Fontan procedure
The Fontan procedure or Fontan–Kreutzer procedure is a palliative surgical procedure used in children with univentricular hearts. It involves diverting the venous blood from the inferior vena cava (IVC) and superior vena cava (SVC) to the pulmonary arteries without passing through the morphologic right ventricle; i.e., the systemic and pulmonary circulations are placed in series with the functional single ventricle. The procedure was initially performed 1968 by Francis Fontan and Eugene Baudet, and further described in 1973 by Guillermo Kreutzer.
| Fontan or Fontan–Kreutzer procedure | |
|---|---|
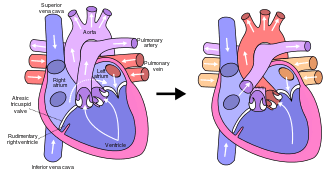 Fontan procedure for tricuspid atresia | |
| ICD-10-PCS | Z98.890 |
| ICD-9-CM | 35.94 |
| MeSH | D018729 |
Indications
The Fontan procedure is used in pediatric patients who possess only a single functional ventricle, either due to lack of a heart valve (e.g. tricuspid or mitral atresia), an abnormality of the pumping ability of the heart (e.g. hypoplastic left heart syndrome or hypoplastic right heart syndrome), or a complex congenital heart disease where a bi-ventricular repair is impossible or inadvisable. The single ventricle is doing nearly twice the expected amount of work because it has to pump blood for the body and lungs. Patients typically present as neonates with cyanosis or congestive heart failure.[1] Fontan completion is usually carried out when the patient is 2–5 years of age, but is also performed before 2 years of age.[2][3]
Contraindications
After Fontan completion, blood must flow through the lungs without being pumped by the heart. Therefore, children with high pulmonary vascular resistance may not tolerate a Fontan procedure. Often, cardiac catheterization is performed to check the resistance before proceeding with the surgery. This is also the reason a Fontan procedure cannot be done immediately after birth; the pulmonary vascular resistance is high in utero and takes months to drop. Fontan procedure is also contraindicated in those with pulmonary artery hypoplasia, patients with left ventricular dysfunction and significant mitral insufficiency.
Types
There are four variations of the Fontan procedure:[4]
- Ventricularization of the Right Atrium (The original Fontan's Technique)
- Atriopulmonary connection (the original Kreutzer's Technique)
- Intracardiac total cavopulmonary connection (lateral tunnel)
- Extracardiac total cavopulmonary connection
Approach

The Fontan is usually done as a two staged repair.
The first stage, also called a Bidirectional Glenn procedure or Hemi-Fontan (see also Kawashima procedure), involves redirecting oxygen-poor blood from the top of the body to the lungs. That is, the pulmonary arteries are disconnected from their existing blood supply (e.g. a shunt created during a Norwood procedure, a patent ductus arteriosus, etc.). The superior vena cava (SVC), which carries blood returning from the upper body, is disconnected from the heart and instead redirected into the pulmonary arteries. The inferior vena cava (IVC), which carries blood returning from the lower body, continues to connect to the heart.
The second stage, also called Fontan completion, involves redirecting the blood from the IVC to the lungs. At this point, the oxygen-poor blood from upper and lower body flows through the lungs without being pumped (driven only by the pressure that builds up in the veins). This corrects the hypoxia and leaves the single ventricle responsible only for supplying blood to the body.
Post-operative complications
In the short term, children can have trouble with pleural effusions (fluid building up around the lungs). This can require a longer stay in the hospital for drainage with chest tubes. To address this risk, some surgeons make a fenestration from the venous circulation into the atrium. When the pressure in the veins is high, some of the oxygen-poor blood can escape through the fenestration to relieve the pressure. However, this results in hypoxia, so the fenestration may eventually need to be closed by an interventional cardiologist.
In a 2016 review, Dr. Jack Rychik, head of the Single Ventricle Survivorship Program at Children's Hospital of Philadelphia summarized the long-term consequences of Fontan circulation as an "indolent and progressive state of heart failure" with predictable long term consequences on several organ systems.[5] Chronic venous hypertension and lowered cardiac output are assumed to be at the root of lymphatic complications such as chylothorax, protein losing enteropathy and plastic bronchitis which may occur in the immediate post-operative period as well as in the medium term. Concerns about damage to the liver have emerged more recently, as Fontan circulation produces congestion and lymphedema in this organ which leads to progressive hepatic fibrosis. Screening protocols and treatment standards are emerging in the light of these discoveries.[5]
The Fontan procedure is palliative — not curative — but in many cases it can result in normal or near-normal growth, development, exercise tolerance, and good quality of life.[6] However, in 20–30% of cases, patients will eventually require heart transplantation[7] and given the long-term consequences of chronic venous hypertension and insidious organ damage, freedom from morbidity is unlikely in the long term.
History

The Fontan procedure was initially described in 1971 by Dr. Francis Fontan (1929–2018) from Bordeaux, France. Prior to this, the surgical treatment for tricuspid atresia consisted of creating a shunt between a systemic arteryand the pulmonary artery (Blalock-Taussig shunt) or the superior vena cava and the pulmonary artery (Glenn shunt). These procedures were associated with high mortality rates, commonly leading to death before the age of one year.[8] In an attempt to improve this, Fontan was engaged in research between 1964 and 1966 endeavouring to fully redirect flow from the superior and inferior vena cavae to the pulmonary artery.[9] His initial attempts in dogs were unsuccessful and all experimental animals died within a few hours; however, despite these failures, he successfully performed this operation in a young woman with tricuspid atresia in 1968 with Dr Eugene Baudet.[8] The operation was completed on a second patient in 1970, and after a third case the series was published in the international journal Thorax in 1971. [10] Dr. Guillermo Kreutzer from Buenos Aires, Argentina (b. 1934) performed a similar procedure in 1973. [11][8]
References
- O'Leary PW. (2002). "Prevalence, clinical presentation and natural history of patients with single ventricle". Progress in Pediatric Cardiology. 16: 31–38. doi:10.1016/s1058-9813(02)00042-5.
- Hirsch JC, Goldberg C, Bove EL, et al. (2008). "Fontan operation in the current era: a 15-year single institution experience". Annals of Surgery. 248 (3): 402–410. doi:10.1097/SLA.0b013e3181858286. PMID 18791360.
- Anderson PA, Sleeper LA, Mahony L, et al. (2008). "Contemporary outcomes after the Fontan procedure: A Pediatric Heart Network multicenter study". Journal of the American College of Cardiology. 52 (2): 85–93. doi:10.1016/j.jacc.2008.01.074. PMC 4385517. PMID 18598886.
- Leval, Marc R de (2005). "The Fontan circulation: a challenge to William Harvey?". Nature Clinical Practice Cardiovascular Medicine. 2 (4): 202–208. doi:10.1038/ncpcardio0157. PMID 16265484.
- Rychik, Jack (2016). "Relentless Effects of the Fontan Paradox". Seminars in Thoracic and Cardiovascular Surgery. 19 (1): 37–43. doi:10.1053/j.pcsu.2015.11.006. PMID 27060041.
- Mair DD, Puga FJ, Danielson GK (November 1992). "Late functional status of survivors of the Fontan procedure performed during the 1970s". Circulation. 86 (5 Suppl): II106–9. PMID 1423987.
- Behrman, Richard E.; Robert M. Kliegman; Hal B. Jenson (2004). Nelson Textbook of Pediatrics (17th ed.). Saunders. ISBN 978-0-7216-9556-3.
- Cowgill, L. D. (June 1991). "The Fontan procedure: a historical review". The Annals of Thoracic Surgery. 51 (6): 1026–1030. doi:10.1016/0003-4975(91)91044-v. ISSN 0003-4975. PMID 2039305.
- Anderson, R. H. (November 1999). "Francis Fontan". Cardiology in the Young. 9 (6): 592–600. doi:10.1017/s1047951100005631. ISSN 1047-9511. PMID 10593269.
- Fontan F, Baudet E (1971). "Surgical repair of tricuspid atresia". Thorax. 26 (3): 240–248. doi:10.1136/thx.26.3.240. PMC 1019078. PMID 5089489.
- Kreutzer G, Galindez H, Bono H (1973). "An operation for the correction of tricuspid atresia". The Journal of Thoracic and Cardiovascular Surgery. 66 (3): 613–621. PMID 4518787.
External links

- Overview of single ventricle lesions from Cincinnati Children's Heart Center