

Influenza virus testing in investigational outbreaks in institutional or other closed settings
 ShareCompartir
ShareCompartir
Back to Clinical Description & Lab Diagnosis of Influenza
Figure: Guide to use of influenza virus diagnostic tests in investigating outbreaks in institutional or other closed settings1
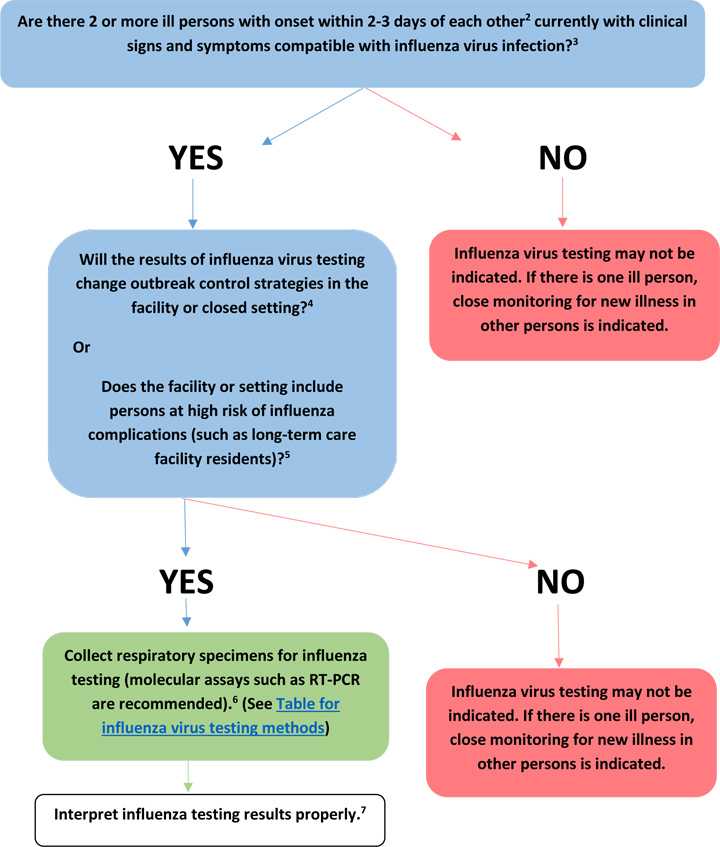
1. Examples of institutional or semi-closed settings include long-term care facilities, nursing homes, schools, correctional facilities, hospitals, dormitories, and cruise ships.
2. In settings with persons at high-risk of influenza complications, a single case of suspected influenza is sufficient for triggering influenza testing and consideration of prompt implementation of infection prevention and control measures, including active surveillance for new illness cases.
3. The signs and symptoms of influenza can vary by age, immune status, and presence of underlying medical conditions. Uncomplicated influenza may include Influenza like-illness (fever with either cough or sore throat), fever with other respiratory symptoms, but fever is not always present. Other symptoms associated with influenza include myalgias, headache, and fatigue. Note that some persons may have atypical presentations (e.g., elderly, very young infants, immunosuppressed, and patients with certain chronic medical conditions). Complications include exacerbation of underlying chronic disease, (e.g., congestive cardiac failure, asthma), pneumonia, bacterial co-infection, bronchiolitis, croup, encephalopathy, encephalitis, seizures, myocarditis, myositis, and others.
4. For example, will influenza testing results influence whether antivirals are used for confirmed influenza cases only or empirically for treatment of ill persons, or for chemoprophylaxis of influenza, changes in infection prevention and control practices (isolation or cohorting of ill, quarantine of exposed), changes in admission or staffing policies, or changes in social distancing recommendations, etc? See Influenza Antiviral Medications: Summary for Clinicians and Infection Control in Health Care Facilities for more information.
5. Persons aged ≥65 years or <2 years; pregnant women; persons with chronic lung disease (including asthma), heart disease, renal, metabolic, hematologic and neurologic disease; immunosuppression; and morbid obesity. See People at High Risk of Developing Flu-Related Complications for more information.
6. In an outbreak setting, RT-PCR or other molecular assays are preferred. Because of the low sensitivity of antigen detection assays such as rapid influenza diagnostic tests (RIDTs) or immunofluorescence assays, false negative results are possible and testing of specimens from more than one ill person is recommended because use of RIDTs or immunofluorescence assays may miss detection of an influenza outbreak. The presence of any influenza positives among persons with clinically compatible illnesses is supportive of influenza virus infection as the probable cause of the outbreak. Negative RIDT results do not exclude influenza virus infection due to low sensitivity to detect influenza viruses. Confirmation of RIDT results by more specific influenza testing (RT-PCR and viral culture) is indicated. See Table 1: Overview of Influenza Testing Methods for more information.
7. Proper interpretation of influenza testing results is very important. See Figure: Influenza testing algorithm to help interpret results when influenza viruses ARE circulating in the community and Figure: Influenza testing algorithm to help interpret results when influenza viruses are NOT circulating in the community for more information.
- Page last reviewed: October 28, 2016
- Page last updated: October 28, 2016
- Content source:
- Centers for Disease Control and Prevention, National Center for Immunization and Respiratory Diseases (NCIRD)
- Page maintained by: Office of the Associate Director for Communication, Digital Media Branch, Division of Public Affairs