We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Pericarditis
From WikEM
Contents
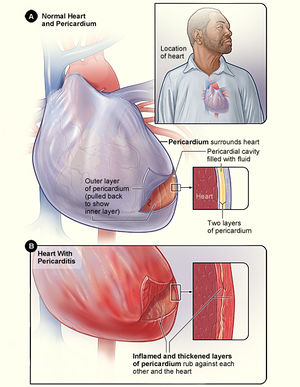
Background
Etiology
- Idiopathic (25-85%)
- Infection (up to 20%, including viral, bacterial, TB)
- Malignancy: heme, lung, breast
- Uremia
- Post radiation
- Connective tissue disease
- Drugs: procainamide, hydralazine, methyldopa, anticoagulants
- Cardiac injury (can see up to weeks later): post MI (Dressler's syndrome), thoracic trauma, aortic dissection
- Troponin elevation may indicate a concurrent myocarditis which predispose to risk of CHF or arrhythmia. [1]
Clinical Features
- Pleuritic chest pain
- Radiates to chest, back, left trapezius
- Diminishes with sitting up/leaning forward
- Shortness of breath
- Especiallyif concommitant pleural effusion
- Hypotension/extremis if cardiac tamponade
- Fever, chills, myalgias (systemic signs with viral infection)
- Friction rub
Differential Diagnosis
ST Elevation
- Myocardial infarct (STEMI)
- Post-MI (ventricular aneurysm pattern)
- Previous MI with recurrent ischemia in same area
- Wellens' syndrome
- Coronary artery vasospasm (eg, Prinzmetal's angina)
- Coronary artery dissection
- Drugs of abuse (eg, cocaine, crack, meth)
- Pericarditis
- Myocarditis
- Aortic dissection in to coronary
- LV aneurysm
- Early repolarization
- Left bundle branch block
- Left ventricular hypertrophy (LVH)
- Pneumomediastinum
- Pneumothorax
- Pulmonary Embolism
- Myocardial tumor
- Myocardial trauma
- External compression of artery
- Medications: Tricyclic (TCA) toxicity, Digoxin
- RV pacing (appears as Left bundle branch block)
- Hyperkalemia (only leads V1 and V2)
- Hypothermia ("Osborn J waves")
- Brugada syndrome
- Takotsubo cardiomyopathy
- AVR ST elevation
Evaluation
Diagnostic Criteria for Acute Pericarditis[2]
- Need 2 of the following
- Chest pain (typically sharp and pleuritic, improved by sitting up and leaning forward)
- Pericardial friction rub
- New or worsening pericardial effusion
- Suggestive ECG changes
Work-Up
- ECG
- Labs
- WBC, CMP, ESR, CRP, trop
- Consider TSH, ANA based on clinical suspicion
- CXR
- Bedside Ultrasound to rule out effusion
- ~2/3 of cases will have pericardial effusion[3]
- Can consider CT or cardiac MRI if workup non-diagnostic and clinical suspicion persists
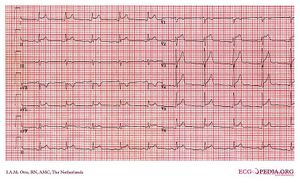
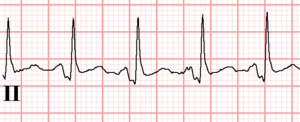
ECG
Classical Teachings with Caveats Below
- Must differentiate from STEMI (classical teachings are not specific enough to do that)
- Classically pericarditis has diffuse ST-elevations
- However, pericarditis may generate localized ST-elevations
- Pericarditis should never produce ST-depressions (suggestive of reciprocal changes), except in V1 and aVR
- Classically pericardidits has concave upwards STE
- Classically pericardititis has PR-depression in viral pericarditis (or PR-elevation in AVR)
- Less reliable in post-MI patients and those with baseline ECG abnormalities
- PR-depression is often early and transient in pericarditis
- In STEMI, PR-depression is associated with atrial injury, though usually not as marked as in viral pericarditis[4]
- PR-elevation in aVR may also be present in STEMI and is infrequently seen in constrictive pericarditis
Other Findings
- Leads II and III
- STE II > STE III favors pericarditis
- STE III > STE II very strongly favors STEMI
- STD not in aVR or V1 (reciprocol changes) suggestive of STEMI
- May see low voltage/alternans if effusion present
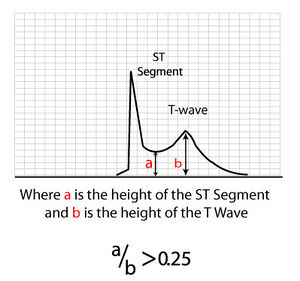
- If early repolarization confounding interpretation check ST:T ratio
- If (STE)/(T height) in V6 or I > 0.25, then it is likely pericarditis
- If predominantly inferior STE, ST-depression in aVL is sensitive for STEMI[5]
- Spodick's sign, purportedly in ~80% - downsloping TP segment, often best seen in lead II and lateral precordial leads[6]

Stages of Progression
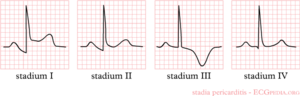
- Stage I:
- Global concave up ST elevation in all leads (esp V4-6, I, II) in all leads except in aVR, V1 and III
- PTa depression (depression between the end of the P-wave and the beginning of the QRS- complex)
- Stage II:
- "pseudonormalisation," ST to baseline, big T's, PR dep
- Stage III:
- T wave flatten then inversion
- Stage IV:
- Return to baseline
STEMI vs Pericarditis
| Disease | STEMI | Pericarditis |
| Pain | Costant | Varies with motion |
| Fever | No | Yes |
| ST changes | focal | Diffuse elevation |
| Reciprocal changes | Yes | No |
| Q waves | Yes | No |
| Pulmonary edema | Sometimes | No |
| Wall motion | Abnormal | Normal |
Management
Initial Treatment
- NSAIDS or Aspirin (ASA)first line treatment (in absence of contraindications) for viral or idiopathic pericarditis.[7]
- Cholchicine add cholchicine to NSAIDs as first line treatment for viral/idiopathic acute and recurrent pericarditis to improve remission rates and prevent recurrence.[8]
- Patients >70kg - 0.6mg PO BID x 3 months
- Patients<70kg - 0.6mg PO Daily x 3 months
- Glucocorticoid therapy second line agent for viral/idiopathic pericarditis, can consider low-moderate doses for patients with contraindications to NSAIDs or persistent symptoms despite appropriate therapy with NSAIDs + colchicine for at least 1 week. Also used for etiologies that are steroid responsive diseases.
- Prednisone 0.2 to 0.5mg/kg of body weight per day for 2 weeks with gradual tapering[9]
Recurrent or Refractory
For recurrent or refractory cases consider colchicine and or steroids although literature suggests it can be used as first line[10]
- Colchicine
- Patients >70kg - 0.6mg PO BID x 6 months
- Patients<70kg - 0.6mg PO Daily x 6 months
- If patients develop serious diarrhea decrease their dosing to the next weight class or stop treatment.
Contraindications to Colchicine[11]
- Tuberculous
- Neoplastic pericarditis
- Liver disease or aminotransferase levels ≥1.5x upper limits of normal
- Creatinine >2.5mg/dL (>221 umol/L)
- Myopathy or CK > upper limits of normal
- Inflammatory bowel disease
- Life expectancy ≤18 months
- Pregnancy or lactation
Uremic Pericarditis
- The definitive treatment is dialysis
Tamponade
- Tamponade requires Pericardiocentesis
Disposition
- Hospitalization is not necessary in most cases
- Consider admission for:
Complications
- Pericardial Effusion and Tamponade
- Recurence
- Usually weeks to months after initial episode
- Management is same
- Constrictive Pericarditis
- Related to etiology; increased risk with bacterial pericarditis, rare with viral/idiopathic etiology
- Restrictive picture with pericardial calcifications on CXR, thickened on TTE
- Treat with pericardial window
See Also
- ST segment elevation
- STEMI
- Myocardial Infarction Complications
- Mattu ECG Case: Sept 3, 2012 - Pericarditis vs. STEMI
References
- ↑ LeWinter MM, et al. Clinical practice. Acute pericarditis. N Engl J Med. 2014 Dec 18;371(25):2410-6. PMID: 25517707.
- ↑ Imazio M, Gaita F, LeWinter M. Evaluation and Treatment of Pericarditis: A Systematic Review. JAMA 2015;314(14):1498–506.
- ↑ LeWinter MM. Clinical practice. Acute pericarditis. N Engl J Med. 2014 Dec 18;371(25):2410-6. doi: 10.1056/NEJMcp1404070. Review.
- ↑ Wang K, Asinger RW, and Marriott HJL. ST-segment Elevation in Conditions Other than Acute Myocardial Infarction. N Engl J Med 2003;349:2128-35.
- ↑ Bischof JE, Worrall C, Thompson P, et al. ST depression in lead aVL differentiates inferior ST-elevation myocardial infarction from pericarditis. Am J Emerg Med. 2016; 34(2):149-154.
- ↑ Chaubey VK and Chhabra L. Spodick’s Sign: A Helpful Electrocardiographic Clue to the Diagnosis of Acute Pericarditis. Perm J. 2014 Winter; 18(1): e122.
- ↑ Imazio M. A randomized trial of colchicine for acute pericarditis.N Engl J Med. 2013 Oct 17;369(16):1522-8 PDF
- ↑ ImazioM, BobbioM, Cecchi E, et al. Colchicine in addition to conventional therapy for acute pericarditis. Circulation. 2005;112(13):2012-2016.
- ↑ Imazio M, Brucato A, Cumetti D, et al. Corticosteroids for recurrent pericar- ditis: high versus low doses: a nonran- domized observation. Circulation 2008; 118:667-71.
- ↑ Imazio M.Colchicine as first-choice therapy for recurrent pericarditis: results of the CORE (COlchicine for REcurrent pericarditis) trial. Arch Intern Med. 2005 Sep 26;165(17):1987-91.
- ↑ Imazio M. Controversial issues in the management of pericardial diseases.Circulation. 2010 Feb 23;121(7):916-28.PDF