

NSSP Updates
 ShareCompartir
ShareCompartir
October 2017
OVERALL NSSP UPDATES
Welcome to NSSP Update

NSSP Update is published monthly by the National Syndromic Surveillance Program (NSSP) and brings you the latest news about the BioSense Platform. To learn more, visit the NSSP website. Link to more resources via the Syndromic Surveillance Community of Practice Portal.

On August 25, 2017, Hurricane Harvey hit the gulf coast as a Category 4 storm and then dumped more than a foot of rain on Houston. Roughly two weeks later on Sunday, September 10, 2017, Hurricane Irma ripped through the US Virgin Islands and the Keys before making landfall at Marco Island, then barreling up Florida’s west coast and affecting much of the state. Shortly thereafter on September 20, 2017, Hurricane Maria hit Puerto Rico.
Texas, Florida, and the Commonwealth of Puerto Rico were declared disaster areas. Texas suffered major flooding; scores of areas in Florida lacked electricity, were flooded, and suffered considerable property damage; and Puerto Rico was devastated. A host of disaster relief organizations responded in the aftermath, including the Federal Emergency Management Agency (FEMA) and the U.S. Department of Health and Human Services (HHS) Office of the Assistant Secretary for Preparedness and Response (ASPR). CDC’s NSSP Team also stepped up to provide expertise in syndromic surveillance.
Syndromic surveillance, which is best known for its ability to provide information in nearly real-time, can improve situational awareness. So just how did SyS perform during these response efforts? The syndromic surveillance capacity of the Texas and Florida public health systems is quite different. Did that affect NSSP’s support? Was the NSSP Team able to support all partners’ needs while collaborating with other federal agencies? Here’s a snapshot of the NSSP Team’s experience during the responses.
Initial Deployment of Disaster Medical Assistance Teams
When disaster struck, ASPR deployed Disaster Medical Assistance Teams (DMATs) in Texas to provide critical medical services to people displaced by flooding and storm damage. A DMAT is a team of emergency medicine, primary care, and pediatric physicians assisted by critical care and emergency medical care nurses plus an array of paramedics and various support staff. Teams are organized under the National Disaster Medical System (NDMS) to provide emergency medical care and to augment local medical capabilities during times of disaster in the United States. Electronic Health Record data from deployed DMATs are transmitted to HHS/ASPR’s Office of Emergency Management, which became an information-sharing hub.
NSSP Collaboration with Texas
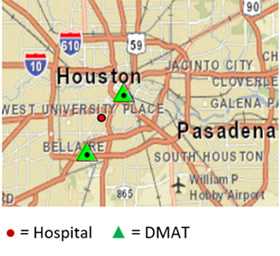
In mid-September, three hospitals in the Houston area were submitting data to the BioSense Platform. Two DMATS were operational.
CDC’s NSSP Team mobilized quickly when Hurricane Harvey struck, engaging with technical staff from HHS/ASPR (see sidebar). First, NSSP sought to better understand the details of the DMAT data so that they could modify the system to support data receipt, data quality assurance, and ingestion into the ESSENCE interface.
The NSSP Team then consulted the ESSENCE developers at Johns Hopkins University Advanced Physics Lab (JHU–APL) about implementing a module previously developed with Florida during the 2012 presidential convention. Given the NSSP Team’s recent and extensive renovation of the BioSense Platform, their previous work with HHS/ASPR technical staff, and solid working relationship with JHU–APL, they were able to rapidly modify system processes and the ESSENCE application. By the time DMATs were deployed to Texas, the BioSense Platform was ready to receive and properly analyze data.
The ASPR DMAT data source is valuable because it can provide a glimpse into public health emergencies occurring on the ground during an event in nearly real time. These data were made available to ASPR, the CDC Emergency Operations Center (CDC EOC), and local partners in the Houston area (Texas Region 6-5). For Texas to take advantage of this valuable new DMAT data source, there is an additional story to tell about site-to-site collaborations and BioSense Platform functionality.
Texas—which includes the Dallas-Fort Worth area (Texas Region 2-3), Texas Region 6-5, and the Texas Department of State Health Services (DSHS)—is in the midst of upgrading and developing statewide syndromic capability. Unfortunately, implementation of a local instance of ESSENCE in Texas Region 6-5 was not complete when Harvey hit. Texas Region 2-3, on the other hand, had both a local instance and could use the BioSense Platform. Texas Region 2-3 receives data from a large hospital chain that also provides data for a few emergency departments (EDs) in Texas Region 6-5. By using the BioSense Platform’s Access & Management Center (AMC), Texas Region 2-3 was able to create users for Texas Region 6-5 (City of Houston and adjacent local jurisdictions) and share the Houston EDs. Once the users and data rules for local EDs were set, NSSP staff could share DMAT data as well.
Thanks to the AMC and a strong partnership with Texas Region 2-3, all users and data sharing rules were in place within about 24 hours. For many participants in this multiagency response, this was their first use of ESSENCE. To familiarize new users with essential components and system functions, the NSSP Team provided just-in-time training, bringing Texas users quickly up to speed on query creation and dashboard sharing to assist with their situational awareness and surveillance efforts. In the days following Harvey, the NSSP Team continued to provide response support to Texas Region 6-5. Further, our Texas partners agreed to allow the NSSP Team to share information and reports about the Houston facilities with CDC EOC epidemiologists and provide important input into the reports CDC EOC shared with other partners (HHS Secretary’s Operations Center [SOC], etc.). This enabled NSSP to ensure situational awareness across different levels of government and assist in guiding any resources that CDC might bring to bear.
NSSP Collaboration with Florida, Georgia, Alabama, South Carolina, North Carolina, US Virgin Islands, and Puerto Rico

By mid-September, 14 DMATs were operational in Florida.
Before NSSP’s response to Harvey had ended, Hurricane Irma, which was rapidly approaching, posed new challenges to the BioSense Platform. For example, the ESSENCE module was not created to support multiple DMAT deployments. Working quickly, the NSSP, JHU–APL, and ASPR teams reconfigured the access control so that ESSENCE could support the need for DMAT data to be controlled by deployment and location. In short order, the system could now support efforts for Hurricane Harvey in Texas and Hurricane Irma in the United States Virgin Islands, Puerto Rico, Florida, Alabama, Georgia, South Carolina, and North Carolina—depending on the storm’s track. Days before Irma hit, the NSSP Team contacted epidemiologists at these locations to discuss what, if any, support they needed from NSSP and to decide what data or reports could be shared with the CDC EOC.
Every site has different experience and capabilities. Florida, having been the original developer of the DMAT module, wanted a DMAT data feed to its local ESSENCE system (FL-ESSENCE) and benefited from the improvements JHU–APL and NSSP had made to how ESSENCE processed the DMAT data. Florida officials determined that its local, more complete system would “own” reporting and identified the reports that Florida’s EOC would share with the CDC EOC. NSSP supplemented Florida’s reports by providing DMAT-related information to the CDC EOC. Working through reporting and data-sharing considerations before the storm hit was imperative.
Georgia, which has a robust syndromic surveillance system, expressed interest in collaborating with NSSP to review data. Similarly, South Carolina and North Carolina were interested in collaborating, but neither state sustained the same level of damage from Hurricane Irma. Alabama, however, suffered storm damage and became one of many locations for evacuees from Florida. Because Alabama does not have a local syndromic surveillance system, the state asked NSSP to assist by developing BioSense Platform queries and dashboards similar to what Texas Region 6-5 had used. In all instances, the NSSP Team adjusted and performed as asked.
In the end, syndromic surveillance helped provide key situational awareness information to NSSP’s response partners at local, state, and federal levels. Information sharing occurred differently across state and local governments depending on availability of staff and resources and on prior experience with hurricanes and the BioSense Platform. All agencies worked well together due largely to good communication with respect to data sharing and the technical capabilities of the BioSense Platform’s AMC and ESSENCE, which facilitated much of the activity.
The BioSense Platform’s design and flexibility withstood Hurricanes Harvey’s and Irma’s tests—and the Platform’s power met local needs. Today, hurricane surveillance operations are supporting the US Virgin Islands and Puerto Rico response to Hurricane Maria. The flexibility, skills, and communications across all teams (NSSP, ASPR, local and state health departments, and JHU–APL) were remarkable and show what can be achieved when our Community of Practice is in need and collaborates during situations like these. This first dramatic test of both the Community of Practice and BioSense Platform abilities since going live in December 2016 demonstrates the value of our work in developing the NSSP, its BioSense Platform, and the Community of Practice.

Resources
Mosquitoes and Hurricanes
Be Safe After a Hurricane
Be Ready! Hurricanes Infographic
Carbon Monoxide (CO) Poisoning Prevention

The Department of Health and Human Services (HHS) Office of the Assistant Secretary for Preparedness and Response (ASPR) is a leader in preparing the nation and its communities to respond to and recover from public health and medical disasters and emergencies.
ASPR focuses on preparedness planning and response; building federal emergency medical operational capabilities; countermeasures research, advanced development, and procurement; and grants to strengthen the capabilities of hospitals and health care systems to minimize the health impacts of disasters and public health emergencies. The office provides federal support, including medical professionals through the National Disaster Medical System, to augment state and local capabilities during an emergency or disaster (ASPR fact sheet).
ASPR coordinates with the Centers for Disease Control and Prevention (CDC) on the development of federal response plans, policy, guidance, and communication, and development of clinical utilization and allocation strategies as appropriate for medical countermeasures and assets.
ASPR and CDC also coordinate interactions with state, local, tribal, territorial, and private entities to provide timely and effective deployment, distribution, dispensing, and administration of medical countermeasures in an emergency.
This information is provided by the U.S. Department of Health & Human Services, Office of the Assistant Secretary for Preparedness and Response. For more information, visit the website.
NSSP Progress Toward Transitioning Legacy Data
The NSSP Team continues to move data from the legacy system to ESSENCE. We made a notable accomplishment in the number of sites migrated to ESSENCE last month. By mid-September, we had processed 16 sites into production ESSENCE. At least 5 sites had data ready to load into ESSENCE. Of the remaining 20 sites, 9 are reviewing their data in the staging environment.
Thanks for your continued patience throughout the legacy transition. If you have specific questions about your site, please contact the NSSP Service Desk.

New, Single Sign-on to BioSense Platform
In early September, we had planned to update the Access & Management Center (AMC) and integrate it with the BioSense Platform’s active directory to make passwords easier to manage. This update was delayed because BioSense Platform data were being used to support critical surveillance related to Hurricanes Harvey and Irma.
The update is being deployed early this month, making the AMC the central point for password management. Now, all BioSense Platform users will have a single username and password for all applications and analysis tools. If you have questions, please contact the NSSP Service Desk.
Update: Refinement of Calculated Patient Class Algorithm
In the August issue of NSSP Update, we described some changes we’re making to the C_Patient_Class field. This field stores the “best available” Patient Class found in incoming messages. Calculated Patient Class data were intended to have pristine Patient Class data. Such data can facilitate queries and be used to create binary flags in ESSENCE that indicate if the visit was “ever in a specific Patient Class.” For example, a flag can indicate if the Patient Class history has “E” somewhere in the history. Binary flags can certainly improve query performance—but only if data are pristine. The updates we’re making to the NSSP Calculated Patient Class definition align with the original intent of having pristine data.
During September, we updated the retrospective data in the NSSP Archive, which is the processed table. Next, we’ll apply this update to existing data in ESSENCE. Then we’ll introduce the “ever in” flags that will be part of the updated definition (see details in August issue).
If you have questions, the NSSP Analytic Data Management Team will be pleased to explain how these changes affect your data. Simply submit a Support Request to the NSSP Service Desk.
NSSP ESSENCE Adds Category for Querying Influenza-like Illness
Influenza season is just around the corner. Influenza-like illness (ILI) is one of the more commonly used syndromes in syndromic surveillance practice. Although ESSENCE already has a few syndromes and sub-syndromes that capture ILI, these use only the chief complaint text. The new keyword-based category uses chief complaint text and discharge diagnoses (ICD-9, ICD-10, and SNOMED codes) to try to improve upon the existing syndromes. We are calling this “ILI CCDD v1.” We plan to update the query once we hear from you and can assess how well it is working.
The query terms as ESSENCE syntax are shown below:
| Category | Query Terms (ESSENCE Syntax) |
|---|---|
| Chief Complaint and Discharge Diagnosis | (,^fever^,andnot,^denies fev^,andnot,^shot^,andnot,^afeb^,andnot,^no fev^,andnot,^no temp^,or,^chill^,or,^pyrexia^,or,^ febrile^,or,^high temp^,or,^elevated temp^,andnot,^denies any elevated temp^,andnot,^no elevated temp^,or,^feeling hot^,or,^feels hot^,or,^fvr^,andnot,^denies fvr^,andnot,^no fvr^,),and,(,^cough^,andnot,^denies cough^,or,^sore ^th[o|r][a|o][a|r]t^,or,^soreth[o|r][a|o][a|r]t^,or,^strep^,or,^pharyn^,or,^upper resp^,),or,(,^[;/ ]J09^,or,^[;/ ]J10^,or,^[;/ ]J11^,or,^[;/ ]487.[018];^,or,^[;/ ]487[018];^,or,^[;/ ]487.[018],or,^[;/ ]487[018],or,^[;/ ]488.[018][19];^,or,^[;/ ]488[018][19];^,or,^[;/ ]488.[018][19],or,^[;/ ]488[018][19],or,^442696006^,or,^442438000^,or,^6142004^,or,^195878008^,or,^influenza^,andnot, ^vaccin^,andnot,^shot^,andnot,^immunizat^,or,^ flu ^ ,andnot,^shot^,andnot,^stomach^,andnot,^vaccin^,andnot,^immuniza^,or,^flu like^,or,^flulike^,or,^flu symptom^,),andnot,^[;/ ]A08.4^,andnot,^[;/ ]A084^ |
You can find the CC and DD category by clicking on the ESSENCE Query Portal, then scrolling the left pane until you find the CC and DD category in the list of Available Query Fields. Select CC and DD category to view available categories in the central pane of the Query Wizard. Simply select ILI CCDD v1 from the list to use it in your query.
Look for more work in this area. We plan to publish the most popular free-text queries as CC and DD categories soon.
CDC Resources:
CDC guidance for the 2017–2018 influenza season
CDC Influenza (Flu) website
Communication Resources—Free, downloadable communication and education materials to assist public health departments in flu prevention.
SPOTLIGHT ON SYNDROMIC SURVEILLANCE PRACTICE
We continue our series of articles examining literature that advances the practice of syndromic surveillance. This month, we feature an article about six use cases that demonstrate the value of syndromic surveillance. These diverse cases and approaches have practical application for local and state health departments.
Advancing the Use of Emergency Department Syndromic Surveillance Data,
New York City, 2012–2016
Use Case Resources
Syndromic Surveillance Use Cases
Site is for users with all levels of experience and encourages information sharing.
Community of Practice Use Case Library
Administered by the International Society for Disease Surveillance (ISDS).
New York City collects syndromic surveillance (SyS) data from all city hospital emergency departments. Through the years, New York’s use of data has broaden considerably to include surveillance of noninfectious disease syndromes and situational awareness. Sometimes, especially early in a health-related event, SyS is the only available data source. Often, it’s the only near real-time data source and is therefore used in tandem with other reporting systems. This article presents six diverse use cases in which SyS has been used in both ways to inform decision making in New York City and prompt public health officials to take action.
Advancing the Use of Emergency Department Syndromic Surveillance Data, New York City, 2012–2016 is part of a supplemental issue of Public Health Reports.2 The six use cases are synthetic cannabinoid drug use, heat-related illness, suspected meningococcal disease, medical needs after severe weather, asthma exacerbation after a building collapse, and Ebola-like illness in travelers returning from West Africa.1
The syndromes described use specific terms and involve few cases per day. The syndrome definitions for each use case have well-defined, targeted surveillance objectives (specificity, sensitivity) and methods for analysis that vary depending on the surveillance objectives. In all the use cases described, the analysts needed knowledge of the disease or condition. The authors summarize each use case under Results. This collection of use cases not only shares syndrome definitions, it shares statistical methods, and other information that led public health practitioners to take action, bolstering the case for making SyS part of any public health department’s comprehensive surveillance program.
NSSP commends the authors for sharing this collection of use cases and for encouraging others to do likewise by publishing their methods and lessons learned. The authors have developed a prototype website that serves as a model for documenting similar use cases. Efforts such as this article and website help the SyS community build capacity for all-hazards preparedness.
1 Lall R, Abdelnabi J, Ngai S, Parton HB, Saunders K, Sell J, Wahnich A, Weiss D, Mathes RW. Advancing the Use of Emergency Department Syndromic Surveillance Data, New York City, 2012–2016. Public Health Reports [Internet]. 2017 July/August [cited 2017 Sep 18];132(1 Suppl):23S–30S. Available from: http://journals.sagepub.com/doi/full/10.1177/0033354917711183
2 Syndromic Surveillance: The Value of Real-time Data for Public Health Action. Public Health Reports [Internet]. 2017 July/August [cited 2017 Jul 25];132(1 Suppl). Available from: http://journals.sagepub.com/toc/phrg/132/1_suppl
UPCOMING EVENTS

| October 3, 2017 | Access & Management Center Active Directory Deployment |
| October 4, 2017 | Data Validation Support Call: 3:00–4:00 PM ET |
| October 17, 2017 | Scheduled vendor patches in staging environment: 6:00–10:00 AM ET |
| October 19, 2017 | Scheduled vendor patches in production environment: 6:00–10:00 AM ET |
| September 26, 2017 | Surveillance Community of Practice Call: 3:00–4:30 PM ET. The topic is Syndromic Surveillance Data Briefs. |
| October 24, 2017 | Surveillance Community of Practice Call: 3:00–4:30 PM ET. The topic is “What is a Chapter?” Reps from regional chapters will discuss their initial formation, activities, and challenges. |
| January 30–February 2, 2018 | ISDS 2018 Annual Conference. Global Health Today and Tomorrow: Policy Options and Scientific Solutions |
| February 27–March 1, 2018 | NSSP 2018 Annual Recipient Meeting (formerly the Grantee Meeting); Atlanta, Georgia. Planning is underway and details will follow. |
Note: To access the Surveillance Community of Practice group resources, you must be signed in to your healthsurveillance.org account. To create an account, click here.
LAST MONTH’S TECHNICAL ASSISTANCE UPDATES
| September 6, 2017 | Data Validation Support Call |
| September 19, 2017 | Scheduled vendor patches in staging environment |
| September 19, 2017 | “Next Steps” call for sites interested in onboarding to the BioSense Platform |
| September 21, 2017 | Scheduled vendor patches in production environment |
NSSP PARTICIPATION
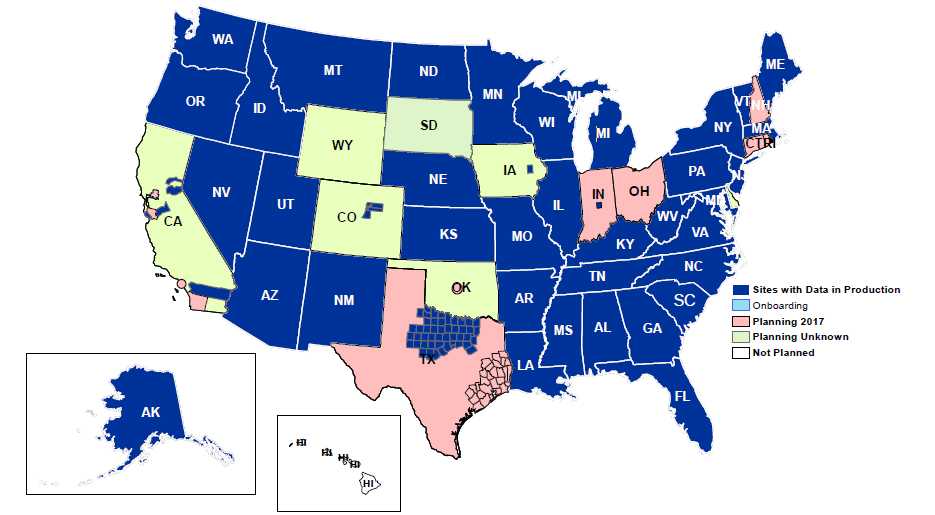
NSSP receives data from more than 4,000 facilities. Of these, 2,086 are emergency departments (EDs) that actively submit data, which means that about 60% of all ED visits in the country are being represented (based on American Hospital Association data). At the end of August 2017, 49 sites in 41 states were participating in NSSP. Although NSSP is pleased with participation to date, sites with data in production do not always translate into sites with broad ED coverage. NSSP continues to work closely with sites to improve data representativeness.
Definitions: NSSP consolidates facilities that provide data under a single data administrative authority called a site administrator. These facilities and single-site administrator constitute a site.
ONBOARDING UPDATES

Fall Onboarding is Underway!
Onboarding will begin October 3, 2017, and continue through December 15, 2017. NSSP held a “next steps” call for participants from 15 interested sites on September 19, 2017, to assess onboarding readiness. Once participants commit, onboarding will kick off with a webinar that introduces connectivity, Master Facility Table, Adminer, and NSSP Service Desk. The NSSP Onboarding Team will also conduct weekly calls to assist site participants who are onboarding. The next window for onboarding will be spring 2018.
Data Validation Support
Conference calls are held the first Wednesday of each month, 3:00–4:00 PM ET, to assist with data validation compliance. For more information, contact the NSSP Service Desk.
GRANTEES AND PARTNERSHIPS UPDATES

Plans Underway for 2018 Annual Recipient Meeting
We’re pleased to announce that planning for our third annual meeting (formerly the Grantee Meeting) is underway. This year’s meeting is scheduled for February 27–March 1, 2018. Once again, the meeting will be held in Atlanta, Georgia, where you’ll have an opportunity to meet the NSSP Team and other public health practitioners who participate in the NSSP.The NSSP project officers sent a draft agenda to recipients of NSSP Enhancing Syndromic Surveillance Capacity and Practice funding, CDC-RFA-OE15-1502. It is our hope that recipients will take a few minutes to review the agenda and submit input to their project officers by November 10, 2017. More details, including registration and hotel information, will be available soon. We look forward to having a successful 2018 Annual Recipient Meeting.
South Region—Kim Raymond, Project Officer
Louisiana Site Visit

In September 2017, Project Officers Kim Raymond and Antheny Wilson met with staff from the Louisiana Department of Health (LDH), Office of Public Health (OPH), Infectious Disease Epidemiology Section (IDEpi). They reviewed challenges, opportunities, and progress toward program goals.
Louisiana operates its own surveillance system, the Louisiana Early Event Detection System (LEEDS), which sends syndromic surveillance (SyS) data to the NSSP BioSense Platform. With 113 emergency departments in Louisiana, NSSP funding has allowed IDEpi to stabilize LEEDS and increase hospital data submissions from 21 to 108, with 71 hospitals submitting data to production and 37 submitting data to test.
Currently, IDEpi submits SyS data from 61 hospitals to the BioSense Platform, with plans to eventually submit all hospital data. Of these 61 hospitals, 84% of the records are available in the BioSense Platform within 48 hours of patient encounter, and 91% of the records are submitted to LEEDS within 24 hours of the date and time of visit.
The use of LEEDS’ syndromic surveillance data has helped IDEpi’s partner agencies—the Office of Behavioral Health and the Bureau of Health Informatics—secure grants for work involving prescription drug overdose and the opioid crisis. Louisiana continues to increase its data quality reviews, do daily data analysis, respond to technical issues, and provide timely situational awareness and response. Louisiana’s SyS program is making considerable strides forward. And for that, we say great work, Louisiana!
Please share your successes for improving data representativeness; data quality, timeliness, and utility; SyS practice; and the use of SyS data for public health action and response. Simply fill out the NSSP Success Stories Template and email to us.
COMMUNITY OF PRACTICE UPDATES

Hurricane season is upon us and the Community of Practice is sharing resources related to Hurricane and Disaster surveillance in the Surveillance Knowledge Repository.
Work Group and Committee Updates
- The Metadata Visualization Application (MVA) Workgroup and NSSP Team have begun adding vendor information to the interactive web MVA. The process begins by creating a standard vendor mapping guide to ensure uniformity before adding the vendor data to the application. Next, personnel from different public health jurisdictions will help validate the guide by reviewing their vendor data post-mapping. Once the mapping is complete, this new variable will be added to the MVA so that personnel from different public health jurisdictions can see which vendors their colleagues have been working with.
- The Urgent Care Justification Workgroup was formed to gather information about urgent care surveillance, justify why these data are needed, and create an abstract for the 2018 International Society for Disease Surveillance (ISDS) Conference. The workgroup is finalizing the Urgent Care Justification abstract and plans to follow-up by creating three support documents. Follow the workgroup’s progress on the Urgent Care Justification Workgroup page (be sure to log in first). Participate in monthly calls, or listen to stay informed on this evolving topic. Meetings are held the second Tuesday of each month, 12:30–1:30 PM ET.
- The Data Quality Committee (DQC) hosted its first open quarterly call in September. This new, open-call format allows the committee to invite additional stakeholders to the discussion each quarter while maintaining the closed, group-only calls that are standard DQC practice. This month, the DQC hosted two representatives from Cerner Corporation: Courtney Fitzgerald and Kirsten Hagemann, who presented on the roll-out of Cerner’s new solution for syndromic surveillance reporting. Call participants were able to ask about it and other Cerner products. The DQC would like to thank Courtney and Kirsten for their time, expertise, and willingness to make themselves available to the syndromic community.
Interested in joining a chapter, committee, or work group? You can find a list of the groups here.
Messaging Guide
The Messaging Guide Workgroup continues to meet regularly to review comments on version 2.2 of the Messaging Guide for Syndromic Surveillance. Currently, the workgroup has reviewed more than half of the submitted comments on subjects including patient name, race, diagnosis concerns, ICD-9 versus ICD-10, OBX concerns including travel and pregnancy status, and PV1 concerns. The Messaging Guide Workgroup met throughout September to reconcile comments and prepare the next version of the guide for the community’s review. If you are interested in joining the Messaging Guide Workgroup, visit the Messaging Guide Workgroup page to access the working documents and call-in information.
Development of Messaging Guide for Syndromic Surveillance*
| Time Frame | Activity |
|---|---|
| 2015 | Version 2.0 Released |
| 2016 | Erratum and Clarification Document Released for Version 2.0 |
| 2017 Spring | Version 2.2 Released for Community Comment and Consensus |
| 2017 Summer | Version 2.3 to be Released for Review |
| 2017 Fall | Version 2.4 to be Prepared for HL7 Balloting |
| 2017 Winter | Version 2.5 HL7 Balloting Begins |
| 2018 January | HL7 Balloting (anticipated) Completed—Version 2.6 Released |
* This document was previously titled Public Health Information Network (PHIN) Messaging Guide for Syndromic Surveillance.
Community of Practice Call
Please join the monthly Surveillance Community of Practice Call. The purpose of this call is to bring together stakeholders with a vested interest in surveillance and to spark collaborative efforts to share guidance, resources, and technical assistance.
The next call will be held October 24, 2017, 3:00–4:30 PM ET and is titled “What is a Chapter?” Join us to hear from our regional Chapters about their initial formation, activities, and challenges. Click here to register.
Note: Please remember that you have to register for each call individually. To access the slides and recordings from previous Surveillance CoP Calls, visit the Surveillance Community of Practice Group Page. You must be signed into your healthsurveillance.org account. To create an account on healthsurveillance.org, click here.
- Page last reviewed: October 6, 2017
- Page last updated: October 6, 2017
- Content source: