We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Takotsubo cardiomyopathy
From WikEM
Contents
Background
- AKA transient apical ballooning syndrome or stress-induced cardiomyopathy
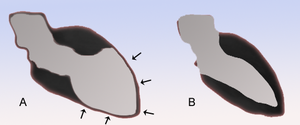
- Bulging out of LV apex with preserved function of the base looks like an octopus pot or "tako tsubo" in Japanese
- 85% of cases caused by stressful event before symptoms (death of loved one, fear, argument, asthma, surgery, stroke, etc.)[1]
- Proposed mechanisms include vasospasm and abnormal response to catecholamine surge
- As high as 28% in ICU patients due to severe physical stress[2]
Clinical Features
- Mimics Acute Coronary Syndrome
- Chest Pain
- Dyspnea
- Cardiogenic Shock and sudden CHF
- Lethal arrhythmia (e.g. VT/VF, PEA)
Differential Diagnosis
ST Elevation
- Myocardial infarct (STEMI)
- Post-MI (ventricular aneurysm pattern)
- Previous MI with recurrent ischemia in same area
- Wellens' syndrome
- Coronary artery vasospasm (eg, Prinzmetal's angina)
- Coronary artery dissection
- Drugs of abuse (eg, cocaine, crack, meth)
- Pericarditis
- Myocarditis
- Aortic dissection in to coronary
- LV aneurysm
- Early repolarization
- Left bundle branch block
- Left ventricular hypertrophy (LVH)
- Pneumomediastinum
- Pneumothorax
- Pulmonary Embolism
- Myocardial tumor
- Myocardial trauma
- External compression of artery
- Medications: Tricyclic (TCA) toxicity, Digoxin
- RV pacing (appears as Left bundle branch block)
- Hyperkalemia (only leads V1 and V2)
- Hypothermia ("Osborn J waves")
- Brugada syndrome
- Takotsubo cardiomyopathy
- AVR ST elevation
Cardiomyopathy
- Dilated cardiomyopathy
- Hypertrophic cardiomyopathy
- Restrictive cardiomyopathy
- Peripartum cardiomyopathy
- Takotsubo cardiomyopathy
- Arrhythmogenic right ventricular dysplasia
Evaluation

- Troponin frequently elevated
- ECG
- May mimic STEMI
- Frequently affects the anterior distribution and to a lesser extent inferior distribution
- Echocardiogram
- Systolic Dysfunction (with ejection fraction dropping from normal to <25-35%)
- Reduced contractility not explained by single vessel disease
- Ventriculography
- Shows LV ballooning
- Angiogram
- No significant coronary blockage to explain LV dysfunction
Clinical Differences Between AMI and [3]
| AMI | Takutsubo | |
| ECG | Specific vascular distribution | Multiple regions of change |
| Echo | Specific vascular distribution | Multiple regions of wall motion abnormalities |
| Troponin | Significant elevation | Mild to no elevation |
| NT proBNP | Mild elevation | Significant elevation |
| RV | Uncommon in left heart AMI | ~1/3 have biventricular ballooning |
| Hypotension | Cardiogenic shock | Multi-factorial: LVOT obstruction, peripheral vasodilation, LV and/or RV decreased inotropy |
| PCI | Stenosis | No coronary obstruction |
Management
- Treat as STEMI until ruled out
- Anticoagulation may be required until wall motion abnormalities resolve
- Monitor QTc intervals and arrhythmias
- Stop all QT prolonging drugs
- Replace magnesium levels
- Management of differs from usual cardiogenic shock[4]
- IVF
- With LVOT obstruction, avoid volume depletion and vasodilator therapy (similar to hypertrophic cardiomyopathy management)
- Avoid use of catecholamine based inotropic meds
- Consider Beta Blockers and ACE Inhibitors, which reduce recurrence
- Intra-aortic balloon pump or ECMO in refractory cases
Prognosis
Ejection Fraction returns to normal (at least >50%) in nearly all cases
Disposition
- Admit for post catheterization care
See Also
External Links
References
- ↑ Sharkey, S., Lesser, J., & Maron, B. (2011). Takotsubo (stress) cardiomyopathy. American Heart Association.
- ↑ Park JH, Kang SJ, Song JK, et al. Left ventricular apical ballooning due to severe physical stress in patients admitted to the medical ICU. Chest 2005;128:296-302.
- ↑ TakotsuboMasoud H. Takotsubo Cardiomyopathy in Intensive Care Unit: Prevention, Diagnosis and Management. International Cardiovascular Forum Journal. 2016; 5:33-35.
- ↑ Masoud H. Takotsubo Cardiomyopathy in Intensive Care Unit: Prevention, Diagnosis and Management. International Cardiovascular Forum Journal. 2016; 5:33-35.