Capnography
Capnography is the monitoring of the concentration or partial pressure of carbon dioxide (CO
2) in the respiratory gases. Its main development has been as a monitoring tool for use during anesthesia and intensive care. It is usually presented as a graph of expiratory CO
2 (measured in millimeters of mercury, "mmHg") plotted against time, or, less commonly, but more usefully, expired volume. The plot may also show the inspired CO
2, which is of interest when rebreathing systems are being used. When the measurement is taken at the end of a breath (exhaling), it is called "end tidal" CO
2 (ETCO2).
| Capnography | |
|---|---|
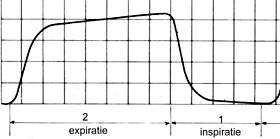 Typical capnogram. Expiration phase on the left, inspiration on the right. | |
| Other names | End tidal CO2 (ETCO2) |
| MeSH | D019296 |
The capnogram is a direct monitor of the inhaled and exhaled concentration or partial pressure of CO
2, and an indirect monitor of the CO
2 partial pressure in the arterial blood. In healthy individuals, the difference between arterial blood and expired gas CO
2 partial pressures is very small. In the presence of most forms of lung disease, and some forms of congenital heart disease (the cyanotic lesions) the difference between arterial blood and expired gas increases and can exceed 1 kPa.
Medical use
Anaesthesia

During anesthesia, there is interplay between two components: the patient and the anesthesia administration device (which is usually a breathing circuit and a ventilator). The critical connection between the two components is either an endotracheal tube or a mask, and CO
2 is typically monitored at this junction. Capnography directly reflects the elimination of CO
2 by the lungs to the anesthesia device. Indirectly, it reflects the production of CO
2 by tissues and the circulatory transport of CO
2 to the lungs.
When expired CO
2 is related to expired volume rather than time, the area beneath the curve represents the volume of CO
2 in the breath, and thus over the course of a minute, this method can yield the CO
2 per minute elimination, an important measure of metabolism. Sudden changes in CO
2 elimination during lung or heart surgery usually imply important changes in cardiorespiratory function.
Capnography has been shown to be more effective than clinical judgement alone in the early detection of adverse respiratory events such as hypoventilation, oesophageal intubation and circuit disconnection; thus allowing patient injury to be prevented. During procedures done under sedation, capnography provides more useful information, e.g. on the frequency and regularity of ventilation, than pulse oximetry.
Capnography provides a rapid and reliable method to detect life-threatening conditions (malposition of tracheal tubes, unsuspected ventilatory failure, circulatory failure and defective breathing circuits) and to circumvent potentially irreversible patient injury.
Capnography and pulse oximetry together could have helped in the prevention of 93% of avoidable anesthesia mishaps according to an ASA (American Society of Anesthesiologists) closed claim study.
Emergency medical services
Capnography is increasingly being used by EMS personnel to aid in their assessment and treatment of patients in the prehospital environment. These uses include verifying and monitoring the position of an endotracheal tube or a blind insertion airway device. A properly positioned tube in the trachea guards the patient's airway and enables the paramedic to breathe for the patient. A misplaced tube in the esophagus will lead to the patient's death if it goes undetected.
A study in the March 2005 Annals of Emergency Medicine, comparing field intubations that used continuous capnography to confirm intubations versus non-use showed zero unrecognized misplaced intubations in the monitoring group versus 23% misplaced tubes in the unmonitored group. The American Heart Association (AHA) affirmed the importance of using capnography to verify tube placement in their 2005 CPR and Emergency Cardiovascular Care Guidelines.
The AHA also notes in their new guidelines that capnography, which indirectly measures cardiac output, can also be used to monitor the effectiveness of CPR and as an early indication of return of spontaneous circulation (ROSC). Studies have shown that when a person doing CPR tires, the patient's end-tidal CO
2 (ETCO2, the level of carbon dioxide released at the end of expiration) falls, and then rises when a fresh rescuer takes over. Other studies have shown when a patient experiences return of spontaneous circulation, the first indication is often a sudden rise in the ETCO2 as the rush of circulation washes untransported CO
2 from the tissues. Likewise, a sudden drop in ETCO2 may indicate the patient has lost pulses and CPR may need to be initiated.
Paramedics are also now beginning to monitor the ETCO2 status of nonintubated patients by using a special nasal cannula that collects the carbon dioxide. A high ETCO2 reading in a patient with altered mental status or severe difficulty breathing may indicate hypoventilation and a possible need for the patient to be intubated. Low ETCO2 readings on patients may indicate hyperventilation.
Capnography, because it provides a breath by breath measurement of a patient's ventilation, can quickly reveal a worsening trend in a patient's condition by providing paramedics with an early warning system into a patient's respiratory status. Clinical studies are expected into the uses of capnography in asthma, congestive heart failure, diabetes, circulatory shock, pulmonary embolus, acidosis, and other conditions, with potential implications for the prehospital use of capnography.
Registered nurses
Registered nurses in critical care settings may use capnography to determine if a nasogastric tube, which is used for feeding, has been placed in the trachea as opposed to the esophagus.[1] Usually a patient will cough or gag if the tube is misplaced, but most patients in critical care settings are sedated or comatose. If a nasogastric tube is accidentally placed in the trachea instead of the esophagus, the tube feedings will go into the lungs, which is a life-threatening situation.
Working mechanism
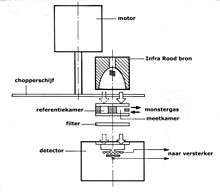
Capnographs usually work on the principle that CO
2 absorbs infrared radiation. A beam of infrared light is passed across the gas sample to fall on a sensor. The presence of CO
2 in the gas leads to a reduction in the amount of light falling on the sensor, which changes the voltage in a circuit. The analysis is rapid and accurate, but the presence of nitrous oxide in the gas mix changes the infrared absorption via the phenomenon of collision broadening.[2] This must be corrected for measuring the CO
2 in human breath by measuring its infrared absorptive power. This was established as a reliable technique by John Tyndall in 1864, though 19th and early 20th century devices were too cumbersome for everyday clinical use.[3]
Diagnostic usage
Capnography provides information about CO
2 production, pulmonary (lung) perfusion, alveolar ventilation, respiratory patterns, and elimination of CO
2 from the anesthesia breathing circuit and ventilator. The shape of the curve is affected by some forms of lung disease; in general there are obstructive conditions such as bronchitis, emphysema and asthma, in which the mixing of gases within the lung is affected.
Conditions such as pulmonary embolism and congenital heart disease, which affect perfusion of the lung, do not, in themselves, affect the shape of the curve, but greatly affect the relationship between expired CO
2 and arterial blood CO
2. Capnography can also be used to measure carbon dioxide production, a measure of metabolism. Increased CO
2 production is seen during fever and shivering. Reduced production is seen during anesthesia and hypothermia.
Capnogram model
The capnogram waveform provides information about various respiratory and cardiac parameters. The capnogram double-exponential model attempts to quantitatively explain the relationship between respiratory parameters and the exhalatory segment of a capnogram waveform[4]. According to the model, each exhalatory segment of capnogram waveform follows the analytical expression:

where
- represents the partial pressure of carbon dioxide measured by the capnogram as a function of time since the beginning of exhalation.
- represents the alveolar partial pressure of carbon dioxide.
- represents the inverse of the dead space fraction (i.e. the ratio of tidal volume to dead space volume).
- represents the pulmonary time constant (i.e. the product of pulmonary resistance and compliance)





In particular, this model explains the rounded "shark-fin" shape of the capnogram observed in patients with obstructive lung disease.
References
- Potter, Patricia Ann, and Anne Griffin Perry. "Nutrition." Essentials for nursing practice. Eighth ed. St. Louis: Elsevier, 2015. 940. Print.
- Raemer DB, Calalang I (April 1991). "Accuracy of end-tidal carbon dioxide tension analyzers". J Clin Monit. 7 (2): 195–208. doi:10.1007/BF01618124. PMID 1906531.
- Jaffe MB (September 2008). "Infrared measurement of carbon dioxide in the human breath: "breathe-through" devices from Tyndall to the present day". Anesth. Analg. 107 (3): 890–904. doi:10.1213/ane.0b013e31817ee3b3. PMID 18713902.
- Abid, Abubakar (May 2017). "Model-Based Estimation of Respiratory Parameters from Capnography, With Application to Diagnosing Obstructive Lung Disease". IEEE Transactions on Biomedical Engineering. 64 (12): 2957–2967. doi:10.1109/TBME.2017.2699972. PMID 28475040.
Bibliography
- Silvestri S, Ralls GA, Krauss B, et al. (May 2005). "The effectiveness of out-of-hospital use of continuous end-tidal carbon dioxide monitoring on the rate of unrecognized misplaced intubation within a regional emergency medical services system". Ann Emerg Med. 45 (5): 497–503. doi:10.1016/j.annemergmed.2004.09.014. PMID 15855946.
- Lightdale JR, Goldmann DA, Feldman HA, Newburg AR, DiNardo JA, Fox VL (June 2006). "Microstream capnography improves patient monitoring during moderate sedation: a randomized, controlled trial". Pediatrics. 117 (6): e1170–8. doi:10.1542/peds.2005-1709. PMID 16702250.
- Burton JH, Harrah JD, Germann CA, Dillon DC (May 2006). "Does end-tidal carbon dioxide monitoring detect respiratory events prior to current sedation monitoring practices?". Acad Emerg Med. 13 (5): 500–4. doi:10.1197/j.aem.2005.12.017. PMID 16569750.
External links
- Physical principles used in capnography graphically explained
- Capnography.com
- Capnography for Paramedics
- CapnoBase.org: Respiratory signal database that contains clinical and simulated capnogram recordings
- Research project on capnography
| Types |
|
|---|---|
| Techniques | |
| Scientific principles |
|
| Measurements | |
| Instruments | |
| Complications | |
| Subspecialties |
|
| Professions |
|
| History |
|
| Organizations |
|
| |