Plasmodium knowlesi
Plasmodium knowlesi is a parasite that causes malaria in humans and other primates. It is found throughout Southeast Asia, and is the most common cause of human malaria in Malaysia. Like other Plasmodium species, P. knowlesi has a life cycle that requires infection of a mosquito host and a warm-blooded host. The natural primate host of P. knowlesi is the long-tailed macaque; however mosquitoes that feed on infected macaques can bite and infect humans. Infected humans can develop severe malaria, similar to that caused by Plasmodium falciparum. P. knowlesi malaria is an emerging disease first recognized in humans in 1965 but increasingly recognized as a human health burden in the 21st century.
| Plasmodium knowlesi | |
|---|---|
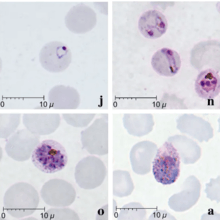 | |
| Giemsa-stained smears of Plasmodium knowlesi infecting human red blood cells | |
| Scientific classification | |
| (unranked): | Diaphoretickes |
| Clade: | TSAR |
| Clade: | SAR |
| Infrakingdom: | Alveolata |
| Phylum: | Apicomplexa |
| Class: | Aconoidasida |
| Order: | Haemospororida |
| Family: | Plasmodiidae |
| Genus: | Plasmodium |
| Species: | P. knowlesi |
| Binomial name | |
| Plasmodium knowlesi Sinton and Mulligan 1933 | |
P. knowlesi has also long been used in medical research. It was first used to cause fever as a treatment for neurosyphilis in the first half of the 20th century. Later, it became popular as a tool for studying parasite biology as well as vaccine and drug development. It readily infects the model primate the rhesus macaque, and can be grown in cell culture in human or macaque blood.
Life cycle
Like other Plasmodium parasites, P. knowlesi has a life cycle that requires it be passed back and forth between mammalian hosts and insect hosts. Primates are infected through the bite of an infected Anopheles mosquito which carries a parasite stage called the sporozoite in its salivary glands. Sporozoites follow the blood stream to the primate liver where they develop and replicate over 5 to 6 days before bursting, releasing thousands of daughter cells called merozoites into the blood (unlike the related P. vivax, P. knowlesi does not make latent hypnozoites in the liver).[1][2] The merozoites in the blood attach to and invade the primate's red blood cells. Inside the red blood cell, the parasite progresses through several morphologically distinguishable stages, called the ring stage, the trophozoite, and then the schizont. The schizont-infected red blood cells eventually burst, releasing up to 16 new merozoites into the blood stream that infect new red blood cells and continue the cycle.[3] P. knowlesi completes this red blood cell cycle every 24 hours, making it uniquely rapid among primate-infecting Plasmodium species (which generally take 48 or 72 hours).[2] Occasionally, parasites that invade red blood cells instead enter a sexual cycle, developing over approximately 48h into distinct sexual forms called microgametocytes or macrogametocytes.[3] These gametocytes remain in the blood to be ingested by mosquitoes.[3]
A mosquito ingests gametocytes when it takes a blood meal from an infected primate host. Once inside the mosquito gut, the gametocytes develop into gametes and then fuse to form a diploid zygote.[1] The zygotes matures into an ookinete, which migrates through the wall of the mosquito gut and develops into an oocyst.[1] The oocyst then releases thousands of sporozoites, which migrate through the mosquito to the salivary glands.[1] This entire process in the mosquito takes 12 to 15 days.[2]
Cell biology
The genome of P. knowlesi consists of 23.5 megabases of DNA separated into 14 chromosomes.[4] This contains approximately 5200 protein-coding genes, 80% of which have orthologs present in P. falciparum and P. vivax.[4] The genome contains two large gene families that are unique to P. knowlesi: SICAvar (schizont-infected cell agglutination variant) and Kir (knowlesi interspersed repeat).[4]
Evolution and taxonomy
Despite its morphological similarity to P. malariae, P. knowlesi is most closely related to other Plasmodium species that infect non-human primates.[5] The last common ancestor of all modern P. knowlesi strains lived an estimated 98,000 to 478,000 years ago.[5] Among human parasites, P. knowlesi is most closely related to P. vivax, from which it diverged between 18 million and 34 million years ago.[6][4] A phylogenetic tree comparing the Plasmodium species that infect humans is shown below:[4]
| Subgenus Plasmodium |
| ||||||||||||||||||
The population of P. knowlesi parasites is more genetically diverse than that of P. falciparum or P. vivax. Within P. knowlesi there are three genetically distinct subpopulations.[4] Two are present in the same areas of Malaysian Borneo; one infects long-tailed macaques while the other infects pig-tailed macaques.[7] The third is geographically separated and comes from the Malaysian Peninsula.[7] Populations of P. knowlesi isolated from macaques are genetically indistinguishable from those isolated from human infections, suggesting the same parasite populations can infect humans and macaques interchangeably.[8]
Three subspecies of P. knowlesi have been described based on differences in their appearance in stained blood films: P. knowlesi edesoni, P. knowlesi sintoni, and P. knowlesi arimai, which were isolated from Malaysia, Java, and Taiwan respectively.[2][9] The relationship between these described subspecies and the populations described in the modern literature is not clear.[2]
Distribution
Plasmodium knowlesi is found throughout Southeast Asia, where it primarily infects long-tailed macaques, pig-tailed macaques, and banded-leaf monkeys, as well as the mosquito vectors Anopheles hackeri, Anopheles latens, Anopheles cracens, Anopheles balabacensis, Anopheles dirus, and Anopheles introlatus.[7] Long-tailed macaques in the wild can be infected with P. knowlesi without any apparent disease, even when they're simultaneously infected with various other Plasmodium species.[2][6] P. knowlesi is rarely found outside of Southeast Asia, likely because the species it infects are restricted to that region.[7]
Role in human disease
P. knowlesi can cause both uncomplicated and severe malaria in humans. Symptoms typically begin approximately 11 days after an infected mosquito has bitten a person and the parasites can be seen in the blood between 10 – 12 days after infection.[10] Those infected nearly always experience fever and chills.[11] People with uncomplicated P. knowlesi malaria often also experience headaches, joint pain, malaise, and loss of appetite.[11] Less commonly, people report coughing, abodminal pain, diarrhera, nausea, and vomiting.[11] Uncomplicated P. knowlesi malaria can resolve on its own, or can be treated with antimalarial drugs.[11] Unlike other human malarias, P. knowlesi malaria tends to have fevers that spike every 24 hours, and is therefore often called daily or "quotidian" malaria.[12]
Approximately 10% of people infected with P. knowlesi develop severe malaria.[8] Severe P. knowlesi malaria resembles severe malaria caused by P. falciparum. Those with severe disease may experience shortness of breath, abdominal pain, and vomiting.[11] As disease progresses, hyperparasitemia develops and likely causes acute kidney injury, jaundice, shock, and respiratory distress.[11][13] Metabolic acidosis is uncommon, but can occur is particularly severe cases.[13] Unlike P. falciparum malaria, severe P. knowlesi malaria rarely causes coma.[13] Approximately 1-2% of cases are fatal.[8]
Diagnosis
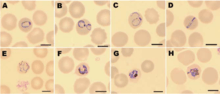
As with other causes of malaria, P. knowlesi infection is traditionally diagnosed by examining stained blood films under a microscope.[7] Complicating proper diagnosis, several P. knowlesi life stages are indistinguishable by microscopy from the more benign P. malariae.[7] Other stages resemble P. falciparum and P. vivax, and misdiagnosis as either is common.[13] While some rapid diagnostic tests can detect P. knowlesi, they tend to have poor sensitivity and specificity and are therefore not always reliable.[7][14] Detection of nucleic acid by PCR or real-time PCR is the most reliable method for detecting P. knowlesi, and differentiating it from other Plasmodium species infection; however due to the relatively slow and expensive nature of PCR, this is not available in many endemic areas.[7] Loop-mediated isothermal amplification methods of P. knowlesi detection have also been developed, but are not yet widely used.[7]
Treatment
Because P. knowlesi takes only 24 hours to complete its erythrocytic cycle, it can rapidly result in very high levels of parasitemia with fatal consequences.[13] For those with uncomplicated malaria, the World Health Organization recommends treatment with artemisinin-based combination therapy (ACT) or chloroquine.[7] For those with severe malaria, the World Health Organization recommends administration of intravenous artesunate for at least 24 hours, followed by ACT treatment.[13] Since P. knowlesi infection of humans has been recognized for a short time, relatively few studies have been done on P. knowlesi sensitivity to various antimalarial drugs.[7] However, in studies that have been done, combinations of chloroquine and primaquine, artesunate and mefloquine, artemether and lumefantrine, and chloroquine alone have all been found to be effective treatments for uncomplicated P. knowlesi malaria.[7][13] There is no evidence of P. knowlesi developing resistance to current antimalarials.[13]
Prevention
Risk of P. knowlesi infection is reduced in households that practice indoor residual spraying of insecticide.[7] As with other mosquito-borne infections, sleeping under bed nets may provide some protection against infection; however, in one study in Sabah, Malaysia, use of bed nets had little effect on infection risk.[7]
Epidemiology
P. knowlesi is the most common cause of malaria in Malaysia.[4] However, cases of P. knowlesi malaria have been reported in most countries of Southeast Asia as well as travelers from the region.[7] Reports of P. knowlesi malaria have increased substantially in the 21st century; this is likely due to increases in capacity to accurately diagnose malaria cases, awareness of P. knowlesi as a cause of human disease, and proximity of humans to the primate and mosquito hosts.[7]
Infection with P. knowlesi is associated with several socioeconomic and lifestyle factors that bring people into close contact with primate and mosquito hosts.[7] Those who live near dense forest cover and low elevation are more likely to be infected by P. knowlesi.[7] Infections are also more common in people over the age of 15, and those who work on a farm or palm oil plantation.[7] As with P. vivax infection, people with Glucose-6-phosphate dehydrogenase deficiency are less likely to be infected by P. knowlesi than those without the condition.[7]
Research
P. knowlesi has long been used as a research model for studying the interaction between parasite and host as well as the development of antimalarial vaccines and drugs.[6] Its utility as a research model is partly due to its ability to infect rhesus macaques, a common laboratory model primate. Rhesus macaques are highly susceptible to P. knowlesi and can be infected by mosquito bite, injection of sporozoites, or injection of blood-stage parasites.[2][6] Infected monkeys develop some hallmarks of human malaria including anemia and enlargement of the spleen and liver.[2] Infection is typically fatal if untreated, with the cause of death seemingly circulatory failure characterized by adhesion of infected red blood cells to the blood vessel walls.[2] Monkeys can be cured of infection by treatment with antimalarials; repeated infection followed by cure results in the monkeys developing some immunity to infection, a topic that has also been the subject of substantial research.[2]
P. knowlesi is also used for in vitro research into Plasmodium cell biology. Isolated sporozoites can infect primary rhesus hepatocytes, allowing the in vitro study of the parasite liver stage.[6] Additionally, P. knowlesi and P. falciparum are the only Plasmodium species that can be maintained continuously in cultured red blood cells, both rhesus and human.[6] Facilitating molecular biology research, the P. knowlesi genome has been sequenced and is available on PlasmoDB and other online repositories.[6] P. knowlesi can be genetically modified in the lab by transfection either in the rhesus macaque model system, or in blood cell culture.[6][15] Blood-infecting stages and sporozoites can be stored long-term by freezing with glycerolyte, allowing the preservation of strains of interest.[1]
History of discovery

The Italian physician Giuseppe Franchini first described what may have been P. knowlesi in 1927 when he noted a parasite distinct from P. cynomolgi and P. inui in the blood of a long-tailed macaque.[16][17] In 1931, the parasite was again seen in a long-tailed macaque by H. G. M. Campbell during his work on kala azar; Campbell's colleague Lionel Napier drew blood from the affected monkey and inoculated three laboratory monkeys, one of which was a rhesus macaque that developed a severe infection.[3][18] Campbell and Napier gave the infected monkey to Biraj Mohan Das Gupta who was able to maintain the parasite by serial passage through monkeys.[19] In 1932 Das Gupta, along with his supervisor Robert Knowles described the morphology of the parasite in macaque blood, and demonstrated that it could infect three human patients (in each case it was used to induce fever with the hope of treating another infection).[3][20] Also in 1932, John Sinton and H. W. Mulligan further described the morphology of the parasite in blood cells, determined it to be a distinct species from others described, and named it Plasmodium knowlesi in honor of Robert Knowles.[3]
Soon thereafter, in 1935 C. E. Van Rooyen and George R. Pile reported using P. knowlesi infection to treat general paralysis in psychiatric patients. P. knowlesi would go on to be used as a general pyretic agent for various diseases, particularly neurosyphilis for which it was used until at least 1955.[19] While, Cyril Garnham had suggested in 1957 that P. knowlesi might naturally infect humans,[21] the first documented case of a human naturally infected with P. knowlesi was in 1965 in a U.S. Army surveryor who developed chills and fever after a five-day deployment in Malaysia.[19][22] Based on this finding, a team at the Institute for Medical Research in Peninsular Malaysia undertook a survey of people living in proximity to macaques, but failed to find evidence that simian malaria was being transmitted to humans.[19]
At the same time, the tractability of P. knowlesi as a research system led to its use for several seminal discoveries in malaria research. In the late 1960s and early 1970s, several groups characterized how P. knowlesi antigenic variation contributed to immune evasion and chronic infection.[19] In 1975 Louis H. Miller and others showed that P. knowlesi required Duffy factor on the surface of red blood cells in order to invade them (they would go on to show the same requirement for P. vivax a year later).[19]
Work on P. knowlesi as a human malaria parasite was revitalized in 2004, when Balbir Singh and others used PCR to show that over half of a group of humans diagnosed with P. malariae malaria in Malaysian Borneo were actually infected with P. knowlesi.[19][23] Over the following decade, several investigators used molecular detection methods capable of distinguishing P. knowlesi from morphologically similar parasites to attribute an increasing proportion of malaria cases to P. knowlesi throughout Southeast Asia.[24] Work with archival samples has shown that infection with this parasite has occurred in Malaysia at least since the 1990s.[25]
References
- Collins, W. E. (2012). "Plasmodium knowlesi: A Malaria Parasite of Monkeys and Humans*". Annual Review of Entomology (Submitted manuscript). 57: 107–121. doi:10.1146/annurev-ento-121510-133540. PMID 22149265.
- Butcher GA, Mitchell GH (September 2016). "The role of Plasmodium knowlesi in the history of malaria research". Parasitology. Cambridge University Press. 145 (1): 6–17. doi:10.1017/S0031182016001888. PMID 27829470.
- Coatney GR, Collins WE, Warren M, Contacos PG (1971). The Primate Malarias. Atlanta, GA: Division of Parasitic Diseases, U.S. Centers for Disease Control. pp. 317–334. Retrieved 26 August 2019.
- Garrido-Cardenas JA, Gonzalez-Ceron L, Manzano-Agugliaro F, Mesa-Valle C (January 2019). "Plasmodium genomics: an approach for learning about and ending human malaria". Parasitology Research. Springer. 118 (1): 1–27. doi:10.1007/s00436-018-6127-9. PMID 30402656.
- Lee KS, Divis PC, Zakaria SK, Matusop A, Julin RA, Conway DJ, Cox-Singh J, Singh B (2011). Kazura JW (ed.). "Plasmodium knowlesi: Reservoir Hosts and Tracking the Emergence in Humans and Macaques". PLoS Pathog. 7 (4): e1002015. doi:10.1371/journal.ppat.1002015. PMC 3072369. PMID 21490952.
- Pasini EM, Zeeman AM, Voorberg-Vanderwel A, Kocken CH (November 2016). "Plasmodium knowlesi: a relevant, versatile experimental malaria model". Parasitology. Cambridge University Press. 145 (1): 56–70. doi:10.1017/S0031182016002286. PMID 27938428.
- Amir A, Cheong FW, de Silva JR, Liew JW, Lau YL (August 2018). "Plasmodium knowlesi malaria: current research perspectives". Infection and Drug Resistance. Dove Press. 11: 1145–1155. doi:10.2147/IDR.S148664. PMID 30127631.
- Millar SB, Cox-Singh J (July 2015). "Human infections with Plasmodium knowlesi-zoonotic malaria". Clinical Microbiology and Infection. Elsevier. 21 (7): 640–648. doi:10.1016/j.cmi.2015.03.017.
- Garnham, PCC (1963) A new sub-species of Plasmodium knowlesi in the long-tailed macaque. J Trop Med & Hyg 66 : 156-158
- Bronner U.; Divis P.C.; Farnert A.; Singh B. (2009). "Swedish traveller with Plasmodium knowlesi malaria after visiting Malaysian Borneo". Malar. J. 8: 15. doi:10.1186/1475-2875-8-15. PMC 2634766. PMID 19146706..
- Singh, B.; Daneshvar, C. (2013). "Human Infections and Detection of Plasmodium knowlesi". Clinical Microbiology Reviews. 26 (2): 165–184. doi:10.1128/CMR.00079-12. PMC 3623376. PMID 23554413.
- Chin W, Contacos PG, Coatney RG, Kimbal HR (1965). "A naturally acquired quotidian-type malaria in man transferable to monkeys". Science. 149 (3686): 865. Bibcode:1965Sci...149..865C. doi:10.1126/science.149.3686.865. PMID 14332847.
- Barber BE, Grigg MJ, William T, Yeo TW, Anstey NM (March 2017). "The treatment of Plasmodium knowlesi malaria". Trends in Parasitology. Elsevier. 33 (3): 242–253. doi:10.1016/j.pt.2016.09.002. PMID 27707609.
- Despommier DD, Griffin DO, Gwadz RW, Hotez PJ, Knirsch CA. Paraistic Diseases (PDF) (7 ed.). Parasites Without Borders. p. 112.
- de Koning-Ward TF; Gilson PR; Crabb BS (June 2015). "Advances in molecular genetic systems in malaria". Nature Reviews Microbiology. Macmillan. 13 (6): 373–387. doi:10.1038/nrmicro3450. PMID 25978707.
- Franchini G (1927) Su di un plasmodio pigmentato di una scimmia. Arch Ital Sci Med Colon 8:187–90
- Antinori S, Milazzo L, Corbellino M (October 2011). "Plasmodium knowlesi: an overlooked Italian discovery?". Clinical Infectious Diseases. 53 (8): 849. doi:10.1093/cid/cir527.
- L. Everard Napier; H. G. M. Campbell (May 1932). "Observations on a Plasmodium infection which causes haemoglobinuria in certain species of monkey" (PDF). The Indian Medical Gazette. pp. 246–249. Retrieved 27 August 2019.
- Antinori, Spinello; Galimberti, Laura; Milazzo, Laura; Corbellino, Mario (2013). "Plasmodium knowlesi: The emerging zoonotic malaria parasite". Acta Tropica. 125 (2): 191–201. doi:10.1016/j.actatropica.2012.10.008. PMID 23088834.
- Knowles R, Das Gupta BM (June 1932). "A study of monkey malaria, and its experimental transmission to man". Indian Medical Gazette. 67 (6): 301–320. PMC 5231565. PMID 29010910.
- Garnham PC, Lainson R, Cooper W (1957). "The tissue stages and sporogony of Plasmodium knowlesi". Trans R Soc Trop Med Hyg. 51 (5): 384–396. doi:10.1016/0035-9203(57)90071-8. PMID 13467997.
- Mason Dentinger, Rachel (26 August 2015). "Patterns of Infection and Patterns of Evolution: How a Malaria Parasite Brought "Monkeys and Man" Closer Together in the 1960s". Journal of the History of Biology. 49 (2): 359–395. doi:10.1007/s10739-015-9421-8. PMID 26307748.
- Singh B, Lee KS, Matusop A, Radhakrishnan A, Shamsul SS, Cox-Singh J, Thomas A, Conway DJ (2004). "A large focus of naturally acquired Plasmodium knowlesi infections in human beings" (PDF). Lancet. 363 (9414): 1017–24. doi:10.1016/S0140-6736(04)15836-4. PMID 15051281.
- Vythilingam I, Noorazian YM, Huat TC, Jiram AI, Yusri YM, Azahari AH, Norparina I, Noorrain A, Lokmanhakim S (2008). "Plasmodium knowlesi in humans, macaques and mosquitoes in peninsular Malaysia". Parasit Vectors. 1 (1): 26. doi:10.1186/1756-3305-1-26. PMC 2531168. PMID 18710577.
- Lee K.S.; Cox-Singh J.; Brooke G.; Matusop A.; Singh B. (2009). "Plasmodium knowlesi from archival blood films: Further evidence that human infections are widely distributed and not newly emergent in Malaysian Borneo". Int J Parasitol. 39 (10): 1125–1128. doi:10.1016/j.ijpara.2009.03.003. PMC 2722692. PMID 19358848.
External links
- CDC malaria page
- WHO malaria page
- P. knowlesi genome data
- Short film on the discovery of the role of P. knowlesi in human malaria
| Biology |
|
|---|---|
| Control and prevention | |
| Diagnosis and treatment |
|
| Society and malaria |
|
| Organisations |
|
| |