

Tobacco Use Among Adults with Mental Illness and Substance Use Disorders
 ShareCompartir
ShareCompartir
Adults with mental illness or substance use disorders smoke cigarettes more than adults without these disorders.1,2 The Substance Abuse and Mental Health Services Administration’s National Survey on Drug Use and Health (NSDUH) defines mental illness as any diagnosable mental, behavioral, or emotional disorder and defines substance use disorder as dependence or abuse of alcohol or illicit drugs.1
Approximately 25% of adults in the U.S. have some form of mental illness or substance use disorder, and these adults consume almost 40% of all cigarettes smoked by adults.1
Tobacco Use Prevalence
36.5% of adults with any mental illness reported current use* of tobacco in 2013 compared to 25.3% of adults with no mental illness.3
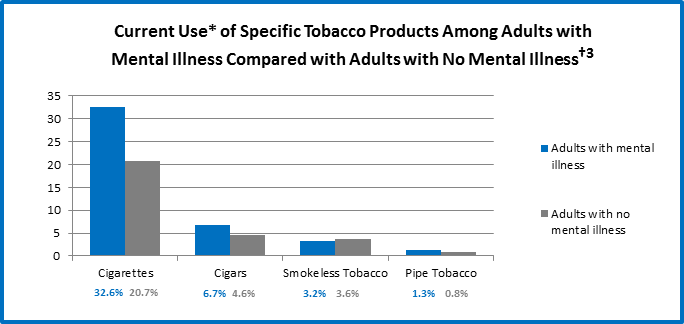
* “Current Use” is defined as self-reported consumption of cigarettes, cigars, smokeless tobacco, and pipe tobacco in the past year and past month (at the time of survey).
† Data taken from the National Survey on Drug Use and Health, 2013, and refer to adults aged 18 years and older reporting any mental illness in the past year.
65.2% of adult cigarette smokers reported co-use of alcohol in 2013 compared to 48.7% of adult non-smokers.4
| Smokers | Non-Smokers | |
|---|---|---|
| Current illicit drug use (in past month) | 18.9% | 4.2% |
| Marijuana | 15.3% | 3.0% |
| Cocaine | 1.8% | 0.2% |
| Heroin | 0.3% | 0.0% |
| Hallucinogens | 0.7% | 0.2% |
| Inhalants | 0.3% | 0.1% |
| Non-medical use of prescription drugs | 5.3% | 1.2% |
| Current alcohol use (in past month) | 65.2% | 48.7% |
| Binge drinking§ | 42.9% | 17.5% |
| Heavy drinking¶ | 15.7% | 3.8% |
‡ Data taken from the National Survey on Drug Use and Health, 2013, and refer to persons aged 26 years and older reporting smoking, drug, and/or alcohol use in the past 30 days.
§ Binge alcohol use is defined as drinking five or more drinks on the same occasion (i.e., at the same time or within a couple of hours of each other) on at least 1 day in the past 30 days.
¶ Heavy alcohol use is defined as drinking five or more drinks on the same occasion on each of 5 or more days in the past 30 days; all heavy alcohol users are also binge alcohol users.
Health Effects
- People with mental illness or substance use disorders die about 5 years earlier than those without these disorders5; many of these deaths are caused by smoking cigarettes.2,6
- The most common causes of death among people with mental illness are heart disease, cancer, and lung disease, which can all be caused by smoking.5
- Drug users who smoke cigarettes are four times more likely to die prematurely than those who do not smoke.7
- Nicotine has mood-altering effects that can temporarily mask the negative symptoms of mental illness, putting people with mental illness at higher risk for cigarette use and nicotine addiction.2,6
- Tobacco smoke can interact with and inhibit the effectiveness of certain medications taken by mental health and substance abuse patients.8
Quitting Behavior
- People with mental illness are less likely to stop smoking than those without mental illness; however, many smokers with mental illness want to quit.2
- People with mental illness are more likely to have stressful living conditions, have low annual household income, and lack access to health insurance, health care, and help quitting. All of these factors make it more challenging to quit.2,6
- Less than half of substance abuse treatment centers (42%) offer tobacco cessation services, and only 34% offer cessation counseling.9
Tobacco Industry Marketing and Influence
- The tobacco industry has used multiple strategies to market cigarettes to populations with mental illnesses, including:
- Developing relationships with and making financial contributions to organizations that work with mentally ill patients.10
- Funding research to foster the myth that cessation would be too stressful because persons with mental illness use nicotine to alleviate negative mood (i.e., self-medicate).2,10
- Providing free or cheap cigarettes to psychiatric facilities.2
- Supporting efforts to block smokefree psychiatric hospital policies.2
- Creating marketing plans that target marginalized populations, including mentally ill, homeless, and LGBT individuals. One example is "Project SCUM” (Sub Culture Urban Marketing), which was implemented in San Francisco in the mid-1990s.10
Culturally appropriate anti-smoking health marketing strategies and mass media campaigns like CDC’s Tips From Former Smokers national tobacco education campaign, as well as CDC-recommended tobacco prevention and control programs and policies, can help reduce the burden of disease among people with mental illness.
Myths
Myths about tobacco use among people with mental illness and substance abuse problems persist, including that—
- They are not interested in quitting.11
- They cannot quit.11
- Quitting interferes with recovery from mental illness or addictions.11
- Tobacco is not as harmful as other substances.10
- Tobacco is necessary for self-medication,11 and tobacco cessation would be too stressful.10
- Tobacco cessation efforts might prevent treatment of other addictions.10
However, with careful monitoring, delivering smoking cessation interventions does not interfere with treatments for mental illness and can actually be part of the treatment.6
Policy Strategies
A number of policy strategies have been suggested in the effort to encourage smoking cessation among people with mental illness and substance use disorders:
- Mental health facilities should consider going smokefree, including prohibiting tobacco use among employees6 or encouraging staff to quit.10
- Counselors should ask clients who smoke cigarettes or use other tobacco products about their interest in quitting while in substance abuse treatment.6,7,12
- The practice of providing mental health patients with cigarettes as an incentive or reward should be discontinued. Additionally, staff should not be allowed to smoke cigarettes with patients.2,6
- Extra help to succeed in quitting should be offered to patients who smoke cigarettes. This can include more counseling, combining stop-smoking medicines or using them longer,6 and follow-up to care (e.g., telephone calls by a counselor, extended counseling, or continued medications).10
Resources


- Substance Abuse and Mental Health Services Administration—list of additional resources [PDF–247 KB]
- National Behavioral Health Network for Tobacco and Cancer Control
- Smoking Cessation Leadership Center
Special Publication
Focusing on People with Mental Illness
 Recent research has shown that, like other smokers, adults with mental illness who smoke want to quit, can quit, and benefit from proven stop-smoking treatments.
Recent research has shown that, like other smokers, adults with mental illness who smoke want to quit, can quit, and benefit from proven stop-smoking treatments.
References
- Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality. The NSDUH Report: Adults With Mental Illness or Substance Use Disorder Account for 40 Percent of All Cigarettes Smoked [PDF–563 KB]. March 20, 2013. Rockville, MD [accessed 2016 May 18].
- Centers for Disease Control and Prevention. Vital Signs: Current Cigarette Smoking Among Adults Aged ≥18 Years With Mental Illness—United States, 2009–2011. Morbidity and Mortality Weekly Report 2013;62(05):81-7 [accessed 2016 May 18].
- Substance Abuse and Mental Health Services Administration. Results from the 2013 National Survey on Drug Use and Health: Mental Health Detailed Tables [PDF–3.2 MB]. Rockville, MD: Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality [accessed 2016 May 18].
- Substance Abuse and Mental Health Services Administration. Results from the 2013 National Survey on Drug Use and Health: Detailed Tables, Tables 6.10B and 6.24B. Rockville, MD: Substance Abuse and Mental health Services Administration, Center for Behavioral Health Statistics and Quality, 2014 [accessed 2016 May 18].
- Druss BG, Zhao L, Von Esenwein S, Morrato EH, Marcus SC. Understanding Excess Mortality in Persons With Mental Illness: 17-Year Follow Up of a Nationally Representative US Survey. Medical Care 2011;49(6):599–604 [cited 2016 May 18].
- Centers for Disease Control and Prevention. Vital Signs Fact Sheet: Adult Smoking Focusing on People With Mental Illness, February 2013. National Center for Chronic Disease and Health Promotion, Office on Smoking and Health, 2013 [accessed 2016 May 18].
- Smoking Cessation Leadership Center. Fact Sheet: The Tobacco Epidemic Among People With Behavioral Health Disorders. San Francisco: Smoking Cessation Leadership Center, University of California, 2015 [accessed 2016 May 18].
- Smoking Cessation Leadership Center. Fact Sheet: Drug Interactions With Tobacco Smoke. San Francisco: Smoking Cessation Leadership Center, University of California, 2015 [accessed 2016 May 18].
- Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality. The N-SSATS Report: Tobacco Cessation Services. September 19, 2013. Rockville, MD [accessed 2016 May 18].
- Centers for Disease Control and Prevention. Best Practices User Guide: Health Equity in Tobacco Prevention and Control. Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2015 [accessed 2016 May 18].
- Prochaska JJ. Smoking and Mental Illness—Breaking the Link. New England Journal of Medicine, 2011;365:196-8 [accessed 2016 May 18].
- Substance Abuse and Mental Health Services Administration. Tobacco Use Cessation During Substance Abuse Treatment Counseling. SAMHSA Advisory 2011;10(2):1-8 [accessed 2016 May 18].
For Further Information
Centers for Disease Control and Prevention
National Center for Chronic Disease Prevention and Health Promotion
Office on Smoking and Health
E-mail: tobaccoinfo@cdc.gov
Phone: 1-800-CDC-INFO
Media Inquiries: Contact CDC's Office on Smoking and Health press line at 770-488-5493.
- Page last reviewed: March 10, 2017
- Page last updated: March 10, 2017
- Content source: