

Human Papillomavirus
 ShareCompartir
ShareCompartir
On this Page
Human papillomavirus (HPV) is the most common sexually transmitted infection in the United States. The relationship of cervical cancer and sexual behavior was suspected for more than 100 years and was established by epidemiologic studies in the 1960s. In the early 1980s, cervical cancer cells were demonstrated to contain HPV DNA. Epidemiologic studies showing a consistent association between HPV and cervical cancer were published in the 1990s. The first vaccine to prevent infection with four types of HPV was licensed in 2006.
Human Papillomaviruses (HPV)
- Small DNA virus
- More than 120 types identified based on the genetic sequence of the outer capsid protein L1
- About 40 types infect the mucosal epithelium
Human Papillomavirus Types and Disease Association
Human Papillomaviruses
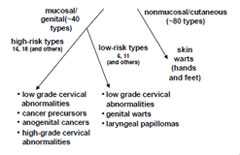
Human papillomaviruses are small, double-stranded DNA viruses that infect the epithelium. More than 120 HPV types have been identified; they are differentiated by the genetic sequence of the outer capsid protein L1. Most HPV types infect the cutaneous epithelium and can cause common skin warts. About 40 types infect the mucosal epithelium; these are categorized according to their epidemiologic association with cervical cancer. Infection with low-risk, or nononcogenic types, such as types 6 and 11, can cause benign or low-grade cervical cell abnormalities, genital warts and laryngeal papillomas. High-risk, or oncogenic, HPV types act as carcinogens in the development of cervical cancer and other anogenital cancers. High-risk types (currently including types 16 and 18, among others) can cause low-grade cervical cell abnormalities, high-grade cervical cell abnormalities that are precursors to cancer, and anogenital cancers. High-risk HPV types are detected in 99% of cervical cancers. Type 16 is the cause of approximately 50% of cervical cancers worldwide, and types 16 and 18 together account for about 70% of cervical cancers. Infection with a high-risk HPV type is considered necessary for the development of cervical cancer, but by itself it is not sufficient to cause cancer because the vast majority of women with HPV infection do not develop cancer.
In addition to cervical cancer, HPV infection is also associated with anogenital cancers less common than cervical cancer, such as cancer of the vulva, vagina, penis and anus. The association of genital types of HPV with non-genital cancers is less well established, but studies support a role for these HPV types in some oropharyngeal cancers.
Pathogenesis
Natural History of HPV Infection
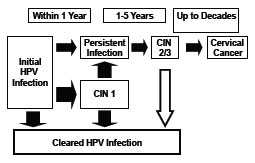
HPV infection occurs at the basal epithelium. Although the incidence of infection is high, most infections resolve spontaneously. A small proportion of infected persons become persistently infected; persistent infection is the most important risk factor for the development of cervical cancer. The most common clinically significant manifestation of persistent genital HPV infection is cervical intraepithelial neoplasia, or CIN. Within a few years of infection, low-grade CIN—called CIN 1—may develop, which may spontaneously resolve and the infection clear.
Persistent HPV infection, however, may progress directly to higher-grade CIN, called CIN2 or CIN3. High-grade abnormalities are at risk of progression to cancer and so are considered cancer precursors. Some high-grade abnormalities spontaneously regress. If left undetected and untreated, years or decades later CIN2 or 3 can progress to cervical cancer.
Infection with one type of HPV does not prevent infection with another type. Of persons infected with mucosal HPV, 5% to 30% are infected with multiple types of the virus.
Clinical Features
HPV Clinical Features
- Most HPV infections are asymptomatic and result in no clinical disease
- Clinical manifestations of HPV infection include:
- anogenital warts
- recurrent respiratory papillomatosis
- cervical cancer precursors (cervical intraepithelial neoplasia)
- cancer (cervical, anal, vaginal, vulvar, penile, and oropharyngeal cancer)
Most HPV infections are asymptomatic and result in no clinical disease. Clinical manifestations of HPV infection include anogenital warts, recurrent respiratory papillomatosis, cervical cancer precursors (cervical intraepithelial neoplasia), and cancers, including cervical, anal, vaginal, vulvar, penile, and oropharyngeal cancer.
Laboratory Diagnosis
HPV has not been cultured by conventional methods. Infection is identified by detection of HPV DNA from clinical samples. Assays for HPV detection differ considerably in their sensitivity and type specificity, and detection is also affected by the anatomic region sampled as well as the method of specimen collection.
Several HPV tests have been approved by the Food and Drug Administration (FDA) and detect 13-14 high-risk types (HPV 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, 68). Test results are reported as positive or negative for any of the types; some tests specifically identify HPV 16 and 18. These tests are approved for triage of Papanicolaou (Pap) test results (ASC-US, atypical cells of undetermined significance) and in combination with the Pap test for cervical cancer screening in women 30 years of age and older. The tests are not clinically indicated nor approved for use in men.
Epidemiologic and basic research studies of HPV generally use nucleic acid amplification methods that generate type-specific results. The polymerase chain reaction (PCR) assays used most commonly in epidemiologic studies target genetically conserved regions in the L1 gene.
The most frequently used HPV serologic assays are virus-like particle (VLP)-based enzyme immunoassays. However, laboratory reagents used for these assays are not standardized and there are no standards for setting a threshold for a positive result.
Medical Management
There is no specific treatment for HPV infection. Medical management depends on treatment of the specific clinical manifestation of the infection (such as genital warts or abnormal cervical cell cytology).
Epidemiology
HPV Epidemiology
- Reservoir
- Human
- Transmission
- Direct contact, usually sexual
- Temporal pattern
- None
- Communicability
- Presumed to be high
Occurrence
HPV infection occurs throughout the world.
Reservoir
Viruses in the papillomavirus family affect other species. Humans are the only natural reservoir of HPV.
Transmission
HPV is transmitted by direct contact, usually sexual, with an infected person. Transmission occurs most frequently with sexual intercourse but can occur following nonpenetrative sexual activity.
Studies of newly acquired HPV infection demonstrate that infection occurs soon after onset of sexual activity. In a prospective study of college women, the cumulative incidence of infection was 40% by 24 months after first sexual intercourse. HPV 16 accounted for 10.4% of infections.
Genital HPV infection also may be transmitted by nonsexual routes, but this appears to be uncommon. Nonsexual routes of genital HPV transmission include transmission from a woman to a newborn infant at the time of birth.
Temporal Pattern
There is no known seasonal variation in HPV infection.
Communicability
HPV is presumably communicable during the acute infection and during persistent infection. This issue is difficult to study because of the inability to culture the virus. Communicability can be presumed to be high because of the large number of new infections estimated to occur each year.
Risk Factors
Risk factors for HPV infection are primarily related to sexual behavior, including lifetime and recent sex partners. Results of epidemiologic studies are less consistent for other risk factors, including young age at sexual initiation, number of pregnancies, genetic factors, smoking, and lack of circumcision of male partner.
Disease Burden in the United States
HPV Disease Burden in the United States
- Anogenital HPV is the most common sexually transmitted infection in the US
- estimated 79 million infected
- 14 million new infections/year
- Common among adolescents and young adults
Anogenital HPV infection is believed to be the most common sexually transmitted infection in the United States. An estimated 79 million persons are infected, and an estimated 14 million new HPV infections occur annually with half of these in persons 15-24 years.
The two most common types of cervical cancer worldwide, squamous cell carcinoma followed by adenocarcinoma, are both caused by HPV. The CDC and National Cancer Institute’s United States Cancer Statistics Working Group reports that from 2005 through 2009 there were annual averages of 12,595 cases and 3,968 deaths due to cervical cancer. HPV is believed to be responsible for nearly all of these cases of cervical cancer. HPV types 16 and 18 are associated with 70% of these cancers.
In addition to cervical cancer, HPV is believed to be responsible for 90% of anal cancers, 71% of vulvar, vaginal, or penile cancers, and 72% of oropharyngeal cancers.
Population-based estimates, primarily from clinics treating persons with sexually transmitted infections, indicate that about 1% of the sexually active adolescent and adult population in the United States have clinically apparent genital warts. More than 90% of cases of anogenital warts are associated with the low-risk HPV types 6 and 11.
About 8 billion dollars are spent annually on management of sequelae of HPV infections, primarily for the management of abnormal cervical cytology and treatment of cervical neoplasia. This exceeds the economic burden of any other sexually transmitted infection except human immunodeficiency virus.
Prevention
HPV Infection
HPV transmission can be reduced but not eliminated with the use of physical barriers such as condoms. Recent studies demonstrated a significant reduction in HPV infection among young women after initiation of sexual activity when their partners used condoms consistently and correctly. Abstaining from sexual activity (i.e., refraining from any genital contact with another individual) is the surest way to prevent genital HPV infection. For those who choose to be sexually active, a monogamous relationship with an uninfected partner is the strategy most likely to prevent future genital HPV infections.
Cervical Cancer Screening
Cervical Cancer Screening
- Revised in 2012
- Screening should begin at age 21 years
- Screen women 21 to 65 years of age with Pap test every 3 years
- Co-testing (Pap and HPV testing) every 5 years in women 30 to 65 years of age
Most cases and deaths from cervical cancer can be prevented through detection of precancerous changes within the cervix by cervical cytology using the Pap test. Currently available Pap test screening can be done by a conventional Pap or a liquid-based cytology. CDC does not issue recommendations for cervical cancer screening, but various professional groups have published recommendations. Cervical cancer screening recommendations were revised in 2012 after the U.S. Preventive Services Task Force (USPSTF) and a multidisciplinary group, including the American Cancer Society (ASC), American Society for Colposcopy and Cervical Pathology (ASCCP), and the American Society for Clinical Pathology (ASCP) reviewed new evidence. Previously, recommendations varied by organization. Since 2012, all organizations have recommended that screening should begin at age 21 years. While there are slight differences in other aspects of the recommendations, all groups recommend screening in women aged 21 to 65 years with cytology (Pap test) every 3 years. For women aged 30 to 65 years who want to lengthen the screening interval, screening can be done with a combination of cytology and HPV testing (“co-testing”) every 5 years.
The use of HPV vaccine does not eliminate the need for continued Pap test screening, since 30% of cervical cancers are caused by HPV types not included in the vaccine.
Human Papillomavirus Vaccine
Human Papillomavirus Vaccine
- HPV L1 major capsid protein of the virus is antigen used for immunization
- L1 protein produced using recombinant technology
- L1 proteins self-assemble into virus-like particles (VLP)
- VLP are noninfectious and nononcogeric
Characteristics
Three HPV vaccines are licensed in the United States. The vaccines are non-infectious subunit vaccines. The antigen for the vaccines is the L1 major capsid protein of HPV, produced by using recombinant DNA technology. L1 proteins self-assemble into noninfectious, nononcogenic units called virus-like particles (VLP).
Quadrivalent HPV (HPV4) vaccine (Gardasil, Merck) was approved by the FDA in June 2006. The vaccine is approved for females and males 9 through 26 years of age. Each 0.5-mL dose of HPV4 contains 20 micrograms HPV 6 L1 protein, 40 micrograms HPV 11 L1 protein, 40 micrograms HPV 16 L1 protein, and 20 micrograms HPV 18 L1 protein. The vaccine antigen is adsorbed on alum adjuvant. The vaccine also includes sodium chloride, L-histidine, polysorbate 80, and sodium borate. HPV4 does not contain a preservative or antibiotic. The vaccine is supplied in single-dose vials and syringes. A 9-valent vaccine (Merck) was approved by the FDA in December 2014.
HPV Vaccines
- HPV4 (Gardasil, Merck)
- approved for females and males 9 through 26 years of age
- contains types 16 and 18 (high risk) and types 6 and 11 (low risk)
- a 9-valent vaccine licensed in December 2014
- HPV2 (Cervarix, GlaxoSmithKline)
- approved for females 10 through 25 years of age
- contains types 16 and 18 (high risk)
Bivalent HPV (HPV2) vaccine (Cervarix, GlaxoSmithKline) was approved by the FDA in October 2009. The vaccine is approved for females 9 through 25 years of age. HPV2 is not approved for males. The L1 antigen is adsorbed onto aluminum hydroxide. The unique adjuvant system, AS04, is composed of 3-O-desacyl-4’-monophosphoryl lipid A (MPL) adsorbed onto aluminum hydroxide. Each 0.5-mL dose contains 20 micrograms of HPV type 16 L1 protein and 20 micrograms of HPV type 18 L1 protein. HPV2 does not contain a preservative or antibiotic. It is available in 2 types of prefilled syringes.
Immunogenicity and Vaccine Efficacy
HPV vaccines are highly immunogenic. More than 99% of recipients develop an antibody response to HPV types included in the respective vaccines 1 month after completing the three-dose series. However, there is no known serologic correlate of immunity and no known minimal titer determined to be protective. The high efficacy found in the clinical trials to date has precluded identification of a minimum protective antibody titer. Further follow-up of vaccinated cohorts may allow determination of serologic correlates of immunity in the future.
Both HPV vaccines have been found to have high efficacy for prevention of HPV vaccine type–related persistent infection, CIN 2/3 and adenocarcinoma in-situ (AIS). Clinical efficacy for HPV4 against cervical disease was determined in two double-blind, placebo-controlled trials. In women 16 through 26 years of age vaccine efficacy for HPV 16 or 18–related CIN 2/3 or AIS was 97%. HPV4 efficacy against HPV 6, 11, 16 or 18–related genital warts was 99%.
HPV2 efficacy was evaluated in two randomized, double-blind, controlled clinical trials in females aged 15 through 25 years. In the phase III trial, efficacy against HPV 16 or 18-related CIN 2/3 or AIS was 93%.
HPV4 was evaluated in men 16 through 26 years and found to have 88% efficacy against vaccine type genital warts. Among men who have sex with men (MSM), efficacy
against anal intraepithelial neoplasia grade 2 or 3 (AIN2/3) was 75%.
HPV Vaccine Efficacy
- High efficacy among females without evidence of infection with vaccine HPV types
- No evidence of efficacy against disease caused by vaccine types with which participants were infected at the time of vaccination
- Prior infection with one HPV type did not diminish efficacy of the vaccine against other vaccine HPV types
Although high efficacy among persons without evidence of infection with vaccine HPV types was demonstrated in clinical trials of both HPV vaccines, there is no evidence of efficacy against disease caused by vaccine types with which participants were infected at the time of vaccination (i.e., the vaccines had no therapeutic effect on existing infection or disease). Participants infected with one or more vaccine HPV types prior to vaccination were protected against disease caused by the other vaccine types. Prior infection with one HPV type did not diminish efficacy of the vaccine against other vaccine HPV types.
The duration of protection following HPV vaccine is not known. For both vaccines a subset of participants have been followed for more than 60 months with no evidence of waning protection. Study populations will continue to be followed for any evidence of waning immunity.
Vaccination Schedule and Use
ACIP recommends vaccination of females with HPV2 or HPV4 for prevention of cervical cancers and precancers. HPV4 is recommended also for prevention of genital warts. ACIP recommends routine vaccination at age 11 or 12 years with HPV4 or HPV2 for females and with HPV4 for males. The vaccination series can be started beginning at age 9 years.
HPV Vaccination Recommendations
- ACIP recommends routine vaccination at age 11 or 12 years with HPV4 or HPV2 for females and HPV 4 for males
- The vaccination series can be started as young as 9 years of age
- Vaccination also recommended for females 13 through 26 years of age
- Vaccination also recommended for males 13 through 21 years of age
- All immunocompromised males (including HIV infection) and MSM through 26 years of age should be vaccinated
- Males aged 22 through 26 years may be vaccinated
HPV4 and HPV2 are each administered in a 3-dose series. The second dose should be administered 1 to 2 months after the first dose and the third dose 6 months after the first dose. Vaccination also is recommended for females aged 13 through 26 years and for males aged 13 through 21 years, who have not been previously vaccinated or who have not completed the 3-dose series. For immunocompromised males (including HIV infection) and men who have sex with men, ACIP recommends routine vaccination with HPV4, as for all males, through 26 years of age for those who have not been vaccinated previously or who have not completed the 3-dose series. Males aged 22 through 26 years without these risk factors may be vaccinated as well. HPV2 is neither licensed nor recommended for males.
If females or males reach age 27 years before the vaccination series is complete, the second and/or third doses of vaccine can be administered after age 26 to complete the vaccination series.
Prevaccination assessments (e.g., Pap testing or screening for high-risk HPV DNA, type-specific HPV tests, or HPV antibody) to establish the appropriateness of HPV vaccination are not recommended.
Ideally, vaccine should be administered before potential exposure to HPV through sexual contact; however, persons who may have already been exposed to HPV should be vaccinated. Sexually active persons who have not been infected with any of the HPV vaccine types will receive full benefit from vaccination. Vaccination will provide less benefit to persons if they have already been infected with one or more of the HPV vaccine types. However, it is not possible for a clinician to assess the extent to which sexually active persons would benefit from vaccination, and the risk of HPV infection may continue as long as persons are sexually active. Pap testing or screening for HPV DNA or HPV antibody is not recommended prior to vaccination at any age.
Both HPV vaccines are administered in a three-dose series of intramuscular injections. The second and third doses should be administered 1 to 2 and 6 months after the first dose. The third dose should follow the first dose by at least 24 weeks. The third dose need not be repeated as long as it was administered at least 16 weeks after the first dose and at least 12 weeks after the second dose. An accelerated schedule for HPV vaccine is not recommended.
HPV Vaccination Schedule
- Routine schedule is 0, 1 to 2, 6 months
- An accelerated schedule using minimum intervals is not recommended
- Series does not need to be restarted if the schedule is interrupted
- Prevaccination assessments not recommended
- No therapeutic effect on HPV infection, genital warts, cervical lesions
There is no maximum interval between doses. If the HPV vaccine schedule is interrupted, the vaccine series does not need to be restarted. If the series is interrupted after the first dose, the second dose should be given as soon as possible, and the second and third doses should be separated by an interval of at least 12 weeks. If only the third dose is delayed, it should be administered as soon as possible.
Whenever feasible, the same HPV vaccine should be used for the entire vaccination series. No studies address interchangeability of HPV vaccines. However, if the vaccine provider does not know or have available the HPV vaccine product previously administered, either HPV vaccine can be used to complete the series to provide protection against HPV 16 and 18. For protection against HPV 6 or 11-related genital warts, a vaccination series with fewer than 3 doses of HPV4 might provide less protection than a complete 3-dose HPV4 series.
HPV vaccine should be administered at the same visit as other age-appropriate vaccines, such as Tdap and quadrivalent meningococcal conjugate (MCV4) vaccines. Administering all indicated vaccines at a single visit increases the likelihood that adolescents and young adults will receive each of the vaccines on schedule. Each vaccine should be administered using a separate syringe at a different anatomic site.
As mentioned, prevaccination assessments (e.g. Pap testing or screening for high-risk HPV DNA, type-specific HPV tests, or HPV antibody) to establish the appropriateness of HPV vaccination are not recommended at any age. HPV vaccination can provide protection against infection with HPV vaccine types not already acquired. Therefore, vaccination is recommended through the recommended age for females regardless of whether they have an abnormal pap test result, and for females or males regardless of known HPV infection.
Women should be advised that the vaccine will not have a therapeutic effect on existing HPV infection, genital warts or cervical lesions.
A history of genital warts or clinically evident genital warts indicates infection with HPV, most often type 6 or 11. However, these persons may be infected with HPV types other than the HPV4 vaccine types, and therefore they may receive HPV4 vaccine if they are in the recommended age group. Persons with a history of genital warts should be advised that data do not indicate HPV4 vaccine will have any therapeutic effect on existing HPV infection or genital warts.
Because HPV vaccines are subunit vaccines, they can be administered to persons who are immunosuppressed because of disease or medications. However, the immune response and vaccine efficacy might be less than that in persons who are immunocompetent. Women who are breastfeeding may receive HPV vaccine.
Contraindications and Precautions to Vaccination
HPV Vaccine Contraindication and Precautions
- Contraindication
- severe allergic reaction to a vaccine component or following a prior dose
- Precaution
- moderate or severe acute illnesses (defer until symptoms improve)
A severe allergic reaction (e.g., anaphylaxis) to a vaccine component or following a prior dose of HPV vaccine is a contraindication to receipt of HPV vaccine. Anaphylactic allergy to latex is a contraindication to bivalent HPV vaccine in a prefilled syringe since the tip cap contains natural rubber latex. A moderate or severe acute illness is a precaution to vaccination, and vaccination should be deferred until symptoms of the acute illness improve. A minor acute illness (e.g., diarrhea or mild upper respiratory tract infection, with or without fever) is not a reason to defer vaccination.
HPV vaccine is not recommended for use during pregnancy. The vaccine has not been causally associated with adverse pregnancy outcomes or with adverse effects on the developing fetus, but data on vaccination during pregnancy are limited. Pregnancy testing before vaccination is not needed. However, if a woman is found to be pregnant after initiation of the vaccination series, the remainder of the series should be delayed until after completion of the pregnancy. No intervention is indicated. Women known to be pregnant should delay initiation of the vaccine series until after delivery.
HPV Vaccination During Pregnancy
- Initiation of the vaccine series should be delayed until after completion of pregnancy
- If a woman is found to be pregnant after initiating the vaccination series, remaining doses should be delayed until after the pregnancy
- If a vaccine dose has been administered during pregnancy, there is no indication for intervention
- Women vaccinated during pregnancy should be reported to the respective manufacturer
HPV Vaccine Adverse Reactions
- Local reactions (pain, redness, swelling)
- 20%-90%
- Fever (100°F)
- 10%-13%*
- No serious adverse reactions associated with either vaccine
*similar to reports in placebo recipients
Pregnancy registries for both HPV2 and HPV4 have been terminated. However, vaccination with either vaccine during pregnancy may still be reported to VAERS or to the manufacturer: GlaxoSmithKline at 1-888-825-5249 (for HPV2), or Merck at 1-877-888-4231 (for HPV4).
Adverse Reactions Following Vaccination
The most common adverse reactions reported during clinical trials of HPV vaccines were local reactions at the site of injection. In prelicensure clinical trials, local reactions, such as pain, redness or swelling were reported by 20% to 90% of recipients. A temperature of 100°F during the 15 days after vaccination was reported in 10% to 13% of recipients of either vaccine. A similar proportion of placebo recipients reported an elevated temperature. Local reactions generally increased in frequency with increasing doses. However, reports of fever did not increase significantly with increasing doses. No serious adverse events have been associated with either HPV vaccine based on monitoring by CDC and the Food and Drug Administration.
A variety of systemic adverse reactions were reported by vaccine recipients, including nausea, dizziness, myalgia and malaise. However, these symptoms occurred with equal frequency among both vaccine and placebo recipients.
Syncope has been reported among adolescents who received HPV and other vaccines recommended for this age group (Tdap, MCV4). Recipients should always be seated during vaccine administration. Clinicians should consider observing recipient for 15 minutes after vaccination.
Vaccine Storage and Handling
HPV vaccines should be maintained at refrigerator temperature between 35°F and 46°F (2°C and 8°C). Manufacturer package inserts contain additional information. For complete information on best practices and recommendations please refer to CDC’s Vaccine Storage and Handling Toolkit [4.33 MB, 109 pages].
Acknowledgment
The editors thank Drs. Lauri Markowitz and Elizabeth Unger for their assistance in updating this chapter.
Selected References
- American College of Obstetricians and Gynecologists. Human papillomavirus vaccination. ACOG committee opinion No. 467. Obstet Gynecol 2010;116:800–803.
- CDC. Human papillomavirus vaccination. Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR 2014;63(No. 5):1-30.
- CDC. Quadrivalent human papillomavirus vaccine. Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR 2007;56(No.RR-2):1–24.
- CDC. FDA licensure of bivalent human papillomavirus vaccine (HPV2, Cervarix) for use in females and updated HPV vaccination recommendations from the Advisory Committee on Immunization Practices (ACIP). MMWR 2010;59(No. 20);626-9.
- CDC. Recommendations on the use of quadrivalent human papillomavirus vaccine in males – Advisory Committee on Immunization Practices (ACIP), 2011. MMWR 2011;60
(No. 50):1705-8. - Dunne E, Markowitz L. Genital human papillomavirus infection. Clin Infect Dis 2006;43:624–9.
- Koutsky LA, Kiviat NB. Genital human papillomavirus. In: Holmes KK, Sparling PF, Mårdh PA, et al, eds. Sexually Transmitted Diseases. 3rd ed. New York: McGraw-Hill;1999:347-59.
- Moyer VA. Screening for cervical cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med 2012;156:880-91, W312.
- Saslow D, Solomon D, Lawson HW, et al. American Cancer Society, American Society for Colposcopy and Cervical Pathology, and American Society for Clinical Pathology screening guidelines for the prevention and early detection of cervical cancer. American Journal of Clinical pathology 2012; 137:516-42.
- Satterwhite CL, Torrone E, Meites E, et al. Sexually Transmitted Infections Among US Women and Men: Prevalence and Incidence Estimates, 2008. Sex Transm Dis. 2013;40:187-93
- Schiller JT, Lowy DR, Markowitz LE. Human papillomavirus vaccines. In: Plotkin SA, Orenstein WA, Offit PA, eds. Vaccines. 6th ed. China: Saunders 2012:235-256.
- Trottier H, Franco E. The epidemiology of genital human papillomavirus infection. Vaccine 2006;24(suppl1):51–15.
- U.S. Cancer Statistics Working Group. United States Cancer Statistics; 1999-2009 Incidence and Mortality Web-based Report. Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention and National Cancer Institute; 2013.
- Winer R, Hughes J, Feng Q, et al. Condom use and the risk of genital human papillomavirus infection in young women. N Engl J Med 2006;354:2645–54.
- Winer R, Lee S, Hughes J, et al. Genital human papilloma-virus infection incidence and risk factors in a cohort of female university students. Am J Epidemiol 2003;157:218-26.
- Page last reviewed: November 15, 2016
- Page last updated: August 5, 2015
- Content source: