Testicular torsion
Testicular torsion occurs when the spermatic cord (from which the testicle is suspended) twists, cutting off the blood supply to the testicle.[3] The most common symptom in children is sudden, severe testicular pain.[1] The testicle may be higher than usual in the scrotum and vomiting may occur.[1][2] In newborns pain is often absent and instead the scrotum may become discolored or the testicle may disappear from its usual place.[1]
| Testicular torsion | |
|---|---|
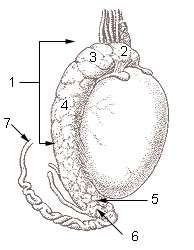 | |
| 1. Epididymis 2. Head of epididymis 3. Lobules of epididymis 4. Body of epididymis 5. Tail of epididymis 6. Duct of epididymis 7. Deferent duct (ductus deferens or vas deferens) | |
| Specialty | Urology |
| Symptoms | Severe testicular pain, elevated testicle[1] |
| Complications | Infertility[2] |
| Usual onset | Sudden[1] |
| Types | Intravaginal torsion, extravaginal torsion[1] |
| Risk factors | "Bell clapper deformity", testicular tumor, cold temperature[1] |
| Diagnostic method | Based on symptoms[1] |
| Differential diagnosis | Epididymitis, inguinal hernia, torsion of the appendix testicle[2] |
| Treatment | Physically untwisting the testicle, surgery[1] |
| Prognosis | Generally good with rapid treatment[1] |
| Frequency | ~1 in 15,000 per year (under 25 years old)[2][3] |
Most of those affected have no obvious prior underlying health problems.[1] Testicular tumor or prior trauma may increase risk.[1][3] Other risk factors include a congenital malformation known as a "bell-clapper deformity" wherein the testis is inadequately attached to the scrotum allowing it to move more freely and thus potentially twist.[1] Cold temperatures may also be a risk factor.[1] The diagnosis should usually be made based on the presenting symptoms.[1][2] An ultrasound can be useful when the diagnosis is unclear.[2]
Treatment is by physically untwisting the testicle, if possible, followed by surgery.[1] Pain can be treated with opioids.[1] Outcome depends on time to correction.[1] If successfully treated within six hours onset, it is often good, however, if delayed for 12 or more hours the testicle is typically not salvageable.[1] About 40% of people require removal of the testicle.[2]
It is most common just after birth and during puberty.[2] It occurs in about 1 in 4,000 to 1 in 25,000 males under 25 years of age each year.[2][3] Of children with testicular pain of rapid onset, testicular torsion is the cause of about 10% of cases.[2] Complications may include an inability to have children.[2] The condition was first described in 1840 by Louis Delasiauve.[4]
Signs and symptoms
Testicular torsion usually presents with severe testicular pain or pain in the groin and lower abdomen.[2] Pain generally begins suddenly and typically involves only one side.[5] There is often associated nausea and vomiting.[2] The testicle may lie higher in the scrotum due to twisting and subsequent shortening of the spermatic cord[5] or may be positioned in a horizontal orientation. Mild warmth and redness of the overlying area may be present. Elevation of the testicle may worsen the pain. The cremasteric reflex, which normally causes elevation of the testicle by stroking the inner thigh, may be absent,[1] especially in children.[5] Urinary symptoms, such as pain or increased frequency of urination are also typically absent.[6] Symptom onset often follows physical activity or trauma to the testes or scrotum. Children with testicular torsion may awaken with testicular or abdominal pain in the middle of the night or in the morning.[7] There may be a history of previous, similar episodes of scrotal pain due to prior transient testicular torsion with spontaneous resolution.[5]
Complications
- Testicular infarction: Testicular damage occurs as a consequence of decreased blood flow, and therefore decreased oxygen and nutrient supply, to the testicle. If the testicle is not viable during surgical exploration, it must be removed to prevent further necrosis, or tissue death.
- Infertility:[8] The impact of testicular torsion on long-term fertility is not yet fully understood.[9] However, testicular torsion may cause abnormal sperm function on semen analysis, although these abnormalities are more likely to be found in adolescents and in adults. Torsion does not seem to affect long-term sperm function in neonates.[10] The cause of abnormal sperm function is thought to be due to the following mechanisms:
- Immunological theory, also known as "sympathetic orchidopathia": It is thought that following injury to the testicle, the body's immune system is activated to clean up damaged cells. In the process, it creates anti-testicular cell antibodies, or proteins that cross the injured blood-testis barrier and damage both the affected and contralateral testicles.[10]
- Abnormalities in microcirculation within the testicle [10][11]
- Reperfusion injury: This type of injury is seen in tissues that have been deprived of blood supply for a prolonged period.[10]
- Gangrene, or a type of tissue damage caused by lack of blood supply, of the testis.
- Recurrence of torsion may occur even after surgical fixation, although this is very unlikely.[12][13]
- Psychological impact of losing a testicle.[14]
Risk factors
Most of those affected with testicular torsion have no prior underlying health problems or predisposing conditions.[1] However, there are certain factors that may increase risk of testicular torsion. A larger testicle either due to normal variation or testicular tumor increases the risk of torsion.[3] Similarly, the presence of a mass or malignancy involving the spermatic cord can also predispose to torsion.[1]
Age is also an important risk factor for torsion. Torsion most commonly occurs either in the newborn or just before or during puberty.[2] Testicular torsion often occurs before or during puberty, prior to complete testicular descent. Epididymitis is more commonly a postpubertal condition.[7]
Several congenital anatomic malformations or variations in the testicle or the surrounding structures may allow for increased scrotal rotation and increase the risk of testicular torsion.[3] A congenital malformation of the processus vaginalis known as "bell-clapper deformity" accounts for 90% of all cases.[3][15] In this condition, rather than the testes attaching posteriorly to the inner lining of the scrotum by the mesorchium, the mesorchium terminates early and the testis is free floating in the tunica vaginalis. Other anatomic risk factors include horizontal lie of the testicle or a spermatic cord with a long intrascrotal portion.[3]
Cryptorchidisim is also a risk factor for torsion[3] with some studies proposing a 10-fold higher risk.[16]
Testicular torsion may also be caused by trauma to the scrotum or exercise (in particular, bicycle riding),[9] however only about 4-8% of cases are the result of trauma.[1][2]
There is thought to be a possible genetic basis for predisposition to torsion, based on multiple published reports of familial testicular torsion.[9] There is controversy whether cold weather months are associated with an increased risk.[9]
Pathophysiology
Testicular torsion occurs when there is mechanical twisting of the spermatic cord, which suspends the testicle within the scrotum and contains the testicular artery and vein. Twisting of the cord reduces or eliminates blood flow to the testicle.[3] The degree of arterial and venous obstruction depends on the duration and severity of the torsion event. Typically, venous blood flow is compromised first.[1] The increase in venous pressure subsequently causes decreased arterial blood flow, leading to decreased oxygen supply to the testicle, and if untreated, testicular infarction.[2]
It is also believed that torsion occurring during fetal development can lead to so-called neonatal torsion or vanishing testis, and is one of the causes of an infant being born with monorchism (one testicle).[17]
Intermittent testicular torsion
Intermittent testicular torsion (ITT) is a less serious but chronic variant of torsion. It is characterized by intermittent scrotal or testicular pain, followed by eventual spontaneous detorsion and resolution of pain. Nausea and vomiting may also occur.[6]:p.150 Though less pressing, such individuals are at significant risk of complete torsion and possible subsequent orchiectomy and the recommended treatment is elective bilateral orchiopexy. Ninety-seven percent of patients who undergo such surgery experience complete relief from their symptoms.[18]:p.316
Extravaginal testicular torsion
Torsion occurring outside of the tunica vaginalis, when the testis and gubernaculum can rotate freely, is termed an extravaginal testicular torsion. This type occurs exclusively in newborns, however, newborns can be affected by other testicular torsion variants as well.[2] Neonates experiencing such a torsion typically present with painless scrotal swelling,[2] discoloration, and a firm, painless mass in the scrotum. Such testes are usually necrotic from birth and must be removed surgically.[18]:p.315 The exact cause of or specific risk factors for extravaginal torsion in this population remain unclear.[2]
Intravaginal testicular torsion
Intravaginal testicular torsion occurs when the testicle rotates on the spermatic cord within the tunica vaginalis.[2] This variant more commonly occurs in older children and adults. The "bell-clapper deformity," in which there is inappropriately high attachment of the tunica vaginalis over the spermatic cord and failure of the normal posterior attachment of the testicle to the inner scrotum, which allows the testicle to move freely within the tunica vaginalis and predisposes to intravaginal testicular torsion.[2]
Torsion of the testicular appendix
The testicular appendix is located in the upper pole of the testicle. It is an embryonic remnant that has no known function, but is at risk for torsion events.[18] This type of torsion is the most common cause of acute scrotal pain in boys ages 7–14. Its appearance is similar to that of testicular torsion but the onset of pain is typically more gradual. Palpation reveals a small firm nodule on the upper portion of the testis which displays a characteristic "blue dot sign". This is the appendix of the testis which has become discolored and is noticeably blue through the skin. Unlike other torsions, however, the cremasteric reflex is still active. Typical treatment involves the use of over-the-counter analgesics and the condition resolves within 2–3 days.[18]:p.316
Torsion of the undescended testicle
The undescended testis is at increased risk of testicular torsion.[16] The mechanism for torsion in the undescended testicle is not fully understood, though it may be due to abnormal contractions of the cremaster muscle, which covers the testicle and spermatic cord and is responsible for raising and lowering the testicle to regulate scrotal temperature. The undescended testicle is also at higher risk for testicular tumor, which due to the increased weight and size compared to a healthy testicle can predispose to torsion.[16]
Diagnosis
The diagnosis should generally be made based on the presenting symptoms.[1][2] An ultrasound can be useful when the diagnosis is unclear.[2] However, imaging should not delay surgical intervention as complications develop with prolonged ischemia.[2] Immediate surgery is recommended regardless of imaging findings if there is a high degree of suspicion based on history and physical examination.[1][2]
Given the treatment implications of testicular torsion, it is important to distinguish testicular torsion from other causes of testicular pain, such as epididymitis, which can present similarly. While both conditions can cause testicular pain, the pain of epididymitis is typically localized to the epididymis at the rear pole of the testicle. Epididymitis may also be characterized by discoloration and swelling of the testis, and fever. The cremasteric reflex in epididymitis is usually present. Testicular torsion, or more probably impending testicular infarction, can also produce a low-grade fever.[18] There is often an absent or decreased cremasteric reflex.[2]
Clinical exam
The absence of the cremasteric reflex in an acutely painful testicle is most indicative of testicular torsion (the twisting of the spermatic cord of the testicle makes reflexive responses all but impossible). On physical examination, the testis can be swollen, tender, high-riding, and with an abnormal transverse lie.[19] Prehn's sign, a classic physical exam finding, has not been reliable in distinguishing torsion from other causes of testicular pain such as epididymitis.[20] The individual will not usually have a fever, though nausea is common.
Imaging
A doppler ultrasound scan of the scrotum can identify the absence of blood flow in the twisted testicle and is nearly 90% accurate in diagnosis.[2][3] It can also help distinguish torsion from epididymitis.[21]
Radionuclide scanning (scintigraphy) of the scrotum is the most accurate imaging technique, but it is not routinely available, particularly with the urgency that might be required.[22] The agent of choice for this purpose is technetium-99m pertechnetate.[23] Initially it provides a radionuclide angiogram, followed by a static image after the radionuclide has perfused the tissue. In the healthy patient, initial images show symmetric flow to the testes, and delayed images show uniformly symmetric activity.[23] In testicular torsion, the images may show heterogenous activity within the affected testicle.[23]
Treatment
Testicular torsion is a surgical emergency that requires immediate intervention to restore the flow of blood to the testicle.[3] If treated either manually or surgically within six hours, there is a high chance (approximately 90%) of saving the testicle. At 12 hours the rate decreases to 50%; at 24 hours it drops to 10%, and after 24 hours the ability to save the testicle approaches 0, although salvage of the testicle has been reported beyond 24 hours.[3][24] About 40% of cases result in loss of the testicle.[2]
With prompt diagnosis and treatment the testicle can often be saved.[3] Typically, when a torsion takes place, the surface of the testicle has rotated towards the midline of the body. Non-surgical correction can sometimes be accomplished by manually rotating the testicle in the opposite direction (i.e., outward, towards the thigh); if this is initially unsuccessful, a forced manual rotation in the other direction may correct the problem.[6]:p.149 The success rate of manual detorsion is not known with confidence.
When salvage of the testicle is accomplished, long-term testicular damage is common. Testicular size is often diminished, and injury to the unaffected testicle is common.[9] The effect of a torsion event on long-term fertility is not fully understood.[9]
A repeat doppler ultrasound scan may confirm restoration of blood flow to the testicle following manual detorsion. However, surgical exploration is often performed in order to assess the health and viability of the testicle. An orchiopexy is performed to both the affected and unaffected testicles in order to prevent recurrence. If the testis is not viable, it is removed (orchiectomy).[25]
Epidemiology
Torsion is most frequent among adolescents with about 65% of cases presenting between 12–18 years of age.[26] It is the most common cause of rapid onset testicular pain and swelling in people under 18 years old.[26] It occurs in about 1 in 4,000 to 1 per 25,000 males per year before 25 years of age;[2][3][15] but it can occur at any age, including infancy.[6]:p.149
See also
- Ovarian torsion – equivalent condition of the female reproductive system.
- Epididymitis – can cause of testicular pain and present similarly to testicular torsion.
References
- Ludvigson, AE; Beaule, LT (June 2016). "Urologic Emergencies". The Surgical Clinics of North America. 96 (3): 407–24. doi:10.1016/j.suc.2016.02.001. PMID 27261785.
- Sharp, VJ; Kieran, K; Arlen, AM (Dec 15, 2013). "Testicular torsion: diagnosis, evaluation, and management". American Family Physician. 88 (12): 835–40. PMID 24364548. Archived from the original on 2016-11-04.
- Wampler SM, Llanes M (September 2010). "Common scrotal and testicular problems". Prim. Care. 37 (3): 613–26, x. doi:10.1016/j.pop.2010.04.009. PMID 20705202.
- Schill, Wolf-Bernhard; Comhaire, Frank H.; Hargreave, Timothy B. (2006). Andrology for the Clinician. Springer Science & Business Media. p. 134. ISBN 9783540337133. Archived from the original on 2017-09-10.
- Gordhan, Chirag G (Jan 2015). "Scrotal pain: Evaluation and management". Korean Journal of Urology. 56 (1): 3–11. doi:10.4111/kju.2015.56.1.3. PMC 4294852. PMID 25598931.
- Uribe, Juan F. (1 January 2008). Potts, Jeannette M. (ed.). Genitourinary Pain and Inflammation: Diagnosis and Management. Totowa, New Jersey: Humana. pp. 149–. ISBN 978-1-60327-126-4. Retrieved 8 July 2013.
- Koester, Michael C (Jan–Mar 2000). "Initial Evaluation and Management of Acute Scrotal Pain". Journal of Athletic Training. 35 (1): 76–79. PMC 1323443. PMID 16558613.CS1 maint: date format (link)
- Abdel Raheem, Amr; Ralph, David; Minhas, S. (September 2012). "Male infertility". British Journal of Medical and Surgical Urology. 5 (5): 254–268. doi:10.1016/j.bjmsu.2012.06.003. ISSN 1875-9742.
- DaJusta, Daniel (Oct 2012). "Contemporary Review of Testicular Torsion: New Concepts, Emerging Technologies and Potential Therapeutics". Journal of Pediatric Urology. 9 (6): 723–30. doi:10.1016/j.jpurol.2012.08.012. PMC 3566290. PMID 23044376.
- Nistal, Manuel; Paniagua, Ricardo; González-Peramato, Pilar; Reyes-Múgica, Miguel (September 2016). "Perspectives in Pediatric Pathology, Chapter 19. Testicular Torsion, Testicular Appendix Torsion, and other Forms of Testicular Infarction". Pediatric and Developmental Pathology. 19 (5): 345–359. doi:10.2350/14-06-1514-pb.1. ISSN 1093-5266. PMID 25105275.
- Karaguzel, Ersagun; Kadihasanoglu, Mustafa; Kutlu, Omer (2014-06-17). "Mechanisms of testicular torsion and potential protective agents". Nature Reviews Urology. 11 (7): 391–399. doi:10.1038/nrurol.2014.135. ISSN 1759-4812. PMID 24934447.
- O’Brien, M., & Chandran, H. (2008). The acute scrotum in childhood. Surgery (Oxford), 26(7), 279-282. doi:10.1016/j.mpsur.2008.05.001
- Sells, Henry; Moretti, Kim L.; Burfield, Geoffrey D. (January 2002). "Recurrent torsion after previous testicular fixation". ANZ Journal of Surgery. 72 (1): 46–48. doi:10.1046/j.1445-2197.2002.02295.x. ISSN 1445-1433.
- Ta, Anthony; D’Arcy, Frank T.; Hoag, Nathan; D’Arcy, John P.; Lawrentschuk, Nathan (June 2016). "Testicular torsion and the acute scrotum". European Journal of Emergency Medicine. 23 (3): 160–165. doi:10.1097/mej.0000000000000303. ISSN 0969-9546. PMID 26267075.
- Ringdahl E, Teague L (November 2006). "Testicular torsion". Am Fam Physician. 74 (10): 1739–43. PMID 17137004.
- Naouar, Sahbi (Jun 2016). "Testicular torsion in undescended testis: A persistent challenge". Asian Journal of Urology. 4 (2): 111–115. doi:10.1016/j.ajur.2016.05.007. PMC 5717970. PMID 29264215.
- Callewaert PR, Kerrebroeck PV (June 2010). "New insights into perinatal testicular torsion". Eur J Pediatr. 169 (6): 705–12. doi:10.1007/s00431-009-1096-8. PMC 2859224. PMID 19856186.
- Kavoussi, Parviz K.; Costabile, Raymond A. (2011). "Disorders of scrotal contents: orchitis, epididimytis, testicular tortion, tortion of the appendages, and Fournier's gangrene". In Chapple, Christopher R.; Steers, William D. (eds.). Practical urology: essential principles and practice. London: Springer-Verlag. ISBN 978-1-84882-033-3. Archived from the original on 2014-07-05.
- Liu DR. Chapter 127. Urologic and Gynecologic Problems and Procedures in Children. In: Tintinalli JE, Stapczynski JS, Cline DM, Ma OJ, Cydulka RK, Meckler GD, eds. Tintinalli's Emergency Medicine: A Comprehensive Study Guide. 7th ed. New York: McGraw-Hill; 2011.
- Lavallee ME, Cash J (April 2005). "Testicular torsion: evaluation and management". Curr Sports Med Rep. 4 (2): 102–4. doi:10.1097/01.CSMR.0000306081.13064.a2. PMID 15763047.
- Arce J, Cortés M, Vargas J (2002). "Sonographic diagnosis of acute spermatic cord torsion. Rotation of the cord: a key to the diagnosis". Pediatr Radiol. 32 (7): 485–91. doi:10.1007/s00247-002-0701-z. PMID 12107581.
- Sexually Transmitted Diseases Treatment Guidelines, 2010 Archived 2012-04-04 at the Wayback Machine from Centers for Disease Control and Prevention, Recommendations and Reports. December 17, 2010 / Vol. 59 / No. RR-12
- Medscape > Testicular Torsion Imaging Archived 2012-06-27 at the Wayback Machine by David Paushter. Updated: May 25, 2011
- Mellick, Larry Bruce; Sinex, James E.; Gibson, Robert W.; Mears, Kim (2017-09-25). "A Systematic Review of Testicle Survival Time After a Torsion Event". Pediatric Emergency Care. Publish Ahead of Print: 1. doi:10.1097/PEC.0000000000001287. ISSN 0749-5161. PMID 28953100.
- Manjunath, Adarsh S.; Hofer, Matthias D. (2018-03-01). "Urologic Emergencies". Medical Clinics of North America. 102 (2): 373–385. doi:10.1016/j.mcna.2017.10.013. ISSN 0025-7125. PMID 29406065.
- Edelsberg JS, Surh YS (August 1988). "The acute scrotum". Emerg. Med. Clin. North Am. 6 (3): 521–46. PMID 3292226.
External links
| Classification | |
|---|---|
| External resources |
- Photos of swollen, excised, and detorsed testicles of patient who sought treatment within four hours of onset of pain.