Commotio cordis
Commotio cordis (Latin, "agitation of the heart") is an often lethal disruption of heart rhythm that occurs as a result of a blow to the area directly over the heart (the precordial region) at a critical time during the cycle of a heart beat, producing what is termed an R-on-T phenomenon that leads to the condition. It is a form of ventricular fibrillation (V-Fib), not mechanical damage to the heart muscle or surrounding organs, and not the result of heart disease. The fatality rate is about 65% even with prompt CPR and defibrillation, and more than 80% without.[1][2]
| Commotio cordis | |
|---|---|
 | |
| Human adult thorax, showing the outline of the heart (in red). The sensitive zone for mechanical induction of heart rhythm disturbances lies between the 2nd and the 4th ribs, to the left of the sternum | |
| Specialty | Emergency medicine |
Commotio cordis occurs mostly in boys and young men (average age 15), usually during sports, most frequently baseball, often despite a chest protector. It is usually caused by a projectile, but can also be caused by the blow of an elbow or other body part. Being less developed, the thorax of an adolescent is likely more prone to this injury given the circumstances.
The phenomenon was confirmed experimentally in the 1930s, with research in anaesthetized rabbits, cats and dogs.[3]
Causes
Sport
Commotio cordis is a very rare event, but nonetheless is often considered when an athlete presents with sudden cardiac death. Some of the sports which have a risk for this cause of trauma are baseball, American football, association football, ice hockey, polo, rugby football, cricket, softball, pelota, fencing, lacrosse, boxing, karate, kung fu, and other martial arts (see Touch of Death). Children are especially vulnerable, possibly due to the mechanical properties of their thoracic skeleton. From 1996 to spring 2007, the USA National Commotio Cordis Registry had 188 cases recorded, with about half occurring during organized sports.[2] Almost all (96%) of the victims were male, the mean age of the victims during that period was 14.7 years, and fewer than one in five survived the incident.[2]
Other situations
Commotio cordis may also occur in other situations, such as in children who are punished with blows over the precordium, cases of torture, and frontal collisions of motor vehicles (the impact of the steering wheel against the thorax, although this has decreased substantially with the use of safety belts and air bags). In one fatality, the impact to the chest was the result of an exploding whipped cream canister.[4]
In contrast, the precordial thump (hard blows given over the precordium with a closed fist to revert cardiac arrest) is a sanctioned procedure for emergency resuscitation by trained health professionals witnessing a monitored arrest when no equipment is at hand, endorsed by the latest guidelines of the International Liaison Committee on Resuscitation. It has been discussed controversially, as—in particular in severe hypoxia—it may cause the opposite effect (i.e., a worsening of rhythm—commotio cordis). In a normal adult, the energy range involved in the precordial thump is five to 10 times below that associated with commotio cordis.[5]
Mechanism
These factors influence the chance of commotio cordis:
- Direction of impact over the precordium (precise area, angle of impact)
- Total applied energy (area of impact versus energy, i.e., the kinetic energy of the projectile )
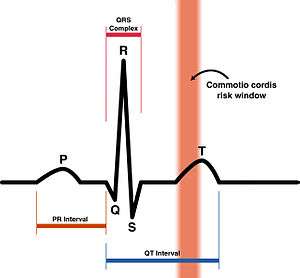
- Impact occurring within a specific 10– to 30-millisecond portion of the cardiac cycle. This period occurs in the ascending phase of the T wave, when the ventricular myocardium is repolarizing, moving from systole to diastole (relaxation).

The small window of vulnerability explains why it is a rare event. Considering that the total cardiac cycle has a duration of 1 second (for a base cardiac frequency of 60 beats per minute), the probability of a mechanical trauma within the window of vulnerability is 1 to 3% only. That also explains why the heart becomes more vulnerable when it is physically strained by sports activities:
- The increase in heart rate (exercise tachycardia) may double the probability above (e.g., with 120 beats per minute the cardiac cycle shortens to 500 milliseconds without fundamentally altering the window-of-vulnerability's size)
- Relative exercise-induced hypoxia and acceleration of the excitoconductive system of the heart make it more susceptible to stretch-induced ventricular fibrillation.
The cellular mechanisms of commotio cordis are still poorly understood, but probably related to the activation of mechanosensitive proteins, ion channels. These trigger extra electrical excitation waves which, if occurring right at the trailing edge of a previous electrical cycle, can give rise to ventricular fibrillation.[6] Since the trailing edge of the preceding electrical cycle travels over the ventricular surface, the critical window for mechanical induction of ventricular fibrillation varies locally - i.e. the commotio cordis risk window exists in time and in space.[6] This helps to explain why precordial impacts tend to have benign consequences.
Impact energies of at least 50 joules are estimated to be required to cause cardiac arrest, when applied in the right time and spot of the precordium of an adult.[5] Impacts up to 130 joules have already been measured with hockey pucks and lacrosse balls, 450 joules in karate punches, and 1028 joules in boxer Rocky Marciano's punch.[7] The 50-joule threshold, however, can be considerably lowered when the victim's heart is under ischemic conditions, such as in coronary artery insufficiency.[5]
Also an upper limit of impact energy is applied to the heart; too much energy will create structural damage to the heart muscle, as well as causing electrical upset. This condition is referred to as contusio cordis (from Latin for bruising of the heart). On isolated guinea pig hearts, as little as 5 mJ were needed to induce release of creatine kinase, a marker for muscle cell damage.[8] Obviously, this figure does not include the dissipation of energy through the chest wall, and is not scaled up for humans, but it is indicative that relatively small amounts of energy are required to reach the heart before physical damage is done.
Prevention
The risk would probably be reduced by improved coaching techniques, such as teaching young batters to turn away from the ball to avoid errant pitches, according to doctors. Defensive players in lacrosse and hockey are now taught to avoid using their chest to block the ball or puck. Starting in 2017, high school lacrosse players are penalized, and play stopped immediately, if they enter their own goal crease with the apparent intent of blocking shots or acting as goalkeeper.[9]
Chest protectors and vests are designed to reduce trauma from blunt bodily injury, but this does not offer protection from commotio cordis and may offer a false sense of security. Almost 20% of the victims in competitive football, baseball, lacrosse and hockey were wearing protectors. This ineffectiveness has been confirmed by animal studies. Development of adequate chest protectors may prove difficult.[1]
Treatment

Most cases are fatal. Automated external defibrillators have helped increase the survival rate to 35%.[1] Defibrillation must be started as soon as possible (within 3 minutes) for maximal benefit. Commotio cordis is the leading cause of fatalities in youth baseball in the US, with two to three deaths per year.[10] It has been recommended that "communities and school districts reexamine the need for accessible automatic defibrillators and cardiopulmonary resuscitation-trained coaches at organized sporting events for children."[11]
Legal issues
Several people have been charged and convicted for deaths of victims of commotio cordis, even when the blows rendered were never given with an intent to kill.[12] In 1992, Italian hockey player Miran Schrott died after a blow to his chest from the stick of Canadian-Italian player Jimmy Boni. Boni was charged with culpable homicide, and eventually pleaded guilty to manslaughter, paying a $1,300 fine and $175,000 restitution to Schrott's family.[13]
See also
- Pulmonary contusion
- Touch of Death
- Commotio thoracis
References
- Maron BJ, Estes NA (March 2010). "Commotio cordis". The New England Journal of Medicine. 362 (10): 917–27. doi:10.1056/NEJMra0910111. PMID 20220186.
- "Position Statement on Commotio Cordis". US Lacrosse. January 2008. Retrieved 22 February 2017.
- Schlomka G (1934). "Commotio cordis und ihre Folgen. Die Einwirkung stumpfer Brustwandtraumen auf das Herz". Ergebnisse der Inneren Medizin und Kinderheilkunde. 47: 1–91. doi:10.1007/978-3-642-90672-5_1. ISBN 978-3-642-88817-5.
- Barnes, Zahra. "Fitness Blogger Rebecca Burger Died After a Whipped Cream Dispenser Exploded". SELF. Retrieved 2017-07-14.
- Kohl P, Sachs F & Franz M (eds): Cardiac Mechano-Electric Feedback and Arrhythmias: from Pipette to Patient. Elsevier (Saunders), Philadelphia 2005.
- Quinn, T. Alexander; Jin, Honghua; Lee, Peter; Kohl, Peter (2017-08-01). "Mechanically Induced Ectopy via Stretch-Activated Cation-Nonselective Channels Is Caused by Local Tissue Deformation and Results in Ventricular Fibrillation if Triggered on the Repolarization Wave Edge (Commotio Cordis)". Circulation: Arrhythmia and Electrophysiology. 10 (8): e004777. doi:10.1161/CIRCEP.116.004777. ISSN 1941-3149. PMC 5555388. PMID 28794084.
- "science.ca View question #821". Retrieved 2008-02-23.
- Cooper PJ, Epstein A, Macleod IA, Schaaf ST, Sheldon J, Boulin C, Kohl P (2006). "Soft tissue impact characterisation kit (STICK) for ex situ investigation of heart rhythm responses to acute mechanical stimulation". Progress in Biophysics and Molecular Biology. 90 (1–3): 444–68. doi:10.1016/j.pbiomolbio.2005.07.004. PMID 16125216.
- Rule 4.18.4, 2018 Boys' Lacrosse Rule Book. Indianapolis, Indiana: National Federation of State High School Associations. 2018. p. 47.
- Abrunzo TJ (November 1991). "Commotio cordis. The single, most common cause of traumatic death in youth baseball". American Journal of Diseases of Children. 145 (11): 1279–82. doi:10.1001/archpedi.1991.02160110071023. PMID 1951221.
- Salib EA, Cyran SE, Cilley RE, Maron BJ, Thomas NJ (December 2005). "Efficacy of bystander cardiopulmonary resuscitation and out-of-hospital automated external defibrillation as life-saving therapy in commotio cordis". The Journal of Pediatrics. 147 (6): 863–6. doi:10.1016/j.jpeds.2005.07.041. PMID 16356450.
- Maron BJ, Mitten MJ, Greene Burnett C (January 2002). "Criminal consequences of commotio cordis". The American Journal of Cardiology. 89 (2): 210–3. doi:10.1016/S0002-9149(01)02202-0. PMID 11792344.
- Maki, Allan (28 September 2007). "Darcy Robinson's death brings shock". The Globe and Mail. Retrieved 29 February 2016.
Further reading
- Kohl P, Nesbitt AD, Cooper PJ, Lei M (May 2001). "Sudden cardiac death by Commotio cordis: role of mechano-electric feedback". Cardiovascular Research. 50 (2): 280–9. doi:10.1016/S0008-6363(01)00194-8. PMID 11334832.
- Geddes LA, Roeder RA (January 2005). "Evolution of our knowledge of sudden death due to commotio cordis". The American Journal of Emergency Medicine. 23 (1): 67–75. doi:10.1016/j.ajem.2003.12.023. PMID 15672341.
External links
| Classification | |
|---|---|
| External resources |
- Yabek, S.M. Commotio cordis. eMedicine, September 2005.