Congenital rubella syndrome
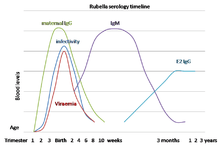
Congenital rubella syndrome (CRS) can occur in a developing fetus of a pregnant woman who has contracted rubella, usually in the first trimester. If infection occurs 0–28 days before conception, the infant has a 43% risk of being affected. If the infection occurs 0–12 weeks after conception, the risk increases to 81%. If the infection occurs 13–26 weeks after conception, the risk is 54% of the infant being affected by the disease. Infants are not generally affected if rubella is contracted during the third trimester, or 26–40 weeks after conception. Problems rarely occur when rubella is contracted by the mother after 20 weeks of gestation and continues to disseminate the virus after birth.
| Congenital rubella syndrome | |
|---|---|
_PHIL_4284_lores.jpg) | |
| White pupils due to congenital cataracts in a child with congenital rubella syndrome | |
| Specialty | Teratology |
It was discovered in 1941 by Australian Norman McAlister Gregg.[1]
Signs and symptoms

The classic triad for congenital rubella syndrome is:[3]
- Sensorineural deafness (58% of patients)
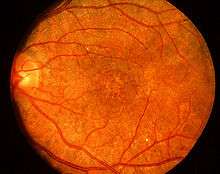
- Eye abnormalities—especially retinopathy, cataract, glaucoma, and microphthalmia (43% of patients)
- Congenital heart disease—especially pulmonary artery stenosis and patent ductus arteriosus (50% of patients)[4]
Other manifestations of CRS may include:
- Spleen, liver, or bone marrow problems (some of which may disappear shortly after birth)
- Intellectual disability
- Small head size (microcephaly)
- Eye defects
- Low birth weight[5]
- Thrombocytopenic purpura
- Extramedullary hematopoiesis (presents as a characteristic blueberry muffin rash)
- Enlarged liver
- Small jaw size
- Skin Lesions [5]
Children who have been exposed to rubella in the womb should also be watched closely as they age for any indication of:
- Developmental delay[5]
- Autism[6]
- Schizophrenia[7]
- Growth retardation[8]
- Learning disabilities
- Diabetes mellitus[9]
Prevention
Vaccinating the majority of the population is effective at preventing congenital rubella syndrome.[10] For females who plan on pregnancy, the MMR (measles mumps, rubella) vaccination is highly recommend, at least 28 days prior to conception.[5] If already pregnant, vaccination is strictly prohibited as the vaccine contains a live version of the virus.[5]
Other preventative actions can include the screening and vaccinations of high-risk personal, such as medical and child care professions.[11]
References
- Atkinson, William (2011). Epidemiology and Prevention of Vaccine-Preventable Diseases (12th ed.). Public Health Foundation. pp. 301–323. ISBN 9780983263135. Retrieved 30 March 2015.
- Sudharshan S, Ganesh SK, Biswas J (2010). "Current approach in the diagnosis and management of posterior uveitis". Indian J Ophthalmol. 58 (1): 29–43. doi:10.4103/0301-4738.58470. ISSN 0301-4738. PMC 2841371. PMID 20029144.
- "Congenital rubella syndrome | Sense". www.sense.org.uk. Retrieved 2015-07-30.
- Oster ME, Riehle-Colarusso T, Correa A (January 2010). "An update on cardiovascular malformations in congenital rubella syndrome". Clin Mol Teratol. 88 (1): 1–8. doi:10.1002/bdra.20621. PMID 19697432.
- "Congenital Rubella Symptoms & Causes | Boston Children's Hospital". www.childrenshospital.org. Retrieved 2019-03-05.
- Muhle, R; Trentacoste, SV; Rapin, I (May 2004). "The genetics of autism". Pediatrics. 113 (5): e472–86. doi:10.1542/peds.113.5.e472. PMID 15121991.
- Brown, A. S (9 February 2006). "Prenatal Infection as a Risk Factor for Schizophrenia". Schizophrenia Bulletin. 32 (2): 200–202. doi:10.1093/schbul/sbj052. PMC 2632220. PMID 16469941.
- Naeye, Richard L. (1965-12-20). "Pathogenesis of congenital rubella". JAMA. 194 (12): 1277–1283. doi:10.1001/jama.1965.03090250011002. ISSN 0098-7484.
- Forrest, Jill M.; Menser, Margaret A.; Burgess, J. A. (1971-08-14). "High Frequency of Diabetes Mellitus in Young Adults with Congenital Rubella". The Lancet. 298 (7720): 332–334. doi:10.1016/S0140-6736(71)90057-2. PMID 4105044.
- "Rubella vaccines: WHO position paper" (PDF). Wkly Epidemiol Rec. 86 (29): 301–16. 15 July 2011. PMID 21766537.
- "Congenital Rubella - Pediatrics". Merck Manuals Professional Edition. Retrieved 2019-03-05.
External links
| Classification | |
|---|---|
| External resources |