Dementia with Lewy bodies
Dementia with Lewy bodies (DLB) is a type of dementia accompanied by changes in behavior, cognition, and movement.[1] As a progressive illness,[7] it is usually diagnosed when cognitive decline interferes with normal daily functioning.[1][8] A core feature is REM sleep behavior disorder (RBD), in which people lose normal muscle paralysis during REM sleep and act out their dreams.[1] Memory loss is not always an early symptom;[9] RBD may appear years or decades before other symptoms.[6] Other frequent symptoms include visual hallucinations, marked fluctuations in attention or alertness, slowness of movement, trouble walking, and rigidity.[1] The autonomic nervous system is usually affected, resulting in changes in blood pressure, heart function, and gastrointestinal function, with constipation as a common symptom.[10] Mood changes such as depression and apathy are also common.[1]
| Dementia with Lewy bodies | |
|---|---|
| Other names | Diffuse Lewy body disease, cortical Lewy body disease, senile dementia of Lewy type |
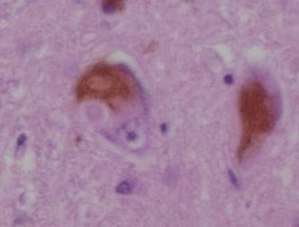 | |
| Microscopic image of Lewy bodies | |
| Specialty | Neurology, psychiatry |
| Symptoms | Dementia, abnormal behavior during REM sleep, fluctuations in alertness, visual hallucinations, slowness of movement[1] |
| Usual onset | After the age of 50[2] |
| Duration | Long term[3] |
| Causes | Unknown[3] |
| Diagnostic method | Based on symptoms and biomarkers[1] |
| Differential diagnosis | Alzheimer's or Parkinson's disease, Parkinson's disease dementia, or certain mental illnesses, vascular dementia[4][5] |
| Medication | Acetylcholinesterase inhibitors such as donepezil and rivastigmine,[1] melatonin[6] |
| Prognosis | Average survival 8 years from diagnosis[3] |
| Frequency | 0.4% (> 65 years old)[2] |
The exact cause is unknown,[3] but involves widespread deposits of abnormal clumps of alpha-synuclein protein known as Lewy bodies in neurons, as well as Lewy neurites.[11][12] DLB is not usually inherited, but there is a genetic association in a small number of families.[3] A probable diagnosis is made based on symptoms and biomarkers; which may include blood tests, neuropsychological tests, medical imaging, and polysomnography.[1][13] Other conditions that share some symptoms of DLB include Alzheimer's disease (AD), Parkinson's disease, delirium, and rarely, psychosis.[9]
There is no cure, and no medication can modify its progression.[3] Treatments aim to relieve some of the symptoms[3] and reduce the burden on caregivers.[8][14][15] Acetylcholinesterase inhibitors, such as donepezil and rivastigmine, are effective at improving cognition and overall functioning, and melatonin can be used for sleep-related symptoms.[1] Antipsychotics are usually avoided, even for hallucinations, because people with DLB are sensitive to them,[1] and their use can result in death.[16] Medications for one symptom may worsen another.[11]
DLB is one of the three most common types of dementia, along with Alzheimer's, and vascular dementia.[13][17][lower-alpha 1] Together with Parkinson's disease dementia, it is one of two dementias classified as the Lewy body dementias.[4] It typically begins after the age of 50, and about 0.4% of people over 65 are affected.[2] People in the latter stages of DLB may be unable to care for themselves.[18] Life expectancy following diagnosis is about eight years.[3] The abnormal deposits of protein that are the underlying mechanism of the disease were discovered in 1912 by Frederic Lewy, and diffuse Lewy body disease was first described by Kenji Kosaka in 1976.[7]
Classification
Dementia with Lewy bodies (DLB) is a progressive neurodegenerative dementia.[7] Together with Parkinson's disease dementia, it is one of the Lewy body dementias,[4] which are also classified as atypical parkinsonian syndromes.[2] It is one of the synucleinopathies—neurodegenerative diseases that are due to an abnormal accumulation of alpha-synuclein protein in the brain—along with Parkinson's disease, multiple system atrophy, and other rarer conditions.[19]
Signs and symptoms
The alpha-synuclein protein deposits causing DLB can damage different regions of the nervous system, including multiple brain regions in the central nervous system, and the autonomic nervous system.[20] This widespread damage can affect several domains of functioning,[lower-alpha 2] resulting in a disease that is more complex than many other dementias, with widely varying symptoms.[16][18] The symptoms can be divided into essential, core, and supportive features.[7]
An identifiable prodromal phase occurs in DLB; the earliest signs are constipation and dizziness from autonomic dysfunction, reduced ability to smell, visual hallucinations, and REM sleep behavior disorder (RBD).[21] DLB is distinguishable from AD even in the prodromal phase.[21]
Essential features
According to the 2017 Fourth Consensus Report of the DLB Consortium, dementia is diagnosed on the occurrence of a "progressive cognitive decline of sufficient magnitude to interfere with normal social or occupational functions, or with usual daily activities.”[1] While dementia is an essential feature of DLB, it does not always appear early on, and is more likely to present as the condition progresses[1][8]—typically after age 55[4]—and memory loss is not always noticeable in the early stages.[9]
In contrast to AD, where the hippocampus is among the first brain structures affected, and episodic memory loss related to encoding of memories is typically the earliest symptom, memory impairment occurs later in DLB.[4][22] Memory loss in DLB has a different progression from AD because frontal structures are involved earlier, with later involvement of temporoparietal brain structures.[22] Deterioration in memory function occurs because new memories may be encoded, but not retrieved.[4][22] Verbal memory is not as severely affected as in AD.[22]
Core features
While specific symptoms may vary, core features—based on "diagnostic specificity and the volume of good-quality evidence available"[1]—designated by the 2017 DLB Consortium are:[1]
- fluctuating cognition, alertness or attention
- REM sleep behavior disorder
- one or more of the cardinal features of parkinsonism, not due to medication or stroke
- repeated visual hallucinations[1]
Impaired attention, executive function, and visuospatial function are common symptoms and are present early in the course of the disease.[1][4] Karantzoulis and Galvin write, "marked attentional and executive function disturbance is central" and "attentional disturbance may serve as the basis of fluctuating cognition that is characteristic".[22] Individuals with DLB may be easily distracted, have a hard time focusing on tasks,[22] or appear to be "delirium-like", "zoning out", or in states of altered consciousness.[1] They may have disorganized speech and their ability to organize their thoughts may change during the day.[1][4] Problems with executive function surface in activities requiring planning and organizing.[2] Deficits can present with impaired job performance, inability to follow conversations, difficulties with multitasking, or with driving-such as misjudging distances or becoming lost.[4] A person with DLB may experience problems of wakefulness or sleep disorders including daytime sleepiness, drowsiness or napping more than two hours a day, insomnia, and restless legs syndrome.[13]
and dementia with Lewy bodies
—B. Tousi (2017), Diagnosis and Management of Cognitive and Behavioral Changes in Dementia With Lewy Bodies.[9]
REM sleep behavior disorder is a parasomnia in which individuals with RBD lose the paralysis of muscles (atonia) normal during rapid eye movement (REM) sleep, and act out their dreams or have other abnormal movements or vocalizations.[8] About 80% of those with DLB have RBD.[6] Abnormal sleep behaviors may begin before cognitive decline is observed,[1] and may appear decades before any other symptoms, often as the first clinical indication of DLB and an early sign of a synucleinopathy.[6] On autopsy, 94 to 98% of individuals with polysomnography-confirmed RBD have a synucleinopathy—most commonly DLB or Parkinson's disease,[8][15][16] in about equal proportions.[23] Other symptoms of the specific synucleinopathy usually manifest within 15 years of the diagnosis of RBD,[11] but may emerge up to 50 years after RBD diagnosis.[8] RBD may subside over time.[1]
Individuals with RBD may not be aware that they act out their dreams.[23] RBD behaviors may include yelling, screaming, laughing, crying, unintelligible talking, nonviolent flailing, or more violent punching, kicking, choking, or scratching.[6][11] The reported dream enactment behaviors are frequently violent,[4] and involve a theme of being chased or attacked.[16] People with RBD may fall out of bed or injure themselves or their bed partners,[1][6][16] with possible resulting bruises, fractures, or subdural hematomae.[8] However, because people are more likely to remember or report violent dreams and behaviors—and to be referred to a specialist when injury occurs—recall or selection bias may explain the prevalence of violence reported in RBD.[6]
Parkinsonism occurs in more than 85% of people with DLB, who may have one or more of the cardinal features that occur in Parkinson's disease—slowness of movement, rigidity,[1] and less commonly, tremor at rest.[4] Motor symptoms may include shuffling gait, problems with balance, falls, blank expression, reduced range of facial expression, and low speech volume or a weak voice.[13] Presentation of motor symptoms is variable, but they are usually symmetric, presenting on both sides of the body.[4] For a DLB diagnosis, only one of the cardinal symptoms of parkinsonism need be present,[1] and the symptoms may be less severe than in persons with Parkinson's disease.[9]
Visual hallucinations are defined by Pezzoli et al. as "well-formed images perceived without the presence of real stimuli".[24] Up to 80% of people with DLB have visual hallucinations, typically early in the course of the disease.[1][25] They are recurrent and frequent; may be scenic, elaborate and detailed;[24][25] and usually involve animated perceptions of animals or people, including children and family members.[4]
These hallucinations can sometimes provoke fear, although their content is more typically neutral.[4] In some cases, the person with DLB may have insight that the hallucinations are not real.[15][25] Individuals with visual hallucinations and one of the Lewy body dementias generally have more severe cognitive impairment.[24] Among those with more disrupted cognition, the hallucinations can become more complex, and they may be less aware that their hallucinations are not real.[24]
Different from visual hallucinations, but also common in DLB, are visual misperceptions or illusions, explained by Pezzoli et al. as "incorrect perceptions of real stimuli".[24] Persons with DLB may have problems with vision (for example, at night) and misinterpret what they see (for example, mistaking a pile of socks for snakes or a clothes closet for the bathroom).[4]
Supportive features
According to the DLB Consortium, although "carrying less diagnostic weight, supportive items are often valuable in clinical decision-making, acting as signposts to or adding evidence for a DLB diagnosis".[1] Supportive features may persist over time, be present early in the progression of DLB, and are common, but they are not specific to the diagnosis. The supportive features are:[1]
- marked sensitivity to antipsychotics (neuroleptics)
- marked dysautonomia (autonomic dysfunction) in which the autonomic nervous system does not work properly
- hallucinations in senses other than vision (hearing, touch, taste, and smell[9])
- hypersomnia (excessive sleepiness)
- hyposmia (reduced ability to smell)
- false beliefs and delusions organized around a common theme
- postural instability, loss of consciousness, and frequent falls
- apathy, anxiety or depression[1][7]
.jpg)
Marked sensitivity to antipsychotics can occur. Antipsychotic treatment of people with DLB results in adverse reactions about half of the time,[11] and can be fatal after a single dose.[15] The Fourth Consensus Report continues to caution against the use of antipsychotics (neuroleptics) for people with DLB.[1] Partly because of dopamine cell loss, people with DLB may have neuroleptic malignant syndrome, impairments in cognition or alertness, or irreversible exacerbation of parkinsonism including severe rigidity,[4] and dysautonomia from the use of antipsychotics.[15] Antipsychotic medications with D2 dopamine receptor-blocking properties are used only with great caution.[9]
Dysautonomia (autonomic dysfunction) occurs when Lewy pathology affects the peripheral autonomic nervous system or the nerves that serve organs such as the intestines, heart, and urinary tract.[20] The first signs of autonomic dysfunction are often subtle.[6] Symptoms include blood pressure problems, such as dizziness after quickly standing up and supine hypertension; constipation, urinary problems, and sexual dysfunction;[10] loss of or reduced ability to smell;[6][9] and excessive sweating, drooling, or salivation, and problems swallowing.[9][11]
Alpha-synuclein deposits can affect cardiac muscle and blood vessels.[10] According to Yamada et al., "[d]egeneration of the cardiac sympathetic nerves is a neuropathological feature" of the Lewy body dementias.[26] Almost all people with synucleinopathies have cardiovascular dysfunction, although most are asymptomatic; 50–60% of individuals with DLB have orthostatic hypotension due to reduced blood flow,[10] which results in symptoms of lightheadedness, feeling faint, and blurred vision.[10]
From chewing to defecation, alpha-synuclein deposits affect every level of gastrointestinal function. Almost all persons with DLB have upper gastrointestinal tract dysfunction (such as delayed gastric emptying) or lower gastrointestinal dysfunction (such as constipation and prolonged stool transit time).[10] Persons with Lewy body dementias almost universally experience nausea, gastric retention, or abdominal distention from delayed gastric emptying.[10] Constipation can present a decade before diagnosis.[27] Difficulty swallowing is milder than in other synucleinopathies, and presents later in the course of the disease.[10]
Urinary difficulties (urinary retention, waking at night to urinate, increased urinary frequency and urgency, and over- or underactive bladder) typically appear later and may be mild to moderate.[10] Sexual dysfunction usually appears early in synucleinopathies, and may include erectile dysfunction, and difficulties achieving orgasm or ejaculating.[10]
Among the other supportive features, psychiatric symptoms are often present when the individual first comes to clinical attention and more likely, compared to AD, to cause more impairment.[22] Anxiety and depression are more common in DLB than in the general population, and may have been present for decades.[11][16] Anxiety leads to increased risk of falls,[9] and apathy may lead to less social interaction.[13]
Agitation, behavioral disturbances,[16] and delusions typically appear later in the course of the disease.[4] Delusions may have a paranoid quality, revolving around themes like a house being broken in to, infidelity,[4] or abandonment.[9] Individuals with DLB who misplace items may have delusions centered around theft.[4] Capgras delusion may occur, where the person with DLB loses knowledge of the spouse, caregiver, or partner's face,[25] and is convinced that an imposter has replaced the caregiver.[4] Hallucinations in other modalities are sometimes present, but are less frequent.[9]
Sleep disorders are common in DLB and may lead to hypersomnia; these include disrupted sleep cycles, sleep apnea, and arousal from periodic limb movement disorder.[11] Loss of sense of smell may occur several years before other symptoms.[4]
Medications (including tricyclic antidepressants and treatments for urinary incontinence) with anticholinergic properties that cross the blood-brain barrier can cause memory loss; dopamine agonists may lead to psychosis; and the antihistamine medication diphenhydramine (Benadryl), sleep medications like zolpidem,[28] and benzodiazepines may worsen confusion[4] or neuropsychiatric symptoms.[15] Some general anesthetics may cause confusion or delirium upon waking in persons with Lewy body dementias, and may result in permanent decline.[13]
Causes
The exact cause of DLB[13]—indeed the cause of synucleinopathies—is not known,[23] but many factors probably are present,[11] including both genetic and environmental influences.[23] Less than 10% of cases can be accounted for by inheritance of a single gene, while in most cases, genetic and environmental factors mediate other disease processes to cause synucleinopathies;[23] these other processes include "mitochondrial or autosomal-lysomal autophagy system dysfunction, inflammation, endoplasmic reticulum stress, or even prion-like infection".[23]
The genetics are not well studied because the large homogeneous DLB populations needed for genetic studies have not been identified.[7] DLB is not usually inherited, but there is a genetic association in a small number of families.[3] DLB risk is heightened with inheritance of the ε4 allele of the apolipoprotein E (APOE) gene,[7] and mutations in the PARK11 and GBA genes are associated with DLB.[12] Further, genetic overlap exists among dementia with Lewy bodies, Parkinson's disease, Parkinson's disease dementia, and Alzheimer's disease.[7][11] Also, RBD is found more often among individuals who have GBA and SNCA mutations.[7]
Having REM sleep behavior disorder, having another family member with DLB, and age over 50 are risk factors for developing DLB.[13] Additional risk factors for rapid conversion of RBD to a synucleinopathy are impairments in color vision or the ability to smell, mild cognitive impairment, and abnormal dopamingeric imaging.[23]
Pathophysiology
_of_alpha-synuclein_in_Lewy_Bodies_and_Lewy_Neurites_in_the_neocortex_of_a_patient_with_Lewy_Body_Disease.jpg)
DLB is characterized by the development of abnormal collections of alpha-synuclein protein within neurons, known as Lewy bodies and Lewy neurites in diseased neurons.[11][12] When these clumps of protein form in neurons, those neurons function less optimally and die.[18] Damage in the brain is widespread, and affects many domains of functioning.[18][lower-alpha 2] In DLB, loss of acetylcholine-producing neurons is thought to account for degeneration in memory and learning, while the death of dopamine-producing neurons appears to be responsible for degeneration of "behavior, cognition, movement, motivation, sleep, and mood".[13]
The amount of Lewy body pathology correlates with the extent of dementia in the Lewy body disorders, but amyloid imaging and autopsy studies indicate that tau protein pathology and amyloid plaques,[30] hallmarks of AD,[22][31] are also common.[12] Amyloid-beta (Aβ) deposits are found in the tauopathies, neurodegenerative diseases characterized by neurofibrillary tangles of hyperphosphorylated tau protein,[31] but the mechanism underlying dementia is often mixed, and Aβ is also a factor in DLB.[11]
The precise mechanisms contributing to DLB are not well understood, and a matter of some dispute.[7] The role played by the alpha-synuclein deposits is unclear, because individuals with no signs of DLB have been found on autopsy to have advanced alpha-synuclein pathology.[11] Weil says, "How Lewy pathology relates to dopamingergic degeneration and later to more widespread cell death has remained contentious."[7] It is not known if the pathology spreads between cells or follows another pattern.[7] The mechanisms that contribute to cell death, how the disease advances through the brain, and the timing of cognitive decline are all poorly understood; nor is there a model to account for the specific neurons and brain regions that are affected.[7]
A proposed pathophysiology for RBD implicates cells in the reticular formation that regulate REM sleep. These cells are affected before other brain regions in the Lewy body dementias; this could be a potential explanation for the appearance of RBD often decades earlier than other symptoms.[11]
Diagnosis
Dementia with Lewy bodies can only be definitively diagnosed after death with an autopsy of the brain[13]—diagnosis of the living is referred to as probable or possible.[1] DLB is often misdiagnosed or confused in its early stages with AD.[9] Another complicating factor is that DLB can occur along with Alzheimer's; autopsy may reveal previously undiagnosed Lewy bodies in as many as half of people with AD.[1] Despite the difficulty in diagnosis, a prompt diagnosis is important because of the serious risks of sensitivity to antipsychotic medications and the need to inform both the person with DLB and the person's caregivers about potentially irreversible side effects of those medications.[4] In comparison to many other neurodegenerative diseases, the management of DLB is difficult, so an accurate diagnosis is important.[16]
Criteria
The 2017 Fourth Consensus Report established diagnostic criteria for probable and possible DLB, in recognition of advances in detection and improvements from the earlier Third Consensus (2005)[32] version. The 2017 criteria are based on essential, core, and supportive clinical features, and diagnostic biomarkers.[1]
The essential feature is dementia; for a DLB diagnosis, it must be sufficient to interfere with social or occupational functioning.[1]
The four core clinical features (described in the Signs and symptoms section) are fluctuating cognition, visual hallucinations, REM sleep behavior disorder, and signs of parkinsonism. Supportive clinical features are marked sensitivity to antipsychotics, marked autonomic dysfunction, nonvisual hallucinations, hypersomnia, reduced ability to smell, false beliefs and delusions organized around a common theme, postural instability, loss of consciousness and frequent falls, apathy, anxiety, or depression.[1][7]

The diagnostic biomarkers are:[1]
Indicative
- reduced dopamine transporter uptake in the basal ganglia shown on PET or SPECT imaging
- low uptake of 123iodine-metaiodobenzylguanidine (123I-MIBG) shown on myocardial scintigraphy
- loss of atonia during REM sleep evidenced on polysomnography
Supportive (from PET, SPECT, CT, or MRI brain imaging studies, or EEG monitoring):[1][7]
- lack of damage to medial temporal lobe
- reduced occipital activity
- prominent slow-wave activity
Probable DLB can be diagnosed when dementia and at least two core features are present, or one core feature with at least one indicative biomarker is present. Possible DLB can be diagnosed when dementia and only one core feature are present or, if no core features are present, at least one indicative biomarker presents.[1]
DLB is distinguished from Parkinson's disease dementia by the time frame in which dementia symptoms appear relative to Parkinson symptoms. DLB is diagnosed when cognitive symptoms begin before or at the same time as parkinsonism. Parkinson's disease dementia would be the diagnosis when Parkinson's disease is well established before the dementia occurs; that is, the onset of dementia is more than a year after the onset of parkinsonian symptoms.[1]
DLB is listed in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) as major or mild neurocognitive disorder with Lewy bodies.[11] The differences between the DSM and DLB Consortium criteria are: 1) the DSM does not include low dopamine transporter uptake as a supportive feature, and 2) unclear diagnostic weight is assigned to biomarkers in the DSM.[11]
Clinical history and testing
Diagnostic tests can be used to establish some features of the condition and distinguish them from symptoms of other conditions; diagnosis may include the person's medical history, physical exam, assessment of neurological function, testing to rule out conditions that may cause similar symptoms, brain imaging, neuropsychological testing to assess cognitive function,[13][33] sleep studies, or myocardial scintigraphy.[1] Laboratory testing can rule out conditions such as depression, abnormal thyroid function, syphilis, HIV, or vitamin deficiencies that may cause symptoms similar to dementia.[33][34]
Dementia screening tests are the Mini-Mental State Examination,[1][35] the Montreal Cognitive Assessment, and others.[9][lower-alpha 3] For tests of attention, digit span, serial sevens, and spatial span can be used for simple screening, and the Revised Digit Symbol Subtest of the Wechsler Adult Intelligence Scale may show defects in attention that are characteristic of DLB.[36] The Frontal Assessment Battery, Stroop test and Wisconsin Card Sorting Test are used for evaluation of executive function, and there are many other screening instruments available.[37]

If DLB is suspected when parkinsonism and dementia are the only presenting features, PET or SPECT imaging may show reduced dopamine transporter activity. A DLB diagnosis may be warranted if other conditions with reduced dopamine transporter uptake can be ruled out.[1][4]
RBD is diagnosed either by sleep study recording or, when sleep studies cannot be performed, by medical history and validated questionnaires.[1][8][lower-alpha 4] In individuals with dementia and a history of RBD, a probable DLB diagnosis can be justified (even with no other core feature or biomarker) based on a sleep study showing REM sleep without atonia because it is so highly predictive.[1] Conditions similar to RBD, like severe sleep apnea and periodic limb movement disorder, must be ruled out.[1] Prompt evaluation and treatment of RBD is indicated when a prior history of violence or injury is present as it may increase the likelihood of future violent dream enactment behaviors.[6] Individuals with RBD may not be able to provide a history of dream enactment behavior, so bed partners are also consulted.[1][6] The REM Sleep Behavior Disorder Single-Question Screen offers diagnostic sensitivity and specificity in the absence of polysomnography with one question:[8] "Have you ever been told, or suspected yourself, that you seem to 'act out your dreams' while asleep (for example, punching, flailing your arms in the air, making running movements, etc.)?"[9]
Since 2001, 123iodine-metaiodobenzylguanidine (123I-MIBG) myocardial scintigraphy has been used diagnostically in East Asia and Japan.[9][38][39] MIBG is taken up by sympathetic nerve endings, such as those that innervate the heart, and is labeled for scintigraphy with radioactive 123iodine.[39] Autonomic dysfunction resulting from damage to nerves in the heart in patients with DLB is associated with lower cardiac uptake of 123I-MIBG.[39]
There is no genetic test to determine if an individual will develop DLB[1][13] and, according to the Lewy Body Dementia Association, genetic testing is not routinely recommended because there are only rare instances of hereditary DLB.[40]
Differential
Many neurodegenerative conditions share cognitive and motor symptoms with dementia with Lewy bodies. The differential diagnosis includes Alzheimer's disease; such synucleinopathies as Parkinson's disease dementia, Parkinson's disease, and multiple system atrophy; vascular dementia; and progressive supranuclear palsy, corticobasal degeneration, and corticobasal syndrome.[4]
Lewy pathology affects the peripheral autonomic nervous system; autonomic dysfunction is observed less often in Alzheimer's, frontotemporal, or vascular dementias, so its presence can help differentiate them.[41]
Alzheimer's disease. Short-term memory impairment is seen early in AD and is a prominent feature, while fluctuating attention is uncommon; impairment in DLB is more often seen first as fluctuating cognition.[4] While 74% of people with autopsy-confirmed DLB had deficits in planning and organization, they show up in only 45% of people with AD.[11] In AD, it is unclear if executive function is impacted early.[22] Visuospatial processing deficits are present in most individuals with DLB,[11] and they show up earlier and are more pronounced than in AD.[22] Hallucinations typically occur early in the course of DLB, are less common in early AD, but usually occur later in AD.[4][25] AD pathology frequently co-occurs in DLB, so the cerebrospinal fluid testing for Aβ and tau protein that is often used to detect AD is not useful in differentiating AD and DLB.[4]
PET or SPECT imaging can be used to detect reduced dopamine transporter uptake and distinguish AD from DLB.[4][30] Severe atrophy of the hippocampus is more typical of AD than DLB.[4] In East Asia and Japan, 123I-MIBG is used in the differential diagnosis of DLB and AD, because reduced labeling of cardiac nerves is seen only in Lewy body disorders.[9][39] Other indicative and supportive biomarkers are useful in distinguishing DLB and AD (preservation of medial temporal lobe structures, reduced occipital activity, and slow-wave EEG activity).[1]
Synucleinopathies. Dementia with Lewy bodies and Parkinson's disease dementia are clinically similar after dementia occurs in Parkinson's disease.[11] Delusions in Parkinson's disease dementia are less common than in DLB,[4] and persons with Parkinson's disease are typically less caught up in their visual hallucinations than those with DLB.[25] There is a lower incidence of tremor at rest in DLB than in Parkinson's disease, and signs of parkinsonism in DLB are more symmetrical.[6] In multiple system atrophy, autonomic dysfunction appears earlier and is more severe, and is accompanied by uncoordinated movements, while visual hallucinations and fluctuating cognition are less common than in DLB.[4] Urinary difficulty is one of the earliest symptoms with multiple system atrophy, and is often severe.[10]
Frontotemporal. Corticobasal syndrome, corticobasal degeneration and progressive supranuclear palsy are frontotemporal dementias[42] with features of parkinsonism and impaired cognition. Similar to DLB, imaging may show reduced dopamine transporter uptake. According to Gomperts, "[c]areful history and examination remain the method of choice"[4] for distinguishing corticobasal syndrome and degeneration, and progressive supranuclear palsy, from DLB. Motor movements in corticobasal syndrome are asymmetrical. There are differences in posture, gaze and facial expressions in the most common variants of progressive supranuclear palsy, and falling backwards is more common relative to DLB. Visual hallucinations and fluctuating cognition are unusual in corticobasal degeneration and progressive supranuclear palsy.[4]
Vascular dementia. MRI scans almost always show abnormalities in the brains of people with vascular dementia, which can begin suddenly.[43] The Dementia Cognitive Fluctuation Scale is a screening questionnaire used to measure fluctuating attention and alertness that has shown promise in distinguishing between DLB and vascular dementia, but as of 2014, it had not been fully validated.[4]
Other. The symptoms of DLB are easily confused with delirium,[14] or more rarely as psychosis.[9] Mismanagement of delirium is a particular concern because of the risks to people with DLB associated with antipsychotics.[14] Dopamine transporter imaging can help distinguish DLB from delirium.[14]
Management
Only palliative care can be offered,[7] as there are no medications which will modify the course of the disease.[12] No medications for DLB are approved by the United States Food and Drug Administration as of 2017,[9] although donepezil is licensed in Japan for the treatment of DLB.[44] Management can be challenging because of the need to balance treatment of cognitive dysfunction, neuropsychiatric features, impairments related to the motor system,[4] and other nonmotor symptoms.[1] A multidisciplinary approach, going beyond early and accurate diagnosis to include educating and supporting the caregivers, is favored by the 2017 DLB Consortium.[1]
Pharmaceutical
—B.P. Boot (2015), Comprehensive treatment of dementia with Lewy bodies[16]
Pharmacological management of DLB is complex because of adverse effects to medications[11] and the wide range of symptoms to be treated (cognitive, motor, neuropsychiatric, autonomic, and sleep).[1][16] Anticholinergic and dopaminergic agents can have adverse effects or result in psychosis in individuals with DLB,[1] and a medication that addresses one feature might worsen another.[11] For example, acetylcholinesterase inhibitors (AChEIs) for cognitive symptoms can lead to complications in dysautonomia features; treatment of movement symptoms with dopaminergic agents may worsen neuropsychiatric symptoms; and treatment of hallucinations and psychosis with antipsychotics may worsen other symptoms or lead to a potentially fatal reaction.[16]
Extreme caution is required in the use of antipsychotic medication in people with DLB because of their sensitivity to these agents.[1] According to Boot (2013), "electing not to use neuroleptics is often the best course of action".[15] People with Lewy body dementias who take neuroleptics are at risk for neuroleptic malignant syndrome, a life-threatening illness.[4] There is little evidence to support the use of antipsychotics to treat the Lewy body dementias, and they carry the additional risk of stroke when used in the elderly with dementia.[11]
Cognitive symptoms. There is strong evidence for the use of AChEIs to treat cognitive problems.[12] Donepezil (Aricept) was licensed in 2014 in Japan for the treatment of DLB,[44] and rivastigmine (Exelon) has a strong evidence base for treating cognitive symptoms.[16] Even if the AChEIs do not lead to improvement in cognitive symptoms, people taking them may have less deterioration,[1] although there may be adverse gastrointestinal effects.[11] The AChEIs are initiated carefully as they may aggravate autonomic dysfunction or sleep behaviors.[16] DLB may be more responsive than AD to donepezil.[45] There is less evidence for the efficacy of memantine in DLB, but it may be used alone or with an AChEI because of its low side effect profile.[1] Anticholinergic drugs are avoided because they worsen cognitive symptoms.[11]
To improve daytime alertness, there is mixed evidence for the use of stimulants such as methylphenidate and dextroamphetamine; although worsening of neuropsychiatric symptoms is not common, they can increase the risk of psychosis.[15][16] In the US, modafinil and armodafinil are not always covered by insurance, but may be effective for daytime sleepiness.[15][16]
Motor symptoms appear to respond in DLB somewhat less to the medications used to treat Parkinson's disease, like levodopa, and neuropsychiatric symptoms can be increased.[1] If such medications are needed for motor symptoms, cautious introduction with slow increases to the lowest possible dose may help avoid psychosis.[1]
Neuropsychiatric symptoms. The first line of defense in reducing visual hallucinations is to reduce the use of dopaminergic drugs, which can worsen hallucinations.[11] Although it has been shown effective in Parkinson's disease, there is limited evidence for the use of clozapine to treat visual hallucinations in DLB, and its use requires regular blood monitoring.[11] Quetiapine is relatively safe[1] and well-tolerated for psychosis and agitation in DLB, but there is little evidence for its efficacy.[11]
Apathy may be treated with AChEIs, and they may also reduce hallucinations and delusions; reduction in anxiety and agitation may be a secondary effect.[1] Mirtazapine and SSRIs can be used to treat depression, depending on how well they are tolerated, and guided by general advice for the use of antidepressants in dementia.[1] Antidepressants can worsen RBD,[9] and antidepressants with anticholinergic properties may worsen hallucinations and delusions.[11] People with Capgras syndrome may not tolerate AChEIs.[9]
Sleep disorders. Injurious dream enactment behaviors are a treatment priority.[6] RBD may be treated with melatonin or clonazepam.[8] Melatonin may be more helpful in preventing injuries,[6] and it offers a safer alternative, because clonazepam can produce deteriorating cognition,[1] and worsen sleep apnea.[6] For some people, memantine or AChEIs are useful.[11] No trials support its use in DLB, but modafinil may be used for hypersomnia.[11] Mirtazapine can be used for hypersomnia, but it can exacerbate RBD.[11] Antidepressants (SSRIs, SNRIs, tricyclics, and MAOIs), AChEIs, beta blockers, caffeine, and tramadol may worsen RBD.[6]
Autonomic symptoms. Decreasing the dosage of dopaminergic or atypical antipsychotic drugs may be needed with orthostatic hypotension, and high blood pressure drugs can sometimes be stopped.[11] When non-pharmacological treatments for orthostatic hypotension have been exhausted, fludrocortisone, droxidopa, midodrine or atomoxetine are options.[10]
Non-pharmaceutical
There is no high-quality evidence for non-pharmacological management of DLB,[1][12] but some interventions have been shown effective for addressing similar symptoms that occur in other dementias.[46] Organized activities, music therapy, physical activity and occupational therapy may help with psychosis or agitation, while exercise and gait training can help with motor symptoms.[46] Cognitive behavioral therapy can be tried for depression or hallucinations, although there is no evidence for its use in DLB.[11][12] The frequency and severity of RBD may be lessened by treating sleep apnea, if it is present.[8] Cues can be used to help with memory retrieval.[4]
For autonomic dysfunction, several non-medication strategies may be helpful. Dietary changes include avoiding meals rich in carbohydrates[15] and sugary foods, eating smaller and more frequent meals,[10] increasing table salt to reduce orthostatic hypotension, and increasing fluids or dietary fiber to treat constipation.[11] Stool softeners and exercise also help with constipation.[15] Physical exercise in a sitting or recumbent position, and exercise in a pool, helps maintain conditioning when orthostatic hypotension is a problem.[10] Compression stockings and elevating the head of the bed may also help.[11] To lessen the risk of fractures in individuals at risk for falls, bone mineral density screening and testing of vitamin D levels are used,[1] and caregivers are educated on the importance of preventing falls.[16] Physical therapy may be helpful for motor symptoms.[16]
Caregiving
Because of the neuropsychiatric symptoms associated with DLB, the demands placed on caregivers are higher than in AD,[14] but education for caregivers has not been studied as thoroughly as in AD.[1][12] Contributing factors to the caregiver burden in DLB are psychosis, aggression, agitation, and night-time behaviors such as parasomnias,[14] that lead to a loss of independence earlier than in AD.[47] Caregivers may experience depression, exhaustion, and be in need of support.[14] Other family members who are not present in the daily caregiving may not observe the fluctuating behaviors or recognize the stress on the caregiver, and conflict can result when family members are not supportive.[13] Caregiver education reduces not only distress for the caregiver, but symptoms for the individual with dementia.[46]
Visual hallucinations associated with DLB create a particular burden on caregivers;[48] educating caregivers on how to distract or change the subject when confronted with hallucinations is more effective than arguing over the reality of the hallucination.[15][49] Coping strategies may help and are worth trying, even though there is no evidence for their efficacy.[25] These strategies include having the person with DLB look away or look at something else, focus on or try to touch the hallucination, wait for it to go away on its own, and speak with others about the visualization.[25] Delusions and hallucinations may be reduced by increasing lighting in the evening, and making sure there is no light at night when the individual with DLB is sleeping.[15]
With the increased risk of antipsychotics for people with DLB, educated caregivers are able to act as advocates for the person with DLB.[50] If evaluation or treatment in an emergency room is needed, the caregiver may be able to explain that, in the words of Gomperts "patients with DLB are essentially 'allergic' to haloperidol and other neuroleptics".[4] Caregiver training, watchful waiting, identifying sources of pain, and increasing social interaction can help minimize agitation.[16] Individuals with dementia may not be able to communicate that they are in pain, and pain is a common trigger of agitation.[15] Medical alert bracelets or notices about medication sensitivity are available and can save lives.[15]
When RBD is present, individuals and their caregivers need counselling about the need to improve bedroom safety.[8][11][15] Sleep-related injuries from falling or jumping out of bed can be avoided by placing a mattress next to the bed to soften the impact of a fall, and removing sharp objects from around the bed.[11] Sharp surfaces near the bed can be padded, bed alarm systems may help with sleepwalking, and bed partners may find it safer to sleep in another room.[8] According to St Louis and Boeve, firearms should be locked away, out of the bedroom.[8]
Driving ability may be impaired early in DLB because of visual hallucinations, movement issues related to parkinsonism, and fluctuations in cognitive ability, and at some point it becomes unsafe for the person to drive.[51] Driving ability is assessed as part of management and family members generally determine when driving privileges are removed.[15][51]
A home safety assessment can be done when there is risk of falling;[1] handrails and shower chairs can help avoid falls.[15]
Prognosis
The prognosis for DLB has not been well studied; early studies had methodological limitations, such as small sample size and selection bias.[14] DLB generally leads to higher disability, lower life expectancy and a reduced quality of life, with increased costs of care.[14][47] Depression, apathy, and visual hallucinations contribute to the reduced quality of life.[14] Decline may be more rapid when severe visuospatial deficits show up early in the course of the Lewy body dementias,[11] when the APOE gene is present, or when Alzheimer's or its biomarkers is also present.[14] The severity of orthostatic hypotension also predicts a worse prognosis.[16]
Compared to AD, which is better studied, memory is retained longer, while verbal fluency may be lost faster.[14] There are more neuropsychiatric symptoms in DLB than AD, and they may emerge earlier, so according to Mueller, those with DLB "might have a less favourable prognosis, with accelerated cognitive decline, shorter lifespan, and increased admission to residential care".[14] The difference in admissions to hospital and time in nursing care may be explained by the presence of hallucinations.[14] Increased mortality relative to AD may be attributed to a higher risk of injury from falls.[47]
Life expectancy is difficult to predict, and limited study data are available.[14] Survival may be defined from the point of disease onset, or from the (possibly delayed) point of diagnosis.[14] A 2017 review found survival from disease onset between 5.5 and 7.7 years, survival from diagnosis between 1.9 and 6.3 years, and a poorer survival rate than in Alzheimer's.[14] The US National Institute of Neurological Disorders and Stroke writes that people with DLB typically live 8 years following diagnosis, about the same as AD,[3] though some people with Lewy body dementias live for 20 years.[13] Shorter life expectancy is more likely when visual hallucinations, abnormal gait, and variable cognition are present early on.[14] In the late part of the disease, people may be unable to care for themselves.[18] Aspiration pneumonia, a complication of difficulty in swallowing that results from dysautonomia, commonly causes death among people with synucleinopathies.[10]
Epidemiology
The Lewy body dementias are as a group the second most common form of dementia after Alzheimer's disease (AD).[11] DLB itself is one of the three most common types of dementia, along with AD and vascular dementia, with AD making up about half of all cases.[13][17][lower-alpha 1]
The diagnostic criteria for DLB before 2017 were highly specific, but not very sensitive,[15] so that more than half of cases were missed.[47] Dementia with Lewy bodies was under-recognized as of 2015, and there was little data on its epidemiology.[11] The incidence and prevalence of DLB is not known accurately, but estimates are increasing with better recognition of the condition since 2017.[52][53]
About 0.4% of those over the age 65 are affected with DLB,[2] and between 1 and 4 per 1,000 people develop the condition each year.[54][55] Symptoms usually appear between the ages of 50 and 80,[2] and it is not uncommon for it to be diagnosed before the age of 65.[11] DLB was thought to be slightly more common in men than women,[11][47] but a 2014 review challenged that view, and said that the gender distribution was unclear.[47] An estimated 10 to 15% of diagnosed dementias are Lewy body type, but estimates range as high as 24%.[11]
A French study found an incidence among persons 65 years and older almost four times higher than a US study (32 vs 112 per 100,000 person-years), but the US study may have excluded people with only mild or no parkinsonism, while the French study screened for parkinsonism.[11] Neither of the studies assessed systematically for RBD, so DLB may have been underdiagnosed in both studies.[11] A door-to-door study in Japan found a prevalence of 0.53% for persons 65 and older, and a Spanish study found similar results.[56]
History
Frederic Lewy (1885–1950) was the first to discover the abnormal protein deposits (later called "Lewy body inclusions") in the early 1900s.[4][57] In 1912, studying Parkinson's disease (paralysis agitans),[58] he described findings of these inclusions in the vagus nerve, the nucleus basalis of Meynert and other brain regions.[59] He published a book, The Study on Muscle Tone and Movement. Including Systematic Investigations on the Clinic, Physiology, Pathology, and Pathogenesis of Paralysis agitans, in 1923 and except for one brief paper a year later, never mentioned his findings again.[60]
In 1961, Okazaki et al. published an account of diffuse Lewy-type inclusions associated with dementia in two autopsied cases.[4][61] Dementia with Lewy bodies was fully recognized and described in an autopsied case by Japanese psychiatrist and neuropathologist Kenji Kosaka in 1976;[7][62] he first proposed the term Lewy body disease four years later, based on 20 autopsied cases.[9][61] DLB was thought to be rare until it became easier to diagnose in the 1980s after the discovery of alpha-synuclein immunostaining that highlighted Lewy bodies in post mortem brains.[4] Kosaka et al. described thirty-four more cases in 1984, which were mentioned along with four UK cases by Gibb et al. in 1987 in the journal Brain, bringing attention of the Japanese work to the Western world.[63] A year later, Burkhardt et al. published the first general description of diffuse Lewy Body Disease.[64]
With Japanese, UK, and US researchers finding in the 1990s that DLB was a common dementia, there were nonetheless no diagnostic guidelines, and each group was using different terminology.[65] The different groups of researchers began to realize that a collaborative approach was needed if research was to advance.[66] The DLB Consortium was established, and in 1996, the term dementia with Lewy bodies was agreed upon[66] and the first criteria for diagnosing DLB were elaborated.[9]
Two 1997 discoveries highlighted the importance of Lewy body inclusions in neurodegenerative processes: a mutation in the SNCA gene that encodes the alpha-synuclein protein was found in kindreds with Parkinson's disease, and Lewy bodies and neurites were found to be immunoreactive for alpha-synuclein.[67] Thus, alpha-synuclein aggregation as the primary building block of the synucleinopathies was established.[67]
Between 1995 and 2005, the DLB Consortium issued three Consensus Reports on DLB.[68] DLB was included in the fourth text revision of the DSM (DSM-IV-TR, published in 2000) under "Dementia due to other general medical conditions”. In the 2010s, the possibility of a genetic basis began to emerge.[7] The Fourth Consensus Report was issued in 2017, giving increased diagnostic weighting to RBD and 123I-MIBG myocardial scintigraphy.[1]
Society and culture

The British author and poet Mervyn Peake died in 1968 and was diagnosed posthumously as a probable case of DLB in a 2003 study published in JAMA Neurology.[72] Based on signs in his work and letters of progressive deterioration, fluctuating cognitive decline, deterioration in visuospatial function, declining attention span, and visual hallucinations and delusions, his may be the earliest known case where DLB was found to have been the likely cause of death.[72]
Robin Williams, the American actor and comedian, died by suicide on August 11, 2014. He had been diagnosed with Parkinson's disease,[69] and according to his widow he experienced depression, anxiety and increasing paranoia.[70] Upon autopsy his widow said he was found to have diffuse Lewy body disease,[69][70][71] while the autopsy used the term diffuse Lewy body dementia.[73] Dennis Dickson, a spokesperson for the Lewy Body Dementia Association, clarified the distinction between the term used in the autopsy report, diffuse Lewy body dementia—which is more commonly called diffuse Lewy body disease and refers to the underlying disease process—and the umbrella term, Lewy body dementia—which encompasses both PDD and DLB.[73] According to Dickson, "The report confirms he experienced depression, anxiety and paranoia, which may occur in either Parkinson's disease or dementia with Lewy bodies", adding that, in Parkinson's, "Lewy bodies are generally limited in distribution, but in DLB, the Lewy bodies are spread widely throughout the brain, as was the case with Robin Williams."[73] Ian G. McKeith, LBD professor and researcher, commented that Williams' symptoms and autopsy findings were explained by DLB.[74]
Research directions
Cognitive training, deep brain stimulation and transcranial direct-current stimulation have been studied more in Parkinson's and Alzheimer's disease than they have in dementia with Lewy bodies, and all are potential therapies for DLB.[12] Medications that alter the underlying process of alpha-synuclein deposits are yet to be identified.[75]
Future strategies involve interventions to modify the course of the disease using immunotherapy, gene therapy, stem cell therapy, and reducing amyloid beta accumulation.[12] Identification of biomarkers for DLB will enable treatments to begin sooner[12] and improve the ability to select subjects and measure efficacy in clinical trials.[30] As of 2018 there are no well-validated neuroimaging modalities to measure alpha-synuclein in the brains of living people, but this is an active area of research.[30]
Notes
- Kosaka (2017) writes: "Dementia with Lewy bodies (DLB) is now well known to be the second most frequent dementia following Alzheimer disease (AD). Of all types of dementia, AD is known to account for about 50%, DLB about 20% and vascular dementia (VD) about 15%. Thus, AD, DLB, and VD are now considered to be the three major dementias."[17] The NINDS (2017) says that Lewy body dementia "is one of the most common causes of dementia, after Alzheimer’s disease and vascular disease."[13]
- Areas of the brain and function affected:[18]
- cerebral cortex—thought, perception and language
- limbic cortex—emotions and behavior
- hippocampus—memory
- midbrain and substantia nigra—movement
- brainstem—sleep, alertness, and autonomic dysfunction
- hypothalamus—autonomic dysfunction
- olfactory cortex—smell
- Other dementia screening tests are the Parkinson's Disease Cognitive Rating Scale, Parkinson's Neuropsychometric Dementia Instrument, and Scales for Outcomes in Parkinson's Disease–Cognition.[9]
- Questionnaires such as the REM Sleep Behavior Disorder Screening Questionnaire (RBDSQ), the REM Sleep Behavior Questionnaires – Hong-Kong (RBD-HK), the Mayo Sleep Questionnaire (MSQ), the Innsbruck REM Sleep Behavior Disorder Inventory, and the REM Sleep Behavior Disorder Single-Question Screen are well-validated.[6]
Sources
- Kosaka K, ed. (2017). Dementia with Lewy bodies: clinical and biological aspects (1st ed.). Japan: Springer. doi:10.1007/978-4-431-55948-1. ISBN 978-4-431-55948-1.
References
- McKeith IG, Boeve BF, Dickson DW, et al. (July 2017). "Diagnosis and management of dementia with Lewy bodies: Fourth consensus report of the DLB Consortium". Neurology (Review). 89 (1): 88–100. doi:10.1212/WNL.0000000000004058. PMC 5496518. PMID 28592453.
- Levin J, Kurz A, Arzberger T, Giese A, Höglinger GU (February 2016). "The differential diagnosis and treatment of atypical parkinsonism". Dtsch Arztebl Int (Review). 113 (5): 61–69. doi:10.3238/arztebl.2016.0061. PMC 4782269. PMID 26900156.
- "Dementia with Lewy bodies information page". National Institute of Neurological Disorders and Stroke. May 25, 2017. Retrieved April 7, 2018.
- Gomperts SN (April 2016). "Lewy body dementias: Dementia with Lewy bodies and Parkinson disease dementia". Continuum (Minneap Minn) (Review). 22 (2 Dementia): 435–63. doi:10.1212/CON.0000000000000309. PMC 5390937. PMID 27042903.
- "Diagnosing Lewy body dementia". National Institute on Aging. US National Institutes of Health. May 17, 2017. Retrieved April 6, 2018.
- St Louis EK, Boeve AR, Boeve BF (May 2017). "REM sleep behavior disorder in Parkinson's disease and other synucleinopathies". Mov Disord (Review). 32 (5): 645–58. doi:10.1002/mds.27018. PMID 28513079.
- Weil RS, Lashley TL, Bras J, Schrag AE, Schott JM (2017). "Current concepts and controversies in the pathogenesis of Parkinson's disease dementia and dementia with Lewy bodies". F1000Res (Review). 6: 1604. doi:10.12688/f1000research.11725.1. PMC 5580419. PMID 28928962.
- St Louis EK, Boeve BF (November 2017). "REM sleep behavior disorder: Diagnosis, clinical implications, and future directions". Mayo Clin Proc (Review). 92 (11): 1723–36. doi:10.1016/j.mayocp.2017.09.007. PMC 6095693. PMID 29101940.
- Tousi B (October 2017). "Diagnosis and management of cognitive and behavioral changes in dementia with Lewy bodies". Curr Treat Options Neurol (Review). 19 (11): 42. doi:10.1007/s11940-017-0478-x. PMID 28990131.
- Palma JA, Kaufmann H (March 2018). "Treatment of autonomic dysfunction in Parkinson disease and other synucleinopathies". Mov Disord (Review). 33 (3): 372–90. doi:10.1002/mds.27344. PMC 5844369. PMID 29508455.
- Walker Z, Possin KL, Boeve BF, Aarsland D (October 2015). "Lewy body dementias". Lancet (Review). 386 (10004): 1683–97. doi:10.1016/S0140-6736(15)00462-6. PMC 5792067. PMID 26595642.
- Velayudhan L, Ffytche D, Ballard C, Aarsland D (September 2017). "New therapeutic strategies for Lewy body dementias". Curr Neurol Neurosci Rep (Review). 17 (9): 68. doi:10.1007/s11910-017-0778-2. PMID 28741230.
- "Lewy body dementia: Hope through research". National Institute of Neurological Disorders and Stroke. US National Institutes of Health. December 8, 2017. Retrieved April 6, 2018.
- Mueller C, Ballard C, Corbett A, Aarsland D (May 2017). "The prognosis of dementia with Lewy bodies". Lancet Neurol (Review). 16 (5): 390–98. doi:10.1016/S1474-4422(17)30074-1. PMID 28342649.
- Boot BP, McDade EM, McGinnis SM, Boeve BF (December 2013). "Treatment of dementia with Lewy bodies". Curr Treat Options Neurol (Review). 15 (6): 738–64. doi:10.1007/s11940-013-0261-6. PMC 3913181. PMID 24222315.
- Boot BP (2015). "Comprehensive treatment of dementia with Lewy bodies". Alzheimers Res Ther (Review). 7 (1): 45. doi:10.1186/s13195-015-0128-z. PMC 4448151. PMID 26029267.
- Kosaka K, ed. (2017), p. v.
- "What is Lewy body dementia?". National Institute on Aging. US National Institutes of Health. May 17, 2017. Retrieved April 7, 2018.
- Goedert M, Jakes R, Spillantini MG (2017). "The synucleinopathies: Twenty years on". J Parkinsons Dis (Review). 7 (s1): S53–S71. doi:10.3233/JPD-179005. PMC 5345650. PMID 28282814.
- Orimo S, Chapter 9 in Kosaka K, ed. (2017), pp. 111–12.
- Donaghy PC, O'Brien JT, Thomas AJ (January 2015). "Prodromal dementia with Lewy bodies" (PDF). Psychol Med (Review). 45 (2): 259–68. doi:10.1017/S0033291714000816. PMID 25066469.
- Karantzoulis S, Galvin JE (November 2011). "Distinguishing Alzheimer's disease from other major forms of dementia". Expert Rev Neurother (Review). 11 (11): 1579–91. doi:10.1586/ern.11.155. PMC 3225285. PMID 22014137.
- Arnaldi D, Antelmi E, St Louis EK, Postuma RB, Arnulf I (December 2017). "Idiopathic REM sleep behavior disorder and neurodegenerative risk: To tell or not to tell to the patient? How to minimize the risk?". Sleep Med Rev (Review). 36: 82–95. doi:10.1016/j.smrv.2016.11.002. PMID 28082168.
- Pezzoli S, Cagnin A, Bandmann O, Venneri A (July 2017). "Structural and functional neuroimaging of visual hallucinations in Lewy body disease: A systematic literature review". Brain Sci (Review). 7 (7): 84. doi:10.3390/brainsci7070084. PMC 5532597. PMID 28714891.
- Burghaus L, Eggers C, Timmermann L, Fink GR, Diederich NJ (February 2012). "Hallucinations in neurodegenerative diseases". CNS Neurosci Ther (Review). 18 (2): 149–59. doi:10.1111/j.1755-5949.2011.00247.x. PMC 6493408. PMID 21592320.
- Yamada M et al, Chapter 12 in Kosaka K, ed. (2017), p. 157.
- Zweig YR, Galvin JE (2014). "Lewy body dementia: the impact on patients and caregivers". Alzheimers Res Ther (Review). 6 (2): 21. doi:10.1186/alzrt251. PMC 4054937. PMID 25031635.
- Gomperts SN (April 2016). "Lewy body dementias: Dementia with Lewy bodies and Parkinson disease dementia (Table 4-6)". Continuum (Minneap Minn) (Review). 22 (2 Dementia): 11. doi:10.1212/CON.0000000000000309. PMC 5390937. PMID 27042903.
- Orimo S, Chapter 9 in Kosaka K, ed. (2017), p. 113.
- Siderowf A, Aarsland D, Mollenhauer B, Goldman JG, Ravina B (April 2018). "Biomarkers for cognitive impairment in Lewy body disorders: Status and relevance for clinical trials". Mov Disord (Review). 33 (4): 528–36. doi:10.1002/mds.27355. PMID 29624752.
- Villemagne VL, Doré V, Burnham SC, Masters CL, Rowe CC (April 2018). "Imaging tau and amyloid-β proteinopathies in Alzheimer disease and other conditions". Nat Rev Neurol (Review). 14 (4): 225–36. doi:10.1038/nrneurol.2018.9. PMID 29449700.
- McKeith IG, Dickson DW, Lowe J, et al. (December 2005). "Diagnosis and management of dementia with Lewy bodies: Third report of the DLB Consortium". Neurology (Review). 65 (12): 1863–72. doi:10.1212/01.wnl.0000187889.17253.b1. PMID 16237129.
- "Diagnosing dementia". National Institute on Aging. US National Institutes of Health. May 17, 2017. Retrieved April 6, 2018.
- Haider A, Dulebohn SC (2018). "Dementia, Lewy Body". StatPearls Publishing. PMID 29494048.
- Mori E, Chapter 6 in Kosaka K, ed. (2017), p. 73.
- Mori E, Chapter 6 in Kosaka K, ed. (2017), p. 74.
- Mori E, Chapter 6 in Kosaka K, ed. (2017), pp. 75–76.
- Yamada M et al, Chapter 12 in Kosaka K, ed. (2017), p. 162.
- Chung EJ, Kim SJ (May 2015). "(123)I-Metaiodobenzylguanidine Myocardial Scintigraphy in Lewy Body-Related Disorders: A Literature Review". J Mov Disord (Review). 8 (2): 55–66. doi:10.14802/jmd.15015. PMC 4460541. PMID 26090077.
- "Caregiving briefs: Genetics" (PDF). Lewy Body Dementia Association. 2015. Retrieved April 20, 2018.
- Orimo S, Chapter 9 in Kosaka K, ed. (2017), p. 112.
- Finger EC (April 2016). "Frontotemporal dementias". Continuum (Minneap Minn) (Review). 22 (2 Dementia): 464–89. doi:10.1212/CON.0000000000000300. PMC 5390934. PMID 27042904.
- "Vascular contributions to cognitive impairment and dementia". National Institute of Aging. US National Institutes of Health. December 31, 2017. Retrieved April 12, 2018.
- Kosaka K, Chapter 1 in Kosaka K, ed. (2017), p. 7.
- Neef D, Walling AD (2006). "Dementia with Lewy bodies: an emerging disease". Am Fam Physician (Review). 73 (7): 1223–29. PMID 16623209. Archived from the original on June 6, 2011.
- Connors MH, Quinto L, McKeith I, et al. (November 2017). "Non-pharmacological interventions for Lewy body dementia: a systematic review". Psychol Med (Review). 48 (11): 1749–58. doi:10.1017/S0033291717003257. PMC 6088773. PMID 29143692.
- Vann Jones SA, O'Brien JT (March 2014). "The prevalence and incidence of dementia with Lewy bodies: a systematic review of population and clinical studies". Psychol Med (Review). 44 (4): 673–83. doi:10.1017/S0033291713000494. PMID 23521899.
- Cheng ST (August 2017). "Dementia caregiver burden: a research update and critical analysis". Curr Psychiatry Rep (Review). 19 (9): 64. doi:10.1007/s11920-017-0818-2. PMC 5550537. PMID 28795386.
- "Caregiving brief: Behavioral symptoms" (PDF). Lewy Body Dementia Association. 2015. Retrieved April 20, 2018.
- "Caregiving brief: Medications in Lewy body dementia" (PDF). Lewy Body Dementia Association. 2015. Retrieved April 20, 2018.
- "Early stage LBD caregiving". Lewy Body Dementia Association. Retrieved April 20, 2018.
- Asada T, Chapter 2 in Kosaka K, ed. (2017), p. 11.
- Asada T, Chapter 2 in Kosaka K, ed. (2017), p. 12.
- Hogan DB, Fiest KM, Roberts JI, et al. (April 2016). "The prevalence and incidence of dementia with Lewy bodies: a systematic review". Can J Neurol Sci (Review). 43 Suppl 1: S83–95. doi:10.1017/cjn.2016.2. PMID 27307129.
- Asada T, Chapter 2 in Kosaka K, ed. (2017), p. 17.
- Asada T, Chapter 2 in Kosaka K, ed. (2017), p. 16.
- Kosaka K (2014). "Lewy body disease and dementia with Lewy bodies". Proc Jpn Acad Ser B Phys Biol Sci (Historical Review). 90 (8): 301–6. doi:10.2183/pjab.90.301. PMC 4275567. PMID 25311140.
- Engelhardt E (October 2017). "Lafora and Trétiakoff: the naming of the inclusion bodies discovered by Lewy". Arq Neuropsiquiatr (Historical article). 75 (10): 751–53. doi:10.1590/0004-282X20170116. PMID 29166468.
- Lewy F (1912). Paralysis agitans. I. Pathologische Anatomie In Handbuch der Neurologie, Vol 3, Lewandowsky M, Abelsdorff G, eds. Springer Verlag, Berlin, pp. 920–33. as cited in Goedert M, Jakes R, Spillantini MG (2017). "The synucleinopathies: Twenty years on". J Parkinsons Dis (Review). 7 (s1): S53–S71. doi:10.3233/JPD-179005. PMC 5345650. PMID 28282814.
- Engelhardt E, Gomes M (2017). "Lewy and his inclusion bodies: Discovery and rejection". Dement Neuropsychol. 11 (2): 198–201. doi:10.1590/1980-57642016dn11-020012. PMC 5710688. PMID 29213511.
- Kosaka K, Chapter 1 in Kosaka K, ed. (2017), p. 4.
- Kosaka K, Oyanagi S, Matsushita M, Hori A (1976). "Presenile dementia with Alzheimer-, Pick- and Lewy-body changes". Acta Neuropathol. 36 (3): 221–33. doi:10.1007/bf00685366. PMID 188300.
- McKeith IG, Chapter 5 in Kosaka K, ed. (2017), p. 60.
- McKeith IG, Chapter 5 in Kosaka K, ed. (2017), pp. 60–61.
- McKeith IG, Chapter 5 in Kosaka K, ed. (2017), p. 63.
- McKeith IG (2006). "Consensus guidelines for the clinical and pathologic diagnosis of dementia with Lewy bodies (DLB): report of the Consortium on DLB International Workshop". J Alzheimers Dis. 9 (3 Suppl): 417–23. doi:10.3233/JAD-2006-9S347. PMID 16914880.
- Goedert M, Spillantini MG, Del Tredici K, Braak H (January 2013). "100 years of Lewy pathology". Nat Rev Neurol (Practice guideline). 9 (1): 13–24. doi:10.1038/nrneurol.2012.242. PMID 23183883.
- McKeith IG, Chapter 5 in Kosaka K, ed. (2017), pp. 64–67.
- Gallman S (November 4, 2015). "Robin Williams' widow speaks: Depression didn't kill my husband". CNN. Archived from the original on April 11, 2015. Retrieved April 6, 2018.
- Williams SS (September 2016). "The terrorist inside my husband's brain". Neurology. 87 (13): 1308–11. doi:10.1212/WNL.0000000000003162. PMID 27672165.
- Robbins R (September 30, 2016). "How Lewy body dementia gripped Robin Williams". Scientific American. Retrieved April 9, 2018.
- Sahlas DJ (June 2003). "Dementia with Lewy bodies and the neurobehavioral decline of Mervyn Peake". Arch Neurol (Historical article). 60 (6): 889–92. doi:10.1001/archneur.60.6.889. PMID 12810496.
- "LBDA Clarifies Autopsy Report on Comedian, Robin Williams". Lewy Body Dementia Association. November 10, 2014. Retrieved April 19, 2018.
- McKeith IG. "Robin Williams had dementia with Lewy bodies -- so, what is it and why has it been eclipsed by Alzheimer's?". The Conversation. Archived from the original on April 11, 2016. Retrieved April 6, 2018.
- Ikeda M, Chapter 16 in Kosaka K, ed. (2017), p. 215.
External links
- Adams BD (January 16, 2013). "Lewy Body Dementia in the Emergency Department". Postgraduate Medical Journal. Retrieved April 18, 2018.
- McKeith I (October 10, 2017). Updated diagnostic criteria and management of Lewy body dementia (Video). ALZForum co-hosted with Lewy Body Dementia Association. Retrieved April 8, 2018.
- "Emergency room treatment of psychosis" (PDF). Lewy Body Dementia Association. Retrieved 27 April 2018.
| Classification | |
|---|---|
| External resources |