

Colorado Tick Fever
 ShareCompartir
ShareCompartir
Agent: Colorado tick fever virus
WHERE FOUND The geographic range of Colorado tick fever virus includes the western United States and southwestern Canada at elevations 4,000 to
10,000 feet. Cases occur primarily in Colorado, Utah, Montana, and Wyoming. Although rare, the virus can also be transmitted from person-to-person
via blood transfusion.
INCUBATION PERIOD: 1-14 days
SIGNS AND SYPMTOMS
- Fever, chills, headache, myalgias, and lethargy
- ~50% of patients have a biphasic illness with symptoms remitting after 2 to 4 days, but then recurring 1 to 3 days later
- Conjunctival injection, pharyngeal erythema and lymphadenopathy may be present
- Maculopapular or petechial rash in <20% of patients
- Prolonged convalescence characterized by weakness and fatigue is common in adults
- Life-threatening complications and death are rare and usually associated with disseminated intravascular coagulation or meningoencephalitis in children
GENERAL LABORATORY FINDINGS
- Leukopenia
- Moderate thrombocytopenia
LABORATORY DIAGNOSIS
- Culture and RT-PCR during first 2 weeks of illness
- Serologic assays (e.g., IgM-capture EIA, indirect fluorescent antibody, and plaque-reduction neutralization) on convalescent samples. IgM antibodies usually do not appear until 14–21 days after illness onset.
TREATMENT
No specific antiviral treatment is available. Patients with suspected CTF should receive supportive care as appropriate. Patients with confirmed CTF should defer blood and bone marrow donation for at least 6 months after recovery.
References
Brackney MM, Marfin AA, Staples JE, et al. Epidemiology of Colorado tick fever in Montana, Utah, and Wyoming, 1995–2003. Vector Borne Zoonotic Dis 2010;10:381–385.
Centers for Disease Control and Prevention. West Nile virus and other nationally notifiable arboviral diseases—United States, 2015. MMWR 2017; 66(02);51-55.
Fischer M, Tsai TF. Coltiviruses (Colorado Tick Fever). In: Principles and Practice of Pediatric Infectious Diseases, 3rd edition. Eds: Long SS, Pickering LK, Prober CG. Elsevier 2008:1076–1078.
Goodpasture HC, Poland JD, Francy DB, Bowen GS, Horn KA. Colorado tick fever: clinical, epidemiologic, and laboratory aspects of 228 cases in Colorado in 1973–1974. Ann Intern Med 1978;88:303–310.
Lambert AJ, Kosoy O, Velez JO, Russell BJ, Lanciotti RS. Detection of Colorado Tick Fever viral RNA in acute human serum samples by a quantitative real-time RT-PCR assay. J Virol Methods 2007;140:43–48.
Romero JR, Simonsen KA. Powassan encephalitis and Colorado tick fever. Infect Dis Clin North Am 2008;22:545–559.
Spruance SL, Bailey A. Colorado Tick Fever. A review of 115 laboratory confirmed cases. Arch Intern Med 1973;131:288–293.
Approximate geographic distribution of Dermacentor andersoni ticks and counties of residence for confirmed and probable Colorado tick fever (CTF) virus disease cases, United States, 2002–2012
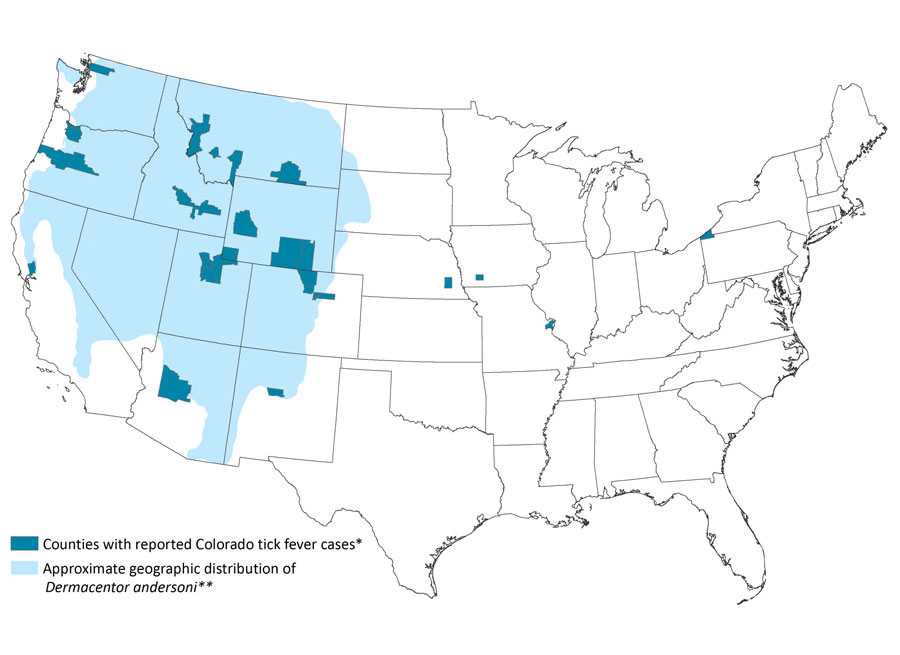
* All cases were acquired in states where local transmission of CTF virus has been reported previously. Two additional cases were reported from Colorado with unknown county of residence.
**Derived from James AM, Freier JE, Keirans JE, Durden LA, et al. Distribution, seasonality, and hosts of the Rocky Mountain wood tick in the United States. J Med Entomol 2006; 43:17–24.
- Page last reviewed: October 23, 2014
- Page last updated: February 1, 2017
- Content source: