

2016 STD Prevention Conference Highlights
 ShareCompartir
ShareCompartir
This web page is archived for historical purposes and is no longer being updated.
STD Prevention Systems
The 2016 STD Prevention Conference showcases the latest STD prevention research, both from the United States and abroad.
This page highlights two scientific posters specific to STD prevention systems. As we continue to navigate STD prevention within the evolving healthcare system, it is critical to ensure that we are reaching all patients, and especially the most vulnerable populations, with the essential services that make up quality STD care.
Poster or presentation images, as well as full abstracts and related links follow below.

Fast Facts
- STD case reports provided to CDC indicate that the majority of cases are reported in non-STD clinic settings, such as private physician offices and health maintenance organizations.
- There are 8,400 new HIV cases identified by STD clinics each year.
- The Affordable Care Act has reduced the number of uninsured people throughout the United States, but publicly funded STD services remain critical for millions.
STD Systems Abstracts
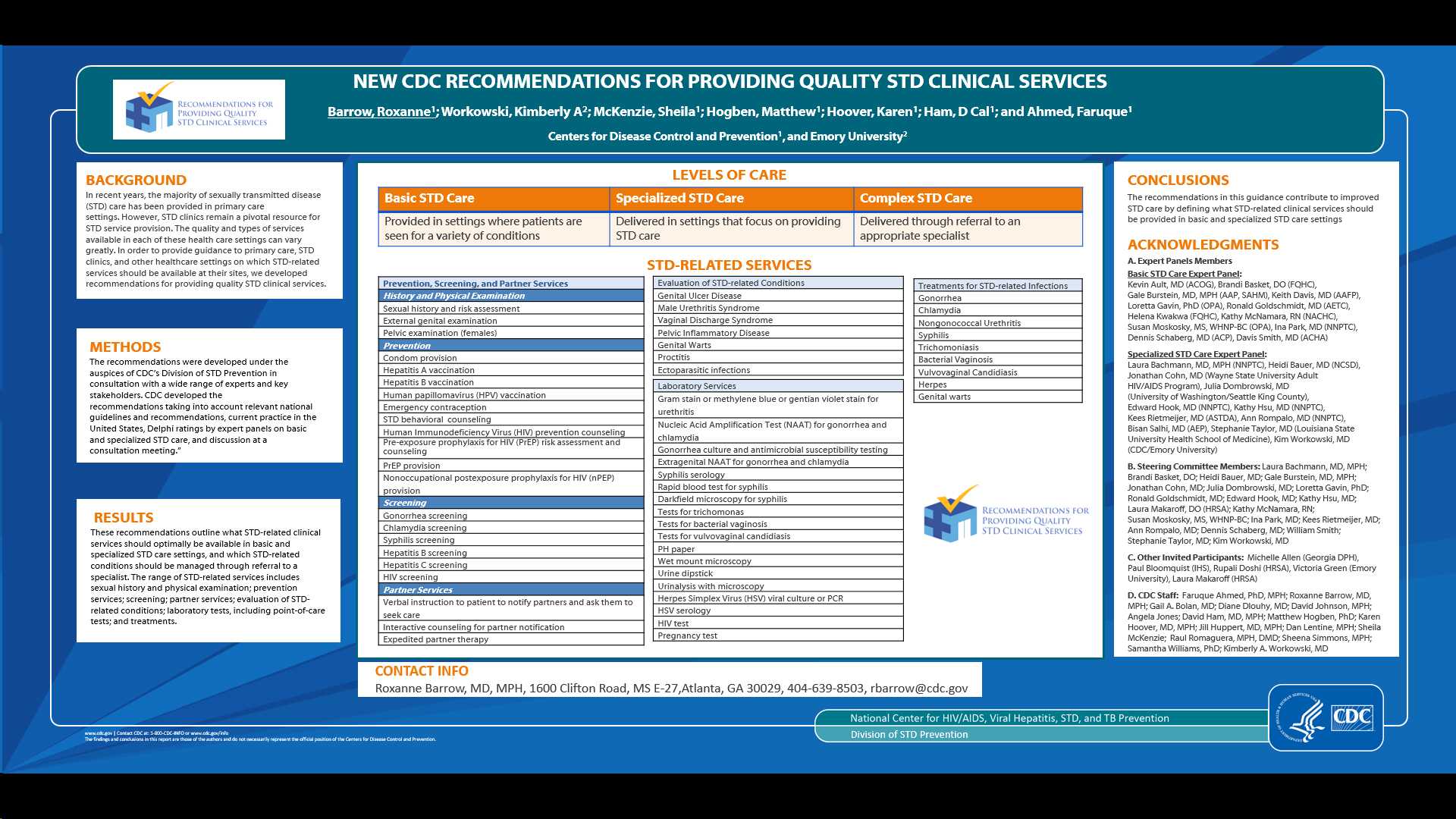
NEW CDC RECOMMENDATIONS FOR PROVIDING QUALITY STD CLINICAL SERVICES
Barrow, Roxanne1; Workowski, Kimberly A2; McKenzie, Sheila1; Hogben, Matthew1; Hoover, Karen1; Ham, D Cal1; and Ahmed, Faruque1
Centers for Disease Control and Prevention1, and Emory University2
Background: In recent years, the majority of sexually transmitted disease (STD) care has been provided in primary care settings. However, STD clinics remain a pivotal resource for STD service provision. The quality and types of services available in each of these health care settings can vary greatly. In order to provide guidance to primary care, STD clinics, and other healthcare settings on which STD-related services should be available at their sites, we developed recommendations for providing quality STD clinical services.
Methods: We reviewed the 2015 CDC STD Treatment Guidelines to generate a list of specific STD-related services, and conducted a systematic literature review to collect information on delivery of these services in a variety of U.S. healthcare settings. Using a modified Delphi method, we asked 29 STD experts from various key professional medical organizations about the services they thought should be available in basic and specialized STD care settings. In November 2015, we convened a consultation meeting of these experts and other stakeholders to discuss the proposed services for both settings.
Results: The recommendations outline essential services for the delivery of quality STD care in the United States. These new recommendations define two levels of STD service delivery, “basic” and “specialized” and provide guidance on the optimal services that should be available at each level. The range of STD-related services includes history and physical examination; prevention; screening; partner services; management of STD-related conditions; laboratory tests, including point of care tests; and on-site medications. Examples of pertinent STD services include brief behavioral counseling; HIV counseling; PrEP risk assessment; expedited partner therapy; nPEP medication for HIV and injectable medications for syphilis and gonorrhea.
Conclusions: The recommendations in this guidance contribute to improved STD care by defining what STD-related clinical services should be provided in basic and specialized STD care settings.
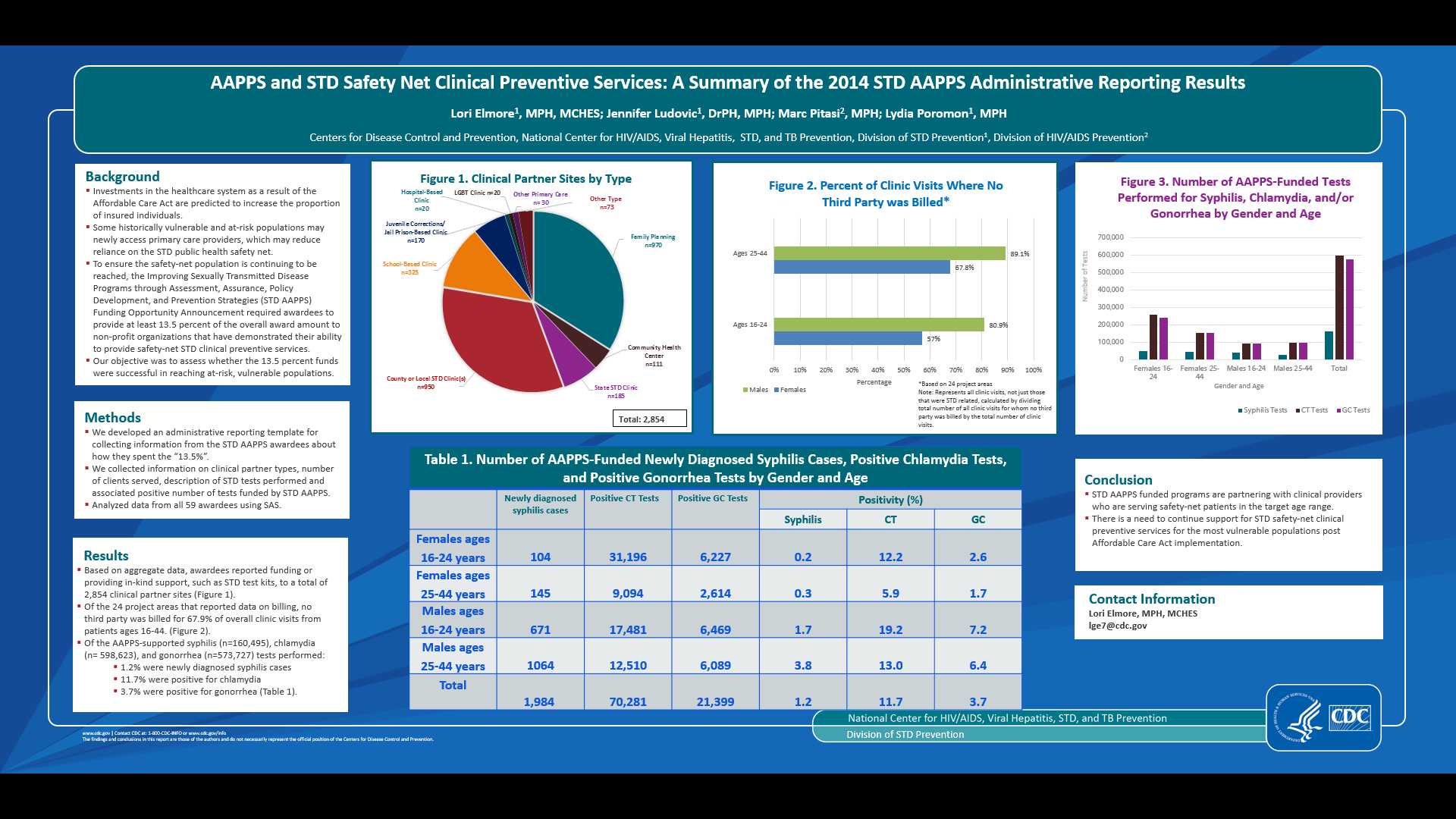
AAPPS AND STD SAFETY NET CLINICAL PREVENTIVE SERVICES: A SUMMARY OF THE 2014 STD AAPPS ADMINISTRATIVE REPORTING RESULTS
Lori Elmore, MPH, MCHES1, Jennifer Ludovic, DrPH, MPH1, Marc Pitasi, MPH2 and Lydia Poromon, MPH1
1Centers for Disease Control and Prevention, Division of STD Prevention, Atlanta, 2Centers for Disease Control and Prevention, Atlanta
Background: Investments in the healthcare system are predicted to increase the proportion of insured individuals. There will be shifts for some historically vulnerable and at-risk populations to an expanded network of primary care providers, which may reduce reliance on the STD public health safety net. In light of this, the Improving Sexually Transmitted Disease Programs through Assessment, Assurance, Policy Development, and Prevention Strategies (STD AAPPS) Funding Opportunity Announcement required awardees to provide at least 13.5 percent of the overall award amount to non-profit organizations that have demonstrated their ability to provide safety net STD clinical preventive services.
Methods: We developed an administrative reporting template to determine how the 13.5% funds have been used by awardees in 2014 to support safety net STD clinical preventive services. Using SAS, we analyzed data from all 59 awardees. We collected information on clinical partner types, number of clients served, description of STD tests performed and associated positivity for tests funded by AAPPS.
Results: Based on aggregate data, awardees reported funding or providing in-kind support, such as STD test kits, to a total of 2,854 clinical partner sites. Of those that reported data on billing, 67.9% of their patients aged 16-44 years were uninsured or underinsured. Over 73% of these clinical partner sites were identified as family planning clinics or state or local public STD clinics. Of the AAPPS-supported syphilis (n=160,495), chlamydia (n= 598,623), and gonorrhea (n=573,727) tests performed, 1.2% were positive for newly diagnosed syphilis cases, 11.7% were positive for chlamydia, and 3.7% were positive for gonorrhea.
Conclusion: STD AAPPS funded programs are partnering with clinical providers who are serving uninsured or underinsured patients in the target age range. There is a need to continue support for STD safety-net clinical preventive services for the most vulnerable populations post Affordable Care Act implementation.
Related Content
- STD Prevention Success Stories
- Program Management & Evaluation Tools
- Improving Sexually Transmitted Disease Programs through Assessment, Assurance, Policy Development, and Prevention Strategies (STD AAPPS)
- STD-related Reproductive Health, Prevention, Training, and Technical Assistance Centers (STDRHPTTACs)
- Page last reviewed: September 1, 2016 (archived document)
- Content source: