Anaphylaxis
Anaphylaxis is a serious allergic reaction that is rapid in onset and may cause death.[4][5] It typically causes more than one of the following: an itchy rash, throat or tongue swelling, shortness of breath, vomiting, lightheadedness, and low blood pressure.[1] These symptoms typically come on over minutes to hours.[1]
| Anaphylaxis | |
|---|---|
 | |
| Angioedema of the face such that the boy cannot open his eyes. This reaction was caused by an allergen exposure. | |
| Specialty | Allergy and immunology |
| Symptoms | Itchy rash, throat swelling, shortness of breath, lightheadedness[1] |
| Usual onset | Over minutes to hours[1] |
| Causes | Insect bites, foods, medications[1] |
| Diagnostic method | Based on symptoms[2] |
| Differential diagnosis | Allergic reaction, angioedema, asthma exacerbation, carcinoid syndrome[2] |
| Treatment | Epinephrine, intravenous fluids[1] |
| Frequency | 0.05–2%[3] |
Common causes include insect bites and stings, foods, and medications.[1] Other causes include latex exposure and exercise.[1] Additionally, cases may occur without an obvious reason.[1] The mechanism involves the release of mediators from certain types of white blood cells triggered by either immunologic or non-immunologic mechanisms.[6] Diagnosis is based on the presenting symptoms and signs after exposure to a potential allergen.[1]
The primary treatment of anaphylaxis is epinephrine injection into a muscle, intravenous fluids, and positioning the person flat.[1][7] Additional doses of epinephrine may be required.[1] Other measures, such as antihistamines and steroids, are complementary.[1] Carrying an epinephrine autoinjector and identification regarding the condition is recommended in people with a history of anaphylaxis.[1]
Worldwide, 0.05–2% of the population is estimated to experience anaphylaxis at some point in life.[3] Rates appear to be increasing.[3] It occurs most often in young people and females.[7][8] Of people who go to a hospital with anaphylaxis in the United States about 99.7% survive.[9] The term comes from the Ancient Greek: ἀνά, romanized: ana, lit. 'against', and the Ancient Greek: φύλαξις, romanized: phylaxis, lit. 'protection'.[10]
Signs and symptoms
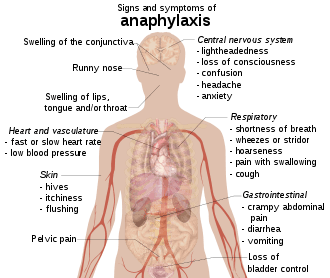
Anaphylaxis typically presents many different symptoms over minutes or hours[7][11] with an average onset of 5 to 30 minutes if exposure is intravenous and 2 hours if from eating food.[12] The most common areas affected include: skin (80–90%), respiratory (70%), gastrointestinal (30–45%), heart and vasculature (10–45%), and central nervous system (10–15%)[13] with usually two or more being involved.[3]
Skin

Symptoms typically include generalized hives, itchiness, flushing, or swelling (angioedema) of the afflicted tissues.[4] Those with angioedema may describe a burning sensation of the skin rather than itchiness.[12] Swelling of the tongue or throat occurs in up to about 20% of cases.[14] Other features may include a runny nose and swelling of the conjunctiva.[15] The skin may also be blue tinged because of lack of oxygen.[15]
Respiratory
Respiratory symptoms and signs that may be present include shortness of breath, wheezes, or stridor.[4] The wheezing is typically caused by spasms of the bronchial muscles[16] while stridor is related to upper airway obstruction secondary to swelling.[15] Hoarseness, pain with swallowing, or a cough may also occur.[12]
Cardiovascular
While a fast heart rate caused by low blood pressure is more common,[15] a Bezold–Jarisch reflex has been described in 10% of people, where a slow heart rate is associated with low blood pressure.[8] A drop in blood pressure or shock (either distributive or cardiogenic) may cause the feeling of lightheadedness or loss of consciousness.[16] Rarely very low blood pressure may be the only sign of anaphylaxis.[14]
Coronary artery spasm may occur with subsequent myocardial infarction, dysrhythmia, or cardiac arrest.[3][13] Those with underlying coronary disease are at greater risk of cardiac effects from anaphylaxis.[16] The coronary spasm is related to the presence of histamine-releasing cells in the heart.[16]
Other
Gastrointestinal symptoms may include crampy abdominal pain, diarrhea, and vomiting.[4] There may be confusion, a loss of bladder control or pelvic pain similar to that of uterine cramps.[4][15] Dilation of blood vessels around the brain may cause headaches.[12] A feeling of anxiety or of "impending doom" has also been described.[3]
Causes
Anaphylaxis can occur in response to almost any foreign substance.[17] Common triggers include venom from insect bites or stings, foods, and medication.[8][18] Foods are the most common trigger in children and young adults while medications and insect bites and stings are more common in older adults.[3] Less common causes include: physical factors, biological agents such as semen, latex, hormonal changes, food additives such as monosodium glutamate and food colors, and topical medications.[15] Physical factors such as exercise (known as exercise-induced anaphylaxis) or temperature (either hot or cold) may also act as triggers through their direct effects on mast cells.[3][19] Events caused by exercise are frequently associated with the ingestion of certain foods.[12] During anesthesia, neuromuscular blocking agents, antibiotics, and latex are the most common causes.[20] The cause remains unknown in 32–50% of cases, referred to as "idiopathic anaphylaxis."[21] Six vaccines (MMR, varicella, influenza, hepatitis B, tetanus, meningococcal) are recognized as a cause for anaphylaxis, and HPV may cause anaphylaxis as well.[22] Physical exercise is an uncommon cause of anaphylaxis;[23] in about a third of such cases there is a co-factor like taking an NSAID or eating a specific food prior to exercising.[24]
Food
Many foods can trigger anaphylaxis; this may occur upon the first known ingestion.[8] Common triggering foods vary around the world. In Western cultures, ingestion of or exposure to peanuts, wheat, nuts, certain types of seafood like shellfish, milk, and eggs are the most prevalent causes.[3][13] Sesame is common in the Middle East, while rice and chickpeas are frequently encountered as sources of anaphylaxis in Asia.[3] Severe cases are usually caused by ingesting the allergen,[8] but some people experience a severe reaction upon contact. Children can outgrow their allergies. By age 16, 80% of children with anaphylaxis to milk or eggs and 20% who experience isolated anaphylaxis to peanuts can tolerate these foods.[17]
Medication
Any medication may potentially trigger anaphylaxis. The most common are β-lactam antibiotics (such as penicillin) followed by aspirin and NSAIDs.[13][25] Other antibiotics are implicated less frequently.[25] Anaphylactic reactions to NSAIDs are either agent specific or occur among those that are structurally similar meaning that those who are allergic to one NSAID can typically tolerate a different one or different group of NSAIDs.[26] Other relatively common causes include chemotherapy, vaccines, protamine and herbal preparations.[3] Some medications (vancomycin, morphine, x-ray contrast among others) cause anaphylaxis by directly triggering mast cell degranulation.[8]
The frequency of a reaction to an agent partly depends on the frequency of its use and partly on its intrinsic properties.[27] Anaphylaxis to penicillin or cephalosporins occurs only after it binds to proteins inside the body with some agents binding more easily than others.[12] Anaphylaxis to penicillin occurs once in every 2,000 to 10,000 courses of treatment, with death occurring in fewer than one in every 50,000 courses of treatment.[12] Anaphylaxis to aspirin and NSAIDs occurs in about one in every 50,000 persons.[12] If someone has a reaction to penicillins, his or her risk of a reaction to cephalosporins is greater but still less than one in 1,000.[12] The old radiocontrast agents caused reactions in 1% of cases, while the newer lower osmolar agents cause reactions in 0.04% of cases.[27]
Venom
Venom from stinging or biting insects such as Hymenoptera (ants, bees, and wasps) or Triatominae (kissing bugs) may cause anaphylaxis in susceptible people.[7][28][29] Previous reactions, that are anything more than a local reaction around the site of the sting, are a risk factor for future anaphylaxis;[30][31] however, half of fatalities have had no previous systemic reaction.[32]
Risk factors
People with atopic diseases such as asthma, eczema, or allergic rhinitis are at high risk of anaphylaxis from food, latex, and radiocontrast agents but not from injectable medications or stings.[3][8] One study in children found that 60% had a history of previous atopic diseases, and of children who die from anaphylaxis, more than 90% have asthma.[8] Those with mastocytosis or of a higher socioeconomic status are at increased risk.[3][8] The longer the time since the last exposure to the agent in question, the lower the risk.[12]
Pathophysiology
Anaphylaxis is a severe allergic reaction of rapid onset affecting many body systems.[5][6] It is due to the release of inflammatory mediators and cytokines from mast cells and basophils, typically due to an immunologic reaction but sometimes non-immunologic mechanism.[6]
Immunologic
In the immunologic mechanism, immunoglobulin E (IgE) binds to the antigen (the foreign material that provokes the allergic reaction). Antigen-bound IgE then activates FcεRI receptors on mast cells and basophils. This leads to the release of inflammatory mediators such as histamine. These mediators subsequently increase the contraction of bronchial smooth muscles, trigger vasodilation, increase the leakage of fluid from blood vessels, and cause heart muscle depression.[6][12] There is also an immunologic mechanism that does not rely on IgE, but it is not known if this occurs in humans.[6]
Non-immunologic
Non-immunologic mechanisms involve substances that directly cause the degranulation of mast cells and basophils. These include agents such as contrast medium, opioids, temperature (hot or cold), and vibration.[6][19] Sulfites may cause reactions by both immunologic and non-immunologic mechanisms.[33]
Diagnosis
Anaphylaxis is diagnosed on the basis of a person's signs and symptoms.[3] When any one of the following three occurs within minutes or hours of exposure to an allergen there is a high likelihood of anaphylaxis:[3]
- Involvement of the skin or mucosal tissue plus either respiratory difficulty or a low blood pressure causing symptoms
- Two or more of the following symptoms after a likely contact with an allergen:
- a. Involvement of the skin or mucosa
- b. Respiratory difficulties
- c. Low blood pressure
- d. Gastrointestinal symptoms
- Low blood pressure after exposure to a known allergen
Skin involvement may include: hives, itchiness or a swollen tongue among others. Respiratory difficulties may include: shortness of breath, stridor, or low oxygen levels among others. Low blood pressure is defined as a greater than 30% decrease from a person's usual blood pressure. In adults a systolic blood pressure of less than 90 mmHg is often used.[3]
During an attack, blood tests for tryptase or histamine (released from mast cells) might be useful in diagnosing anaphylaxis due to insect stings or medications. However these tests are of limited use if the cause is food or if the person has a normal blood pressure,[3] and they are not specific for the diagnosis.[17]
Classification
There are three main classifications of anaphylaxis. Anaphylactic shock is associated with systemic vasodilation that causes low blood pressure which is by definition 30% lower than the person's baseline or below standard values.[14] Biphasic anaphylaxis is the recurrence of symptoms within 1–72 hours with no further exposure to the allergen.[3] Reports of incidence vary, with some studies claiming as many as 20% of cases.[34] The recurrence typically occurs within 8 hours.[8] It is managed in the same manner as anaphylaxis.[7] Pseudoanaphylaxis or anaphylactoid reactions are a type of anaphylaxis that does not involve an allergic reaction but is due to direct mast cell degranulation.[8][35] Non-immune anaphylaxis is the current term used by the World Allergy Organization[35] with some recommending that the old terminology no longer be used.[8]
Allergy testing

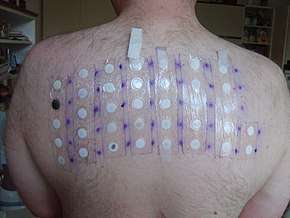
Allergy testing may help in determining the trigger. Skin allergy testing is available for certain foods and venoms.[17] Blood testing for specific IgE can be useful to confirm milk, egg, peanut, tree nut and fish allergies.[17]
Skin testing is available to confirm penicillin allergies, but is not available for other medications.[17] Non-immune forms of anaphylaxis can only be determined by history or exposure to the allergen in question, and not by skin or blood testing.[35]
Differential diagnosis
It can sometimes be difficult to distinguish anaphylaxis from asthma, syncope, and panic attacks.[3] Asthma however typically does not entail itching or gastrointestinal symptoms, syncope presents with pallor rather than a rash, and a panic attack may have flushing but does not have hives.[3] Other conditions that may present similarly include: scrombroidosis and anisakiasis.[8]
Post-mortem findings
In a person who died from anaphylaxis, autopsy may show an "empty heart" attributed to reduced venous return from vasodilation and redistribution of intravascular volume from the central to the peripheral compartment.[36] Other signs are laryngeal edema, eosinophilia in lungs, heart and tissues, and evidence of myocardial hypoperfusion.[37] Laboratory findings could detect increased levels of serum tryptase, increase in total and specific IgE serum levels.[37]
Prevention
Avoidance of the trigger of anaphylaxis is recommended. In cases where this may not be possible, desensitization may be an option. Immunotherapy with Hymenoptera venoms is effective at desensitizing 80–90% of adults and 98% of children against allergies to bees, wasps, hornets, yellowjackets, and fire ants. Oral immunotherapy may be effective at desensitizing some people to certain food including milk, eggs, nuts and peanuts; however, adverse effects are common.[3] For example, many people develop an itchy throat, cough, or lip swelling during immunotherapy.[38] Desensitization is also possible for many medications, however it is advised that most people simply avoid the agent in question. In those who react to latex it may be important to avoid cross-reactive foods such as avocados, bananas, and potatoes among others.[3]
Management
Anaphylaxis is a medical emergency that may require resuscitation measures such as airway management, supplemental oxygen, large volumes of intravenous fluids, and close monitoring.[7] Administration of epinephrine is the treatment of choice with antihistamines and steroids (for example, dexamethasone) often used as adjuncts.[7] A period of in-hospital observation for between 2 and 24 hours is recommended for people once they have returned to normal due to concerns of biphasic anaphylaxis.[8][12][34][39]
Epinephrine

Epinephrine (adrenaline) is the primary treatment for anaphylaxis with no absolute contraindication to its use.[7] It is recommended that an epinephrine solution be given intramuscularly into the mid anterolateral thigh as soon as the diagnosis is suspected. The injection may be repeated every 5 to 15 minutes if there is insufficient response.[7] A second dose is needed in 16–35% of episodes with more than two doses rarely required.[7] The intramuscular route is preferred over subcutaneous administration because the latter may have delayed absorption.[7][40] Minor adverse effects from epinephrine include tremors, anxiety, headaches, and palpitations.[3]
People on β-blockers may be resistant to the effects of epinephrine.[8] In this situation if epinephrine is not effective intravenous glucagon can be administered which has a mechanism of action independent of β-receptors.[8]
If necessary, it can also be given intravenously using a dilute epinephrine solution. Intravenous epinephrine, however, has been associated both with dysrhythmia and myocardial infarction.[7] Epinephrine autoinjectors used for self-administration typically come in two doses, one for adults or children who weigh more than 25 kg and one for children who weigh 10 to 25 kg.[41]
Adjuncts
Antihistamines (both H1 and H2), while commonly used and assumed effective based on theoretical reasoning, are poorly supported by evidence.[42][43] A 2007 Cochrane review did not find any good-quality studies upon which to base recommendations[43] and they are not believed to have an effect on airway edema or spasm.[8] Corticosteroids are unlikely to make a difference in the current episode of anaphylaxis, but may be used in the hope of decreasing the risk of biphasic anaphylaxis. Their prophylactic effectiveness in these situations is uncertain.[34] Nebulized salbutamol may be effective for bronchospasm that does not resolve with epinephrine.[8] Methylene blue has been used in those not responsive to other measures due to its presumed effect of relaxing smooth muscle.[8]
Preparedness
People prone to anaphylaxis are advised to have an "allergy action plan." Parents are advised to inform schools of their children's allergies and what to do in case of an anaphylactic emergency. The action plan usually includes use of epinephrine autoinjectors, the recommendation to wear a medical alert bracelet, and counseling on avoidance of triggers.[44] Immunotherapy is available for certain triggers to prevent future episodes of anaphylaxis. A multi-year course of subcutaneous desensitization has been found effective against stinging insects, while oral desensitization is effective for many foods.[13]
Prognosis
In those in whom the cause is known and prompt treatment is available, the prognosis is good.[45] Even if the cause is unknown, if appropriate preventative medication is available, the prognosis is generally good.[12] If death occurs, it is usually due to either respiratory (typically asphyxia) or cardiovascular causes (shock),[6][8] with 0.7–20% of cases causing death.[12][16] There have been cases of death occurring within minutes.[3] Outcomes in those with exercise-induced anaphylaxis are typically good, with fewer and less severe episodes as people get older.[21]
Epidemiology
The number of people who get anaphylaxis is 4–100 per 100,000 persons per year,[8][46] with a lifetime risk of 0.05–2%.[47] About 30% of people get more than one attack.[46] Exercise-induced anaphylaxis affects about 1 in 2000 young people.[24]
Rates appear to be increasing: with the numbers in the 1980s being approximately 20 per 100,000 per year, while in the 1990s it was 50 per 100,000 per year.[13] The increase appears to be primarily for food-induced anaphylaxis.[48] The risk is greatest in young people and females.[7][8]
Anaphylaxis leads to as many as 500–1,000 deaths per year (2.7 per million) in the United States, 20 deaths per year in the United Kingdom (0.33 per million), and 15 deaths per year in Australia (0.64 per million).[8] Another estimate from the United States puts the death rate at 0.7 per million.[49] Mortality rates have decreased between the 1970s and 2000s.[50] In Australia, death from food-induced anaphylaxis occur primarily in women while deaths due to insect bites primarily occur in males.[8] Death from anaphylaxis is most commonly triggered by medications.[8]
History
The term aphylaxis was coined by Charles Richet in 1902 and later changed to anaphylaxis due to its nicer quality of speech.[17] In his experiments, Richet injected a dog with sea anemone (Actinia) toxin in an attempt to protect it. Although the dog had previously tolerated the toxin, on re-exposure, three weeks later with the same dose, it developed fatal anaphylaxis. Thus instead of inducing tolerance (prophylaxis), when lethal responses resulted from previously tolerated doses, he coined the word a (without) phylaxis (protection). He was subsequently awarded the Nobel Prize in Physiology or Medicine for his work on anaphylaxis in 1913.[12] The phenomenon itself, however, has been described since ancient times.[35] The term comes from the Greek words ἀνά, ana, meaning "against", and φύλαξις, phylaxis, meaning "protection".[51]
Research
There are ongoing efforts to develop sublingual epinephrine to treat anaphylaxis.[8] Subcutaneous injection of the anti-IgE antibody omalizumab is being studied as a method of preventing recurrence, but it is not yet recommended.[3][52]
References
- "Anaphylaxis". National Institute of Allergy and Infectious Diseases. April 23, 2015. Archived from the original on 4 May 2015. Retrieved 4 February 2016.
- Caterino, Jeffrey M.; Kahan, Scott (2003). In a Page: Emergency medicine. Lippincott Williams & Wilkins. p. 132. ISBN 9781405103572. Archived from the original on 2017-09-08.
- Simons, FE; Ardusso, LR; Bilò, MB; El-Gamal, YM; Ledford, DK; Ring, J; Sanchez-Borges, M; Senna, GE; Sheikh, A; Thong, BY; World Allergy, Organization. (February 2011). "World allergy organization guidelines for the assessment and management of anaphylaxis". The World Allergy Organization Journal. 4 (2): 13–37. doi:10.1097/wox.0b013e318211496c. PMC 3500036. PMID 23268454.
- Sampson HA, Muñoz-Furlong A, Campbell RL, et al. (February 2006). "Second symposium on the definition and management of anaphylaxis: summary report—Second National Institute of Allergy and Infectious Disease/Food Allergy and Anaphylaxis Network symposium". The Journal of Allergy and Clinical Immunology. 117 (2): 391–7. doi:10.1016/j.jaci.2005.12.1303. PMID 16461139.
- Tintinalli, Judith E. (2010). Emergency Medicine: A Comprehensive Study Guide (Emergency Medicine (Tintinalli)). New York: McGraw-Hill Companies. pp. 177–182. ISBN 978-0-07-148480-0.
- Khan, BQ; Kemp, SF (August 2011). "Pathophysiology of anaphylaxis". Current Opinion in Allergy and Clinical Immunology. 11 (4): 319–25. doi:10.1097/ACI.0b013e3283481ab6. PMID 21659865.
- The EAACI Food Allergy and Anaphylaxis Guidelines Group (August 2014). "Anaphylaxis: guidelines from the European Academy of Allergy and Clinical Immunology". Allergy. 69 (8): 1026–45. doi:10.1111/all.12437. PMID 24909803.
- Lee, JK; Vadas, P (July 2011). "Anaphylaxis: mechanisms and management". Clinical and Experimental Allergy. 41 (7): 923–38. doi:10.1111/j.1365-2222.2011.03779.x. PMID 21668816.
- Ma, L; Danoff, TM; Borish, L (April 2014). "Case fatality and population mortality associated with anaphylaxis in the United States". The Journal of Allergy and Clinical Immunology. 133 (4): 1075–83. doi:10.1016/j.jaci.2013.10.029. PMC 3972293. PMID 24332862.
- Gylys, Barbara (2012). Medical Terminology Systems: A Body Systems Approach. F.A. Davis. p. 269. ISBN 9780803639133. Archived from the original on 2016-02-05.
- Oswalt ML, Kemp SF (May 2007). "Anaphylaxis: office management and prevention". Immunol Allergy Clin North Am. 27 (2): 177–91, vi. doi:10.1016/j.iac.2007.03.004. PMID 17493497.
Clinically, anaphylaxis is considered likely to be present if any one of three criteria is satisfied within minutes to hours
- Marx, John (2010). Rosen's emergency medicine: concepts and clinical practice 7th edition. Philadelphia, PA: Mosby/Elsevier. p. 1511–1528. ISBN 978-0-323-05472-0.
- Simons FE (October 2009). "Anaphylaxis: Recent advances in assessment and treatment". The Journal of Allergy and Clinical Immunology. 124 (4): 625–36, quiz 637–8. doi:10.1016/j.jaci.2009.08.025. PMID 19815109.
- Limsuwan, T; Demoly, P (July 2010). "Acute symptoms of drug hypersensitivity (urticaria, angioedema, anaphylaxis, anaphylactic shock)" (PDF). The Medical Clinics of North America. 94 (4): 691–710, x. doi:10.1016/j.mcna.2010.03.007. PMID 20609858. Archived (PDF) from the original on 2012-04-26.
- Brown, SG; Mullins, RJ; Gold, MS (Sep 4, 2006). "Anaphylaxis: diagnosis and management". The Medical Journal of Australia. 185 (5): 283–9. doi:10.5694/j.1326-5377.2006.tb00563.x. hdl:2440/23292. PMID 16948628.
- Triggiani, M; Patella, V; Staiano, RI; Granata, F; Marone, G (September 2008). "Allergy and the cardiovascular system". Clinical and Experimental Immunology. 153 Suppl 1 (s1): 7–11. doi:10.1111/j.1365-2249.2008.03714.x. PMC 2515352. PMID 18721322.
- Boden, SR; Wesley Burks, A (July 2011). "Anaphylaxis: a history with emphasis on food allergy". Immunological Reviews. 242 (1): 247–57. doi:10.1111/j.1600-065X.2011.01028.x. PMC 3122150. PMID 21682750.
- Worm, M (2010). Epidemiology of anaphylaxis. Chemical Immunology and Allergy. 95. pp. 12–21. doi:10.1159/000315935. ISBN 978-3-8055-9441-7. PMID 20519879.
- editors, Marianne Gausche-Hill, Susan Fuchs, Loren Yamamoto (2007). The pediatric emergency medicine resource (Rev. 4. ed.). Sudbury, Mass.: Jones & Bartlett. p. 69. ISBN 978-0-7637-4414-4. Archived from the original on 2016-12-23.
- Dewachter, P; Mouton-Faivre, C; Emala, CW (November 2009). "Anaphylaxis and anesthesia: controversies and new insights". Anesthesiology. 111 (5): 1141–50. doi:10.1097/ALN.0b013e3181bbd443. PMID 19858877.
- editor, Mariana C. Castells (2010). Anaphylaxis and hypersensitivity reactions. New York: Humana Press. p. 223. ISBN 978-1-60327-950-5. Archived from the original on 2016-12-23.
- Adverse Effects of Vaccines: Evidence and Causality (PDF). U.S. Institute of Medicine. 2011. ISBN 9780309214353. Archived from the original on 2017-09-08. Retrieved 2014-01-16.
- Feldweg, AM (May 2015). "Exercise-Induced Anaphylaxis". Immunology and Allergy Clinics of North America (Review). 35 (2): 261–75. doi:10.1016/j.iac.2015.01.005. PMID 25841550.
- Pravettoni, V; Incorvaia, C (2016). "Diagnosis of exercise-induced anaphylaxis: current insights". Journal of Asthma and Allergy. 9: 191–198. doi:10.2147/JAA.S109105. PMC 5089823. PMID 27822074.
- Simons FE, Ebisawa M, Sanchez-Borges M, Thong BY, Worm M, Tanno LK, Lockey RF, El-Gamal YM, Brown SG, Park HS, Sheikh A (2015). "2015 update of the evidence base: World Allergy Organization anaphylaxis guidelines". The World Allergy Organization Journal. 8 (1): 32. doi:10.1186/s40413-015-0080-1. PMC 4625730. PMID 26525001.
- Modena, B; White, AA; Woessner, KM (November 2017). "Aspirin and Nonsteroidal Antiinflammatory Drugs Hypersensitivity and Management". Immunology and Allergy Clinics of North America. 37 (4): 727–749. doi:10.1016/j.iac.2017.07.008. PMID 28965637.
- Drain, KL; Volcheck, GW (2001). "Preventing and managing drug-induced anaphylaxis". Drug Safety. 24 (11): 843–53. doi:10.2165/00002018-200124110-00005. PMID 11665871.
- Klotz, JH; Dorn, PL; Logan, JL; Stevens, L; Pinnas, JL; Schmidt, JO; Klotz, SA (Jun 15, 2010). ""Kissing bugs": potential disease vectors and cause of anaphylaxis". Clinical Infectious Diseases. 50 (12): 1629–34. doi:10.1086/652769. PMID 20462351.
- Brown, Simon G. A.; Wu, Qi-Xuan; Kelsall, G. Robert H.; Heddle, Robert J. & Baldo, Brian A. (2001). "Fatal anaphylaxis following jack jumper ant sting in southern Tasmania". Medical Journal of Australia. 175 (11): 644–647. doi:10.5694/j.1326-5377.2001.tb143761.x. PMID 11837875. Archived from the original on 2012-01-14.
- Bilò, MB (July 2011). "Anaphylaxis caused by Hymenoptera stings: from epidemiology to treatment". Allergy. 66 Suppl 95: 35–7. doi:10.1111/j.1398-9995.2011.02630.x. PMID 21668850.
- Cox, L; Larenas-Linnemann, D; Lockey, RF; Passalacqua, G (March 2010). "Speaking the same language: The World Allergy Organization Subcutaneous Immunotherapy Systemic Reaction Grading System". The Journal of Allergy and Clinical Immunology. 125 (3): 569–74, 574.e1–574.e7. doi:10.1016/j.jaci.2009.10.060. PMID 20144472.
- Bilò, BM; Bonifazi, F (August 2008). "Epidemiology of insect-venom anaphylaxis". Current Opinion in Allergy and Clinical Immunology. 8 (4): 330–7. doi:10.1097/ACI.0b013e32830638c5. PMID 18596590.
- Lewis, Julius M. Cruse, Robert E. (2010). Atlas of immunology (3rd ed.). Boca Raton, FL: CRC Press/Taylor & Francis. p. 411. ISBN 9781439802694. Archived from the original on 2017-03-20.
- Lieberman P (September 2005). "Biphasic anaphylactic reactions". Ann. Allergy Asthma Immunol. 95 (3): 217–26, quiz 226, 258. doi:10.1016/S1081-1206(10)61217-3. PMID 16200811.
- Ring, J; Behrendt, H; de Weck, A (2010). History and classification of anaphylaxis (PDF). Chemical Immunology and Allergy. 95. pp. 1–11. doi:10.1159/000315934. ISBN 978-3-8055-9441-7. PMID 20519878.
- Anaphylaxis at eMedicine
- Da Broi, U; Moreschi, C (Jan 30, 2011). "Post-mortem diagnosis of anaphylaxis: A difficult task in forensic medicine". Forensic Science International. 204 (1–3): 1–5. doi:10.1016/j.forsciint.2010.04.039. PMID 20684869.
- Simons, FE; Ardusso, LR; Dimov, V; Ebisawa, M; El-Gamal, YM; Lockey, RF; Sanchez-Borges, M; Senna, GE; Sheikh, A; Thong, BY; Worm, M; World Allergy, Organization. (2013). "World Allergy Organization Anaphylaxis Guidelines: 2013 update of the evidence base". International Archives of Allergy and Immunology. 162 (3): 193–204. doi:10.1159/000354543. PMID 24008815.
- "Emergency treatment of anaphylactic reactions – Guidelines for healthcare providers" (PDF). Resuscitation Council (UK). January 2008. Archived (PDF) from the original on 2008-12-02. Retrieved 2008-04-22.
- Simons, KJ; Simons, FE (August 2010). "Epinephrine and its use in anaphylaxis: current issues". Current Opinion in Allergy and Clinical Immunology. 10 (4): 354–61. doi:10.1097/ACI.0b013e32833bc670. PMID 20543673.
- Halbrich, M; Mack, DP; Carr, S; Watson, W; Kim, H (2015). "CSACI position statement: epinephrine auto-injectors and children < 15 kg". Allergy, Asthma, and Clinical Immunology. 11 (1): 20. doi:10.1186/s13223-015-0086-9. PMC 4485331. PMID 26131015.
- Nurmatov, UB; Rhatigan, E; Simons, FE; Sheikh, A (February 2014). "H2-antihistamines for the treatment of anaphylaxis with and without shock: a systematic review". Annals of Allergy, Asthma & Immunology. 112 (2): 126–31. doi:10.1016/j.anai.2013.11.010. PMID 24468252.
- Sheikh A, Ten Broek V, Brown SG, Simons FE (August 2007). "H1-antihistamines for the treatment of anaphylaxis: Cochrane systematic review". Allergy. 62 (8): 830–7. doi:10.1111/j.1398-9995.2007.01435.x. PMID 17620060.
- Martelli, A; Ghiglioni, D; Sarratud, T; Calcinai, E; Veehof, S; Terracciano, L; Fiocchi, A (August 2008). "Anaphylaxis in the emergency department: a paediatric perspective". Current Opinion in Allergy and Clinical Immunology. 8 (4): 321–9. doi:10.1097/ACI.0b013e328307a067. PMID 18596589.
- Harris JP, Weisman MH (2007-07-26). Head and Neck Manifestations of Systemic Disease. CRC Press. pp. 325–. ISBN 978-1-4200-1756-4.
- Tejedor-Alonso M, A; Moro-Moro, M; Múgica-García, MV (2015). "Epidemiology of Anaphylaxis: Contributions From the Last 10 Years". Journal of Investigational Allergology & Clinical Immunology. 25 (3): 163–75, quiz follow 174–5. PMID 26182682.
- Leslie C. Grammer (2012). Patterson's Allergic Diseases (7 ed.). ISBN 9781451148633. Archived from the original on 2015-06-20.
- Koplin, JJ; Martin, PE; Allen, KJ (October 2011). "An update on epidemiology of anaphylaxis in children and adults". Current Opinion in Allergy and Clinical Immunology. 11 (5): 492–6. doi:10.1097/ACI.0b013e32834a41a1. PMID 21760501.
- Fromer, L (December 2016). "Prevention of Anaphylaxis: The Role of the Epinephrine Auto-Injector". The American Journal of Medicine. 129 (12): 1244–1250. doi:10.1016/j.amjmed.2016.07.018. PMID 27555092.
- Demain, JG; Minaei, AA; Tracy, JM (August 2010). "Anaphylaxis and insect allergy". Current Opinion in Allergy and Clinical Immunology. 10 (4): 318–22. doi:10.1097/ACI.0b013e32833a6c72. PMID 20543675.
- "anaphylaxis". merriam-webster.com. Archived from the original on 2010-04-10. Retrieved 2009-11-21.
- Vichyanond, P (September 2011). "Omalizumab in allergic diseases, a recent review". Asian Pacific Journal of Allergy and Immunology. 29 (3): 209–19. PMID 22053590.
External links
| Classification | |
|---|---|
| External resources |
| Look up anaphylaxis in Wiktionary, the free dictionary. |
| Wikimedia Commons has media related to Anaphylaxis. |
- Anaphylaxis at Curlie
- National Institute for Health and Clinical Excellence. Clinical guideline 134: Anaphylaxis: assessment to confirm an anaphylactic episode and the decision to refer after emergency treatment for a suspected anaphylactic episode. London, 2011. and Anaphylaxis pathway
| Authority control |
|
|---|