infectious. Only isolation of influenza virus by viral culture can identify whether infectious influenza virus is present.
3. Antiviral treatment is recommended as soon as possible for all of the following: outpatients who are at high-risk for influenza complications, persons with progressive disease, and all hospitalized patients with suspected or confirmed influenza. See Influenza Antiviral Medications: Summary for Clinicians for more information.
4. See: Prevention Strategies for Seasonal Influenza in Healthcare Settings
5. Influenza virus infection may include seasonal influenza A(H3N2), A(H1N1)pdm09, influenza B, or rarely, novel influenza A virus infection. The interpretation of positive and negative influenza testing results will, in part, depend on the test used, the sensitivity and specificity of the test compared to a “gold standard test”, and the prevalence of influenza in the population being tested – some tests only detect influenza A virus, some will detect influenza B virus and some will detect both A and B viruses. If tests for both influenza A and influenza B are positive, refer the respiratory specimen to a public health laboratory for resolution, as dual infections are uncommon. Most tests do not distinguish between influenza A virus subtypes, and do not distinguish between seasonal influenza A viruses and novel influenza A viruses. If influenza A virus subtyping is needed, specimens should be sent to a state public health laboratory for molecular testing (RT-PCR). If there has been recent exposure to pigs or birds (poultry or wild birds) or to a sick person with such animal exposures and novel influenza A virus infection is suspected, the state health department should be notified immediately and specimens should be forwarded for RT-PCR at the state health department virology laboratory. See Avian Influenza: Information for Health Professionals and Laboratorians and Variant Influenza Viruses: Background and CDC Risk Assessment and Reporting for more information.
6. Consult the local or state health department or other sources (e.g., virology testing at a local hospital) for local activity on other respiratory pathogens associated with acute respiratory illness. Empiric antibiotic coverage in hospitalized patients should consider coverage for Streptococcus pneumoniae, Staphylococcus aureus (including MRSA), Group A Streptococcus, and others, especially for hospitalized adult patients per IDSA/ATS CAP guidelines.
7. Antigen detection tests (rapid influenza diagnostic tests, immunofluorescence assays) have suboptimal sensitivities to detect influenza viruses in respiratory specimens compared to molecular assays and viral culture and negative results of antigen detection tests should not be used to exclude a diagnosis of influenza. If influenza is suspected, and diagnostic testing is indicated, influenza testing of respiratory specimens by molecular assay (RT-PCR) should be performed.
8. Respiratory specimens should be collected as close to illness onset as possible to maximize detection of influenza viruses. Influenza viral shedding in the upper respiratory tract declines after about 3-4 days in most people. Infants, young children, immunocompromised and immunosuppressed patients can shed influenza viruses for longer duration. Molecular assays can detect influenza viral RNA in respiratory specimens for longer periods than antigen detection assays. For hospitalized patients with lower respiratory tract disease and suspected influenza, lower respiratory tract specimens should be collected and tested for influenza viruses by RT-PCR because influenza viral shedding in the lower respiratory tract may be detectable for longer periods than in the upper respiratory tract, if influenza testing of upper respiratory tract specimens yields a negative result. If the patient is critically ill on invasive mechanical ventilation, and has tested negative on an upper respiratory tract specimen, including by a molecular assay, a lower respiratory tract specimen (endotracheal aspirate or bronchioalveolar lavage fluid) should be collected for influenza testing by RT-PCR or other molecular assays.
- Page last reviewed: November 2, 2016
- Page last updated: November 2, 2016
- Content source:
- Centers for Disease Control and Prevention, National Center for Immunization and Respiratory Diseases (NCIRD)
- Page maintained by: Office of the Associate Director for Communication, Digital Media Branch, Division of Public Affairs