

Ehrlichiosis
 ShareCompartir
ShareCompartir
Agents
Ehrlichia chaffeensis, Ehrlichia ewingii, Ehrlichia muris-like (EML)
 WHERE FOUND
WHERE FOUND
Ehrlichiosis is most frequently reported from the southeastern and south-central U.S., from the eastern seaboard extending westward to Texas. The areas from which cases are reported correspond with the known geographic distribution of the lone star tick (Amblyomma americanum), which is associated with transmission of both E. chaffeensis and E. ewingii. Three states (Oklahoma, Missouri, Arkansas) account for 35% of all reported E. chaffeensis infections. In 2009 a new Ehrlichia species, provisionally called Ehrlichia muris-like (EML) was identified among patients in the upper Midwest. Since that time more than 67 cases have been identified. At this time, the tick responsible for transmitting EML is unknown and clinical presentations have not been differentiated from that of other Ehrlichia species.
INCUBATION PERIOD: 1-2 weeks
SIGNS AND SYPMTOMS
- Fever
- Headache
- Chills
- Cough
- Malaise
- Muscle pain
- Gastrointestinal symptoms (nausea, vomiting, diarrhea, anorexia)
- Central nervous system involvement, including meningitis or meninigeoencephalitis may occur late in illness
- Conjunctival injection
- Rash (more commonly reported among children)
Ehrlichiosis and anaplasmosis have a similar clinical presentation, but they are transmitted by two different species of ticks and generally occur in different regions of the U.S.
The above list presents symptoms commonly seen with ehrlichiosis. However, it is important to note that few people will develop all symptoms and the number and combination of symptoms varies greatly from person to person.
 Confirmation of the diagnosis is based on laboratory testing, but antibiotic therapy should not be delayed in a patient with a suggestive clinical presentation.
Confirmation of the diagnosis is based on laboratory testing, but antibiotic therapy should not be delayed in a patient with a suggestive clinical presentation.
GENERAL LABORATORY FINDINGS
Typically Observed During the First Week of Clinical Disease:
- Anemia (may occur late in illness)
- Leukopenia (absolute)
- Mild to moderate elevations in hepatic transaminases may occur in some patients
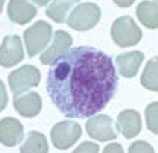
- During the acute stage of illness, morulae may be detected in about 20% of patients. E. chaffeensis most commonly infects monocytes, whereas E. ewingii more commonly infects granulocytes.
LABORATORY CONFIRMATION
Antibodies to Ehrlichia species are detectable 7-10 days after illness onset. The gold-standard serologic test looks for a four-fold change in IgG-specific antibody titers using indirect immunofluorescence assay (IFA) on paired samples. The first sample should be taken within the first week of illness and the second should be taken 2 to 4 weeks later.
- Demonstration of a four-fold change in IgG-specific antibody titer by indirect immunofluorescence assay (IFA) test in paired serum samples; or
- Detection of DNA by PCR on whole blood. This method is most sensitive within the first week of illness; may decrease in sensitivity after administration of antibiotics.
NOTE: IgM antibodies are less specific than IgG antibodies and are more likely to generate false positive results. IgM results alone should not be used for laboratory diagnosis
NOTE: Antibody titers are frequently negative in the first 7–10 days of illness, thus serologic tests may be falsely negative during this time period.
Treatment
Anaplasmosis, ehrlichiosis, and Rocky Mountain spotted fever are treated in the same manner with doxycycline.† Clinical suspicion of any of these diseases is sufficient to begin treatment. Delay in treatment may result in severe illness and death. The regimens listed below are guidelines only and may need to be adjusted depending on a patient’s age, medical history, underlying health conditions, pregnancy status, or allergies. Consult an infectious disease specialist in cases of documented pregnancy or life-threatening allergies to doxycycline.
| Age Category | Drug | Dosage | Maximum | Duration (Days) |
|---|---|---|---|---|
| Adults | Doxycycline | 100 mg twice per day, orally or IV | 100 mg/dose | Patients should be treated for at least 3 days after the fever subsides and until there is evidence of clinical improvement. Minimum course of treatment is 5-7 days. |
| Children weighing <100 lbs. (45.4 kg) | Doxycycline | 2.2 mg/kg per dose twice per day, orally or IV | 100 mg/dose |
NOTE: Use doxycycline as first-line treatment for suspected ehrlichiosis in patients of all ages. The use of doxycycline to treat suspected ehrlichiosis in children is recommended by both the CDC and the American Academy of Pediatrics Committee on Infectious Diseases. Use of antibiotics other than doxycycline increases the risk of patient death. At the recommended dose and duration needed to treat ehrlichiosis, no evidence has been shown to cause staining of permanent teeth, even when five courses are given before the age of eight.
References
†Biggs HM, Barton Behravesh C, Bradley KK, et al. Diagnosis and management of tickborne rickettsial diseases: Rocky Mountain spotted fever and other spotted fever group rickettsioses, ehrlichioses, and anaplasmosis — United States. MMWR Recomm Rep 2016; 65 (2); 1-48.
Dumler JS, Madigan JE, Pusterla N, Bakken JS. Ehrlichioses in humans: epidemiology, clinical presentation, diagnosis, and treatment. Clin Infect Dis 2007 Jul 15;45 Suppl 1:S45–51.
Engel J, Bradley K, et al. Revision of the national surveillance case definition for ehrlichiosis [PDF – 36 KB]. Council of State and Territorial Epidemiologists, Infectious Diseases Committee, 2007 Position Statement.
Gelfand JA, Vannier E. Ehrlichia chaffeensis (human monocytotropic ehrlichiosis), Anaplasma phagocytophilum (human granulocytotropic anaplasmosis) and other ehrlichiae. In: Mandell GL, Bennett JE, Dolin R, editors. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. 6th ed. Philadelphia, PA: Churchill Livingstone; 2005. p. 2310–2318.
Johnson DKH, Neitzel DF, Miller TK, Feist MA, Sloan LM, Eremeeva ME, Fritsche TR, Uphoff TS, Ray J, Schiffman E, Murphy D, Davis JP, Pritt BS. Five Years’ Experience with the Novel Human Ehrlichia sp. in the Upper Midwestern United States: 2009-2013. American Society of Tropical Medicine and Hygiene 63rd Annual Meeting, New Orleans, LA. November 2013.
Todd SR, Dahlgren FS, et al. No visible dental staining in children treated with doxycycline for suspected Rocky Mountain spotted fever. J Pediatr, available online 17 March 2015.
Reported Cases of Ehrlichiosis, U.S., 2015
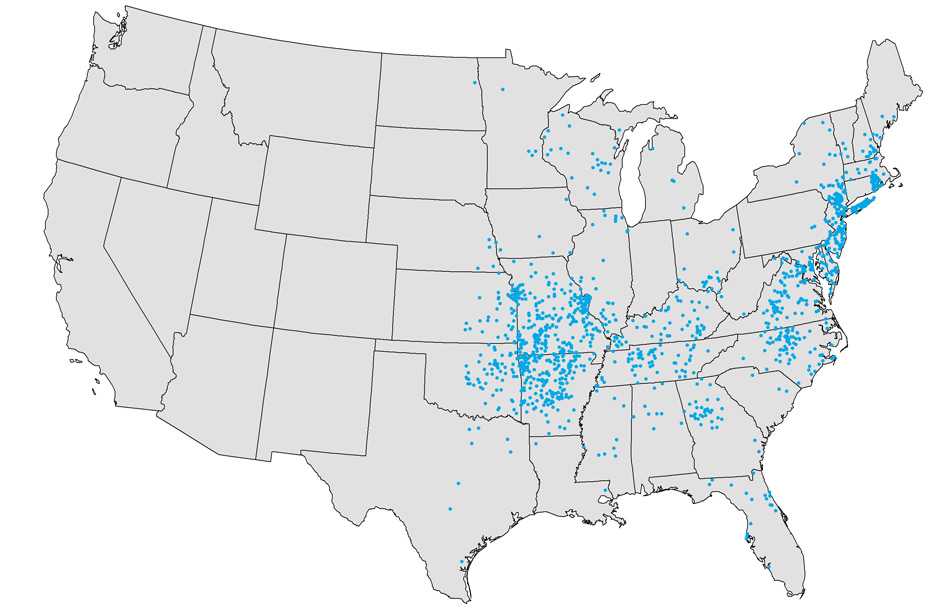
NOTE: Each dot represents one case. Cases are reported from the infected person’s county of residence, not necessarily the place where they were infected.
NOTE: In 2015, no cases of ehrlichiosis were reported from Hawaii or Alaska.
- Page last reviewed: October 23, 2014
- Page last updated: February 8, 2017
- Content source: