Subacute combined degeneration of spinal cord
Subacute combined degeneration of spinal cord, also known as Lichtheim's disease,[1][2] refers to degeneration of the posterior and lateral columns of the spinal cord as a result of vitamin B12 deficiency (most common), vitamin E deficiency,[3] and copper deficiency.[4] It is usually associated with pernicious anemia.
| Subacute combined degeneration of spinal cord | |
|---|---|
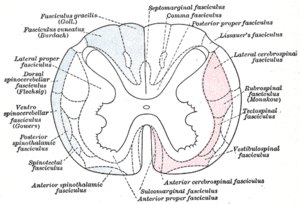 | |
| Diagram of the principal fasciculi of the spinal cord. (In subacute combined degeneration of spinal cord, the "combined" refers to the fact that the dorsal columns and lateral corticospinal tracts are both affected, in contrast to tabes dorsalis which is selective for the dorsal columns.) | |
| Specialty | Neurology |
Signs and symptoms
The onset is gradual and uniform. The pathological findings of subacute combined degeneration consist of patchy losses of myelin in the dorsal and lateral columns. Patients present with weakness of legs, arms, trunk, tingling and numbness that progressively worsens. Vision changes and change of mental state may also be present. Bilateral spastic paresis may develop and pressure, vibration and touch sense are diminished. A positive Babinski sign may be seen.[5] Prolonged deficiency of vitamin B12 leads to irreversible nervous system damage. HIV-associated vacuolar myelopathy can present with a similar pattern of dorsal column and corticospinal tract demyelination.
It has been thought that if someone is deficient in vitamin B12 and folic acid, the vitamin B12 deficiency must be treated first. However, modern research says ″Although it was thought that folic acid might exacerbate vitamin B12 deficiency and its symptoms, it is probably not the case″.[6] And that if this were the case then ″mechanisms by which folic acid exacerbates vitamin B12 deficiency remain unclear″[7]
Administration of nitrous oxide anesthesia can precipitate subacute combined degeneration in people with subclinical vitamin B12 deficiency, while chronic nitrous oxide exposure can cause it even in persons with normal B12 levels. Posterior column dysfunction decreases vibratory sensation and proprioception (joint sense). Lateral corticospinal tract dysfunction produces spasticity and dorsal spinocerebellar tract dysfunction causes ataxia.
Cause
This condition can be due to a dietary deficiency of B12, malabsorption of B12 in the terminal ileum, lack of intrinsic factor secreted from gastric parietal cells, low gastric pH inhibiting attachment of intrinsic factor to ileal receptors.[8]
Vitamin E deficiency, which is associated with malabsorption disorders such as cystic fibrosis and Bassen-Kornzweig syndrome,[9] can cause a similar presentation due to the degeneration of the dorsal columns.[3]
Diagnosis
Serum B12, methylmalonic acid, Schilling test, Complete Blood Count- looking for megaloblastic anemia if there is also folic acid deficiency or macrocytic anemia. The Schilling Test is no longer available in most areas.[10]
MRI- T2 images may reveal increased signal within the white matter of the spinal cord predominately in the posterior columns but also may be in the spinothalamic tracts.
Treatment
Therapy with vitamin B12 results in partial to full recovery where SACD has been caused by a B12 deficiency, depending on the duration and extent of neurodegeneration.
References
- synd/492 at Who Named It?
- L. Lichtheim. Zur Kenntnis der perniciösen Anämie. Verhandlungen des Deutschen Kongress für innere Medizin, 1889, 6: 84-96. 42: 1887.
- Agamanolis, Dimitri P. (July 2014). "Nutritional CNS Disorders". Retrieved 13 September 2014.
Clinically, vitamin E deficiency causes a sensory peripheral neuropathy, ataxia, retinitis pigmentosa, and skeletal and cardiac myopathy. Neuropathological examination in such cases reveals loss of dorsal ganglionic neurons with degeneration of their peripheral and central axons (peripheral neuropathy and posterior column degeneration respectively). Neuroaxonal swellings are seen in the gracile and cuneate nuclei. Similar changes can be produced in rats and monkeys with experimental vitamin E deprivation.
- Kumar N, Gross JB Jr, Ahlskog JE. Copper deficiency myelopathy produces a clinical picture like subacute combined degeneration. Neurology. 2004 Jul 13;63(1):33-9.
- Hemmera B et al. Subacute combined degeneration: clinical, electrophysiological, and magnetic resonance imaging findings. J Neurol Neurosurg Psychiatry 1998;65:822-827 doi:10.1136/jnnp.65.6.822
- https://www.cambridge.org/core/services/aop-cambridge-core/content/view/D8C38CD6D49977957C5B098623459519/S0029665107005873a.pdf/div-class-title-folate-and-vitamin-b-span-class-sub-12-span-friendly-or-enemy-nutrients-for-the-elderly-a-href-fn001-ref-type-fn-a-div.pdf
- https://oup.silverchair-cdn.com/oup/backfile/Content_public/Journal/nutritionreviews/74/7/10.1093_nutrit_nuw015/3/nuw015.pdf?Expires=1488023069&Signature=YwLo2YqL~dkimRwBF3eZ3TgB6IdtIU3PutgyACZruOlY9l1oVZhPLmOhkTfvLKX5N7IJWvWKb3rntY3ECOclDE47wHFHkrGpR1HTPYyQdQF55~13228rSMEfY1g1eAtMlqXBfduGQZ7f0Wh6-68eA4zlK4iuRtYbEMjIz8sP~96D8WlNqnjqhIn-AMPOFtKKqVGkYQF8MXtm7~mPzP9SxxmZ09pozWnet6X3pX8yB0Gx11HvNqk8mi2c5tponqc3iJeIHbZFoXHHayyJXrRokg3wXUoEpixgJom2klTTZ05Cs6SoQNxYHphagm0lPuXQ9Ly8G76lWPg4AQjuQh5rlg__&Key-Pair-Id=APKAIUCZBIA4LVPAVW3Q
- Greenburg, Mark (2010). Handbook of Neurosurgery 7th Edition. New York: Thieme Publishers. pp. 1187–1188. ISBN 978-1-60406-326-4.
- Agamanolis, Dimitri P. (July 2014). "Nutritional CNS Disorders". Retrieved 13 September 2014.
Deficiency of the lipid-soluble vitamin E occurs in cases of intestinal malabsorption such as cystic fibrosis, congenital biliary atresia, intestinal resection, and abetalipoproteinemia (Bassen-Kornzweig syndrome).
- Carmel, Ralph (2007). "The Disappearance of Cobalamin Absorption Testing: A Critical Diagnostic Loss". The Journal of Nutrition. 137 (11): 2481–2484. doi:10.1093/jn/137.11.2481. PMID 17951489.
External links
| Classification | |
|---|---|
| External resources |