Autism therapies
Autism therapies are interventions that attempt to lessen the deficits and problem behaviours associated with autism spectrum disorder (ASD) in order to increase the quality of life and functional independence of individuals with autism. Treatment is typically catered to the person's needs. Treatments fall into two major categories: educational interventions and medical management. Training and support are also given to families of those with ASD.[2]
| Autism therapies | |
|---|---|
 A three-year-old with autism points to fish in an aquarium, as part of an experiment on the effect of intensive shared-attention training on language development.[1] |
Studies of interventions have some methodological problems that prevent definitive conclusions about efficacy.[3] Although many psychosocial interventions have some positive evidence, suggesting that some form of treatment is preferable to no treatment, the systematic reviews have reported that the quality of these studies has generally been poor, their clinical results are mostly tentative, and there is little evidence for the relative effectiveness of treatment options.[4] Intensive, sustained special education programs and behavior therapy early in life can help children with ASD acquire self-care, social, and job skills,[2] and often can improve functioning, and decrease symptom severity and maladaptive behaviors;[5] claims that intervention by around age three years is crucial are not substantiated.[6] Available approaches include applied behavior analysis (ABA), developmental models, structured teaching, speech and language therapy, social skills therapy, and occupational therapy.[2] Educational interventions have some effectiveness in children: intensive ABA treatment has demonstrated effectiveness in enhancing global functioning in preschool children,[7] and is well established for improving intellectual performance of young children.[5] Neuropsychological reports are often poorly communicated to educators, resulting in a gap between what a report recommends and what education is provided.[8] The limited research on the effectiveness of adult residential programs shows mixed results.[9]
Many medications are used to treat problems associated with ASD.[10] More than half of U.S. children diagnosed with ASD are prescribed psychoactive drugs or anticonvulsants, with the most common drug classes being antidepressants, stimulants, and antipsychotics.[11] Aside from antipsychotics,[12] there is scant reliable research about the effectiveness or safety of drug treatments for adolescents and adults with ASD.[13][14] A person with ASD may respond atypically to medications, the medications can have adverse effects, and no known medication relieves autism's core symptoms of social and communication impairments.[15]
Some newer treatments are geared towards children with ASD and focus on community-based education and living, and early intervention. The treatments that may have the most benefit focus on early behavioral development and have shown significant improvements in communication and language. These treatments include parental involvement as well as special educational methods. Further research will examine the long term outcome of these treatments and the details surrounding the process and execution of them.[16]
Many alternative therapies and interventions are available, ranging from elimination diets to chelation therapy. Few are supported by scientific studies.[17][18][19][20][21] Treatment approaches lack empirical support in quality-of-life contexts, and many programs focus on success measures that lack predictive validity and real-world relevance.[22] Scientific evidence appears to matter less to service providers than program marketing, training availability, and parent requests.[23] Even if they do not help, conservative treatments such as changes in diet are expected to be harmless aside from their bother and cost.[24] Dubious invasive treatments are a much more serious matter: for example, in 2005, botched chelation therapy killed a five-year-old boy with autism.[25]
Treatment is expensive;[26] indirect costs are more so. For someone born in 2000, a U.S. study estimated an average discounted lifetime cost of $4.3 million (2019 dollars, inflation-adjusted from 2003 estimate[27]), with about 10% medical care, 30% extra education and other care, and 60% lost economic productivity.[28] A UK study estimated discounted lifetime costs at £1.75 million and £1.13 million for an autistic person with and without intellectual disability, respectively[29] (2019 pounds, inflation-adjusted from 2005/06 estimate[30]). Legal rights to treatment are complex, vary with location and age, and require advocacy by caregivers.[31] Publicly supported programs are often inadequate or inappropriate for a given child, and unreimbursed out-of-pocket medical or therapy expenses are associated with likelihood of family financial problems;[32] one 2008 U.S. study found a 14% average loss of annual income in families of children with ASD,[33] and a related study found that ASD is associated with higher probability that child care problems will greatly affect parental employment.[34] After childhood, key treatment issues include residential care, job training and placement, sexuality, social skills, and estate planning.[31]
Educational interventions
Educational interventions attempt to help children not only to learn academic subjects and gain traditional readiness skills, but also to improve functional communication and spontaneity, enhance social skills such as joint attention, gain cognitive skills such as symbolic play, reduce disruptive behavior, and generalize learned skills by applying them to new situations. Several model programs have been developed, which in practice often overlap and share many features, including:[2]
- early intervention that does not wait for a definitive diagnosis;
- intense intervention, at least 25 hours per week, 12 months per year;
- low student/teacher ratio;
- family involvement, including training of parents;
- interaction with neurotypical peers;
- social stories, ABA and other visually based training;[35]
- structure that includes predictable routine and clear physical boundaries to lessen distraction; and
- ongoing measurement of a systematically planned intervention, resulting in adjustments as needed.
Several educational intervention methods are available, as discussed below. They can take place at home, at school, or at a center devoted to autism treatment; they can be done by parents, teachers, speech and language therapists, and occupational therapists.[2][36] A 2007 study found that augmenting a center-based program with weekly home visits by a special education teacher improved cognitive development and behavior.[37]
Studies of interventions have methodological problems that prevent definitive conclusions about efficacy.[3] Although many psychosocial interventions have some positive evidence, suggesting that some form of treatment is preferable to no treatment, the methodological quality of systematic reviews of these studies has generally been poor, their clinical results are mostly tentative, and there is little evidence for the relative effectiveness of treatment options.[4] Concerns about outcome measures, such as their inconsistent use, most greatly affect how the results of scientific studies are interpreted.[38] A 2009 Minnesota study found that parents follow behavioral treatment recommendations significantly less often than they follow medical recommendations, and that they adhere more often to reinforcement than to punishment recommendations.[39] Intensive, sustained special education programs and behavior therapy early in life can help children acquire self-care, social, and job skills,[2] and often improve functioning and decrease symptom severity and maladaptive behaviors;[5] claims that intervention by around age three years is crucial are not substantiated.[6]
Applied behavior analysis
Applied behavior analysis (ABA) is the applied research field of the science of behavior analysis, and it underpins a wide range of techniques used to treat autism and many other behaviors and diagnoses,[40] including those who are patients in rehab or in whom a behavior change is desired . ABA-based interventions focus on teaching tasks one-on-one using the behaviorist principles of stimulus, response and reward,[41] and on reliable measurement and objective evaluation of observed behavior.[2] There is wide variation in the professional practice of behavior analysis and among the assessments and interventions used in school-based ABA programs.[42]
Conversely, various major figures within the autistic community have written biographies detailing the harm caused by the provision of ABA, including restraint, sometimes used with mild self stimulatory behaviors such as hand flapping, and verbal abuse. The Autistic Self Advocacy Network campaigns against the use of ABA in autism.[43][44]
Discrete trial training
Many intensive behavioral interventions rely heavily on discrete trial teaching (DTT) methods, which use stimulus-response-reward techniques to teach foundational skills such as attention, compliance, and imitation.[46] However, children have problems using DTT-taught skills in natural environments.[2] These students are also taught with naturalistic teaching procedures to help generalize these skills. In functional assessment, a common technique, a teacher formulates a clear description of a problem behavior, identifies antecedents, consequences, and other environmental factors that influence and maintain the behavior, develops hypotheses about what occasions and maintains the behavior, and collects observations to support the hypotheses.[2] A few more-comprehensive ABA programs use multiple assessment and intervention methods individually and dynamically.[42]
ABA-based techniques have demonstrated effectiveness in several controlled studies: children have been shown to make sustained gains in academic performance, adaptive behavior, and language, with outcomes significantly better than control groups.[2] A 2009 review of educational interventions for children, whose mean age was six years or less at intake, found that the higher-quality studies all assessed ABA, that ABA is well-established and no other educational treatment is considered probably efficacious, and that intensive ABA treatment, carried out by trained therapists, is demonstrated effective in enhancing global functioning in pre-school children.[7] These gains maybe complicated by initial IQ.[47] A 2008 evidence-based review of comprehensive treatment approaches found that ABA is well established for improving intellectual performance of young children with ASD.[5] A 2009 comprehensive synthesis of early intensive behavioral intervention (EIBI), a form of ABA treatment, found that EIBI produces strong effects, suggesting that it can be effective for some children with autism; it also found that the large effects might be an artifact of comparison groups with treatments that have yet to be empirically validated, and that no comparisons between EIBI and other widely recognized treatment programs have been published.[48] A 2009 systematic review came to the same principal conclusion that EIBI is effective for some but not all children, with wide variability in response to treatment; it also suggested that any gains are likely to be greatest in the first year of intervention.[6] A 2009 meta-analysis concluded that EIBI has a large effect on full-scale intelligence and a moderate effect on adaptive behavior.[49] However, a 2009 systematic review and meta-analysis found that applied behavior intervention (ABI), another name for EIBI, did not significantly improve outcomes compared with standard care of preschool children with ASD in the areas of cognitive outcome, expressive language, receptive language, and adaptive behavior.[50] Applied behavior analysis is cost effective for administrators [51]
Recently behavior analysts have built comprehensive models of child development (see Behavior analysis of child development) to generate models for prevention as well as treatment for autism.
Pivotal response training
Pivotal response treatment (PRT) is a naturalistic intervention derived from ABA principles. Instead of individual behaviors, it targets pivotal areas of a child's development, such as motivation, responsivity to multiple cues, self-management, and social initiations; it aims for widespread improvements in areas that are not specifically targeted. The child determines activities and objects that will be used in a PRT exchange. Intended attempts at the target behavior are rewarded with a natural reinforcer: for example, if a child attempts a request for a stuffed animal, the child receives the animal, not a piece of candy or other unrelated reinforcer.[52]
Aversive therapy
The Judge Rotenberg Educational Center uses aversion therapy, notably contingent shock (electric shock delivered to the skin for a few seconds), to control the behavior of its patients, many of whom are autistic. The practice is controversial[53] and has not been popular or used elsewhere since the 1990s.
Communication interventions
The inability to communicate, verbally or non-verbally, is a core deficit in autism. Children with autism are often engaged in repetitive activity or other behaviors because they cannot convey their intent any other way. They do not know how to communicate their ideas to caregivers or others. Helping a child with autism learn to communicate their needs and ideas is absolutely core to any intervention. Communication can either be verbal or non-verbal. Children with autism require intensive intervention to learn how to communicate their intent.
Communication interventions fall into two major categories. First, many autistic children do not speak, or have little speech, or have difficulties in effective use of language.[54] Social skills have been shown to be effective in treating children with autism.[54] Interventions that attempt to improve communication are commonly conducted by speech and language therapists, and work on joint attention, communicative intent, and alternative or augmentative and alternative communication (AAC) methods such as visual methods,[55] for example visual schedules. AAC methods do not appear to impede speech and may result in modest gains.[56] A 2006 study reported benefits both for joint attention intervention and for symbolic play intervention,[57] and a 2007 study found that joint attention intervention is more likely than symbolic play intervention to cause children to engage later in shared interactions.[58]
Second, social skills treatment attempts to increase social and communicative skills of autistic individuals, addressing a core deficit of autism. A wide range of intervention approaches is available, including modeling and reinforcement, adult and peer mediation strategies, peer tutoring, social games and stories, self-management, pivotal response therapy, video modeling, direct instruction, visual cuing, Circle of Friends and social-skills groups.[59] A 2007 meta-analysis of 55 studies of school-based social skills intervention found that they were minimally effective for children and adolescents with ASD,[60] and a 2007 review found that social skills training has minimal empirical support for children with Asperger syndrome or high-functioning autism.[19]
SCERTS
The SCERTS model[61] is an educational model for working with children with autism spectrum disorder (ASD). It was designed to help families, educators and therapists work cooperatively together to maximize progress in supporting the child.
The acronym refers to the focus on:
- SC – social communication – the development of functional communication and emotional expression.
- ER – emotional regulation – the development of well-regulated emotions and ability to cope with stress.
- TS – transactional support – the implementation of supports to help families, educators and therapists respond to children's needs, adapt the environment and provide tools to enhance learning.
Computer-assisted therapy for reasoning about communicative actions
Many remediation strategies have not taken into account that people with autism suffer from difficulties in learning social rules from examples. Computer-assisted autism therapy has been proposed to teach not simply via examples but to teach the rule along with it.[62] A reasoning rehabilitation strategy, based on playing with a computer based mental simulator that is capable of modeling mental and emotional states of the real world, has been subject to short-term and long-term evaluations.[63] The simulator performs the reasoning in the framework of belief-desire-intention model. Learning starts from the basic concepts of knowledge and intention and proceeds to more complex communicative actions such as explaining, agreeing, and pretending.
Relationship based, developmental models
Relationship based models give importance to the relationships that help children reach and master early developmental milestones. These are often missed or not mastered in children with ASD. Examples of these early milestones are engagement and interest in the world, intimacy with a caregiver, intentionality of action.
Relationship Development Intervention
Relationship development intervention[64] is a family-based treatment program for children with autism spectrum disorder (ASD). This program is based on the belief that the development of dynamic intelligence (the ability to think flexibly, take different perspectives, cope with change and process information simultaneously) is key to improving the quality of life of children with autism.
Floortime/DIR
The Floortime/DIR (Developmental, Individual Differences based, Relationship based ) approach is a developmental intervention to autism developed by Stanley Greenspan and Serena Weider. This approach is based on the idea that the core deficits in autism are individual differences in the sensory system, motor planning problems, difficulties in communication and relation to others, and the inability to connect ones desire to intentional action and communication. When addressed through a combination of sensory support and DIR/Floortime techniques, the facilitator is playfully obstructive to redirect the child to play and relate to their therapist. The primary goal of Floortime is to improve the child's cognitive, language, and social abilities.[65] However, these claims should be regarded with some scepticism, owing to a lack of independent scientific research into the efficacy of the floortime approach.
The DIR model is based on the model of a developmental 'tree', the central notion being that Autistic children have yet to master certain early developmental milestones, or 'branches' of the tree, which are as follows:
- Stage One: Regulation and Interest in the World: Being calm and feeling well enough to attend to a caregiver and surroundings. Have shared attention.
- Stage Two: Engagement and Relating: Interest in another person and in the world, developing a special bond with preferred caregivers. Distinguishing inanimate objects from people.
- Stage Three: Two way intentional communication: Simple back and forth interactions between child and caregiver. Smiles, tickles, anticipatory play.
- Stage Four: Social Problem solving: Using gestures, interaction, babble to indicate needs, wants, pleasure, upset. Get a caregiver to help with a problem. Using pre-language skills to show intention.
- Stage Five: Symbolic Play: Using words, pictures, symbols to communicate an intention, idea. Communicate ideas and thoughts, not just wants and needs.
- Stage Six: Bridging Ideas: This stage is the foundation of logic, reasoning, emotional thinking and a sense of reality.
Exponents of the floortime approach argue that children with ASD struggle with or have missed some of these vital developmental stages. An introduction to DIR/Floortime can be found in the book - Engaging Autism: Using the Floortime Approach to Help Children Relate, Communicate, and Think, by Stanley Greenspan, M.D. and Serena Wieder, PhD.
The PLAY Project
The PLAY Project (an acronym for PLAY and Language for Autistic Youngsters) is a community-based, national autism training and early intervention program established in 2001 by Richard Solomon.[66] Based on the DIR (Developmental, Individualized, Relationship-based) theory of Stanley Greenspan MD, the program is designed to train parents and professionals to implement intensive, developmental interventions for young children (18 months to 6 years) with autism. The program is operating in nearly 100 agencies worldwide including 25 states and in 5 countries outside of the U.S. (Australia, Canada, England, Ireland and Switzerland). The PLAY Project has been operating since 2001 from its headquarters in Ann Arbor, MI.
Some preliminary research on the program was published by the peer-reviewed British journal, Autism [67] (May, 2007).
Son-Rise
Son-Rise is a home-based program that emphasizes on implementing a color- and sensory-free playroom. Before implementing the home-based program, an institute trains the parents how to accept their child without judgment through a series of dialogue sessions. Like Floortime, parents join their child's ritualistic behavior for relationship-building. To gain the child's "willing engagement", the facilitator continues to join them only this time through parallel play. Proponents claim that children will become non-autistic after parents accept them for who they are and engage them in play. The program was started by the parents of Raun Kaufman, who is claimed to have gone from being autistic to normal via the treatment in the early 1970s.[68] No independent study has tested the efficacy of the program, but a 2003 study found that involvement with the program led to more drawbacks than benefits for the involved families over time,[69] and a 2006 study found that the program is not always implemented as it is typically described in the literature, which suggests it will be difficult to evaluate its efficacy.[70]
TEACCH
Treatment and Education of Autistic and Related Communication Handicapped Children (TEACCH), which has come to be called "structured teaching", emphasises structure by using organized physical environments, predictably sequenced activities, visual schedules and visually structured activities, and structured work/activity systems where each child can practice various tasks.[2] Parents are taught to implement the treatment at home. A 1998 controlled trial found that children treated with a TEACCH-based home program improved significantly more than a control group.[71] A 2013 meta-analysis compiling all the clinical trials of TEACCH indicated that it has small or no effects on perceptual, motor, verbal, cognitive, and motor functioning, communication skills, and activities of daily living. There were positive effects in social and maladaptive behavior, but these required further replication due to the methodological limitations of the pool of studies analysed.[72]
Sensory integration
Unusual responses to sensory stimuli are more common and prominent in children with autism, although there is not good evidence that sensory symptoms differentiate autism from other developmental disorders.[73] Several therapies have been developed to treat Sensory processing disorder.[74] Some of these treatments (for example, sensorimotor handling) have a questionable rationale and have no empirical evidence. Other treatments have been studied, with small positive outcomes, but few conclusions can be drawn due to methodological problems with the studies. These treatments include prism lenses, physical exercise, auditory integration training, and sensory stimulation or inhibition techniques such as "deep pressure"—firm touch pressure applied either manually or via an apparatus such as a hug machine or a pressure garment.[75] Weighted vests, a popular deep-pressure therapy, have only a limited amount of scientific research available, which on balance indicates that the therapy is ineffective.[76] Although replicable treatments have been described and valid outcome measures are known, gaps exist in knowledge related to Sensory processing disorder and therapy.[77] In a 2011 Cochrane review, no evidence was found to support the use of auditory integration training as an ASD treatment method.[78] Because empirical support is limited, systematic evaluation is needed if these interventions are used.[79]
The term multisensory integration in simple terms means the ability to use all of ones senses to accomplish a task. Occupational therapists sometimes prescribe sensory treatments for children with Autism however in general there has been little or no scientific evidence of effectiveness.[75]
Animal-assisted therapy
Animal-assisted therapy, where an animal such as a dog or a horse becomes a basic part of a person's treatment, is a controversial treatment for some symptoms. A 2007 meta-analysis found that animal-assisted therapy is associated with a moderate improvement in autism spectrum symptoms.[80] Reviews of published dolphin-assisted therapy (DAT) studies have found important methodological flaws and have concluded that there is no compelling scientific evidence that DAT is a legitimate therapy or that it affords any more than fleeting improvements in mood.[81]
Neurofeedback
Neurofeedback attempts to train individuals to regulate their brainwave patterns by letting them observe their brain activity more directly. In its most traditional form, the output of EEG electrodes is fed into a computer that controls a game-like audiovisual display. Neurofeedback has been evaluated with positive results for ASD, but studies have lacked random assignment to controls.[82]
Patterning
Patterning is a set of exercises that attempts to improve the organization of a child's neurologic impairments. It has been used for decades to treat children with several unrelated neurologic disorders, including autism. The method, taught at The Institutes for the Achievement of Human Potential, is based on oversimplified theories and is not supported by carefully designed research studies.[83]
Packing
In packing, children are wrapped tightly for up to an hour in wet sheets that have been refrigerated, with only their heads left free. The treatment is repeated several times a week, and can continue for years. It is intended as treatment for autistic children who harm themselves; most of these children cannot speak. Similar envelopment techniques have been used for centuries, such as to calm violent patients in Germany in the 19th century; its modern use in France began in the 1960s, based on psychoanalytic theories such as the theory of the refrigerator mother. Packing is currently used in hundreds of French clinics. There is no scientific evidence for the effectiveness of packing, and some concern about risk of adverse health effects.[84]
Other methods
There are many simple methods such as priming, prompt delivery, picture schedules, peer tutoring, and cooperative learning, that have been proven to help autistic students to prepare for class and to understand the material better. Priming is done by allowing the students to see the assignment or material before they are shown in class. Prompt delivery consists of giving prompts to the autistic children in order to elicit a response to the academic material. Picture schedules are used to outline the progression of a class and are visual cues to allow autistic children to know when changes in the activity are coming up. This method has proven to be very useful in helping the students follow the activities. Peer tutoring and cooperative learning are ways in which an autistic student and a nonhandicapped student are paired together in the learning process. This has shown be very effective for “increasing both academic success and social interaction.”[85] There are more specific strategies that have been shown to improve an autistic’s education, such as LEAP, Treatment and Education of Autistic and Related Communication Handicapped Children, and Non-Model-Specific Special Education Programs for preschoolers. LEAP is “an intensive 12-month program that focuses on providing a highly structured and safe environment that helps students to participate in and derive benefit from educational programming” and focuses on children from 5-21 who have a more severe case of autism.[86] The goal of the program is to develop functional independence through academic instruction, vocational/translational curriculum, speech/language services, and other services personalized for each student.[86] While LEAP, TEACCH, and Non-Model Specific Special Education Programs are all different strategies, there has been no evidence that one is more effective than the other.[87]
Societal aspects
Martha Nussbaum discusses how education is one of the fertile functions that is important for the development of a person and their ability to achieve a multitude of other capabilities within society.[88] Autism causes many symptoms that interfere with a child’s ability to receive a proper education such as deficits in imitation, observational learning, and receptive and expressive communication. Of all disabilities affecting the population, autism ranks third lowest in acceptance into a postsecondary education institution.[89] In a study funded by the National Institute of Health, Shattuck et al. found that only 35% of autistics are enrolled in a 2 or 4 year college within the first two years after leaving high school compared to 40% of children who have a learning disability.[90] Due to the growing need for a college education to obtain a job, this statistic shows how autistics are at a disadvantage in gaining many of the capabilities that Nussbaum discusses and makes education more than just a type of therapy for those with autism.[89] According to the study by Shattuck, only 55% of children with autism participated in any paid employment within the first two years after high school. Furthermore, those with autism that come from low income families tend to have lower success in postsecondary schooling.[90] Due to these issues, education has become more than just an issue of therapy for those with autism but also a social issue.
Disadvantages
Oftentimes, schools simply lack the resources to create an optimal classroom setting for those in need of special education. In the United States, it can cost between $6595 to $10,421 extra to educate a child with autism.[91] In the 2011-2012 school year, the average cost of education for a public school student was $12,401. In some cases, the extra cost required to educate a child with autism nearly doubles the average cost to educate the average public school student.[92] As the range of those with autism can widely vary, it is very difficult to create an autism program that is well suited to the entire population of autistics as well as those with other disabilities. In the United States, many school districts are requiring schools to meet the needs of disabled students, regardless of the number of children with disabilities there are in the school.[93] This combined with a shortage of licensed special education teachers has created a deficiency in the special education system. The shortage has caused some states to give temporary special education licenses to teachers with the caveat that they receive a license within a few years.[94]
Policies
In the United States, there have been three major policies addressing special education in the United States. These policies were the Education for All Handicapped Children Act in 1975, the Individuals with Disabilities Education Act in 1997, and the No Child Left Behind in 2001. The development of these policies showed increased guidelines for special education and requirements; such as requiring states to fund special education, equality of opportunities, help with transitions after secondary schooling, requiring extra qualifications for special education teachers, and creating a more specific class setting for those with disabilities.[95][96][97] The Individuals with Disabilities Education Act, specifically had a large impact on special education as public schools were then required to employ high qualified staff. For one to be a Certified Autism Specialist, one must have a master's degree, two years of career experience working with the autism population, earn 14 continuing education hours in autism every two years, and register with the International Institute of Education.[98] In 1993, Mexico passed an education law that called for the inclusion of those with disabilities. This law was very important for Mexico education, however, there have been issues in implementing it due to a lack of resources.[99]
There have also been multiple international groups that have issued reports addressing issues in special education. The United Nations on “International Norms and Standards relating to Disability” in 1998. This report cites multiple conventions, statements, declarations, and other reports such as: The Universal Declaration of Human Rights, The Salamanca Statement, the Sundberg Declaration, the Copenhagen Declaration and Programme of Action, and many others. One main point that the report emphasizes is the necessity for education to be a human right. The report also states that the “quality of education should be equal to that of persons without disabilities.” The other main points brought up by the report discuss integrated education, special education classes as supplementary, teacher training, and equality for vocational education.[100] The United Nations also releases a report by the Special Rapporteur that has a focus on persons with disabilities. In 2015, a report titled “Report of the Special Rapporteur to the 52nd Session of the Commission for Social Development: Note by the Secretary-General on Monitoring of the implementation of the Standard Rules on the Equalization of Opportunities for Persons with Disabilities” was released. This report focused on looking at how the many countries involved, with a focus on Africa, have handled policy regarding persons with disabilities. In this discussion, the author also focuses on the importance of education for persons with disabilities as well as policies that could help improve the education system such as a move towards a more inclusive approach.[101] The World Health Organization has also published a report addressing people with disabilities and within this there is a discussion on education in their “World Report on Disability” in 201.[102] Other organizations that have issued reports discussing the topic are UNESCO, UNICEF, and the World Bank.[103]
Environmental enrichment
Environmental enrichment is concerned with how the brain is affected by the stimulation of its information processing provided by its surroundings (including the opportunity to interact socially). Brains in richer, more-stimulating environments, have increased numbers of synapses, and the dendrite arbors upon which they reside are more complex. This effect happens particularly during neurodevelopment, but also to a lesser degree in adulthood. With extra synapses there is also increased synapse activity and so increased size and number of glial energy-support cells. Capillary vasculation also is greater to provide the neurons and glial cells with extra energy. The neuropil (neurons, glial cells, capillaries, combined together) expands making the cortex thicker. There may also exist (at least in rodents) more neurons.
Research on nonhuman animals finds that more-stimulating environments could aid the treatment and recovery of a diverse variety of brain-related dysfunctions, including Alzheimer's disease and those connected to aging, whereas a lack of stimulation might impair cognitive development.
Research on humans suggests that lack of stimulation (deprivation—such as in old-style orphanages) delays and impairs cognitive development. Research also finds that higher levels of education (which is both cognitively stimulating in itself, and associates with people engaging in more challenging cognitive activities) results in greater resilience (cognitive reserve) to the effects of aging and dementia.
Massage therapy
A review of massage therapy as a symptomatic treatment of autism found limited evidence of benefit. There were few high quality studies, and due to the risk of bias found in the studies analyzed, no firm conclusions about the efficacy of massage therapy could be drawn.[104]
Music
Music therapy uses the elements of music to let people express their feelings and communicate. A 2014 review found that music therapy may help in social interactions and communication.[105]
Music therapy can involve various techniques depending on where the subject is sitting on the ASD scale. Somebody who may be considered as 'low-functioning' would require vastly different treatment to somebody on the ASD scale who is 'high-functioning'. Examples of these types of therapeutic techniques include:[106]
- Free improvisation - No boundaries or skills required
- Structured improvisation - Some established parameters within the music
- Performing or recreating music - Reproducing a pre-composed piece of music or song with associated activities
- Composing music - Creating music that caters to the specific needs of that person using instruments or the voice
- Listening - Engaging in specific musical listening base exercises
Improvisational Music Therapy (IMT), is increasing in popularity as a therapeutic technique being applied to children with ASD. The process of IMT occurs when the client and therapist make up music, through the use of various instruments, song and movement. The specific needs of each child or client need to be taken into consideration. Some children with ASD find their different environments chaotic and confusing, therefore, IMT sessions require the presence of a certain routine and be predictable in nature, within their interactions and surroundings.[107] Music can provide all of this, it can be very predicable, it is highly repetitious with its melodies and sounds, but easily varied with phrasing, rhythm and dynamics giving it a controlled flexibility. The allowance of parents or caregivers to sessions can put the child at ease and allow for activities to be incorporated into everyday life.[107]
Sensory enrichment therapy
In all interventions for autistic children, the main strategy is to aim towards the improvement on sensitivity in all senses. Autistic children suffer from a lack of the ability to derive and sort out their senses as well as the feelings and moods of the people around them.[1] Many children with autism suffer from this Sensory Processing Disorder.[2] In sensory-based interventions, there have been signs of progress in children responding with an appropriate response when given a stimulus after being in sensory-based therapies for a period of time. However, at this time, there is no concrete evidence that these therapies are effective for children with Autism.[2] Autism is a very complex disorder and differs from child to child. This makes the effectiveness of each type of therapy and even therapy activity vary.
The purpose of these differentiated interventions are to intervene at the neurological level of the brain in hopes to develop appropriate responses to the different sensations from one's body and also to outside stimuli in one's environment. Scientist have used music therapies, massage therapies, occupational therapies and more. With the Autistic Spectrum being so diverse and widespread, each case or scenario is different.[75]
Parent mediated interventions
Parent mediated interventions offer support and practical advice to parents of autistic children.[55] A 2002 Cochrane Review found only two relevant studies, with small numbers of participants, and no clinical recommendations could be made due to these limitations.[108] A very small number of randomized and controlled studies suggest that parent training can lead to reduced maternal depression, improved maternal knowledge of autism and communication style, and improved child communicative behavior, but due to the design and number of studies available, definitive evidence of effectiveness is not available.[109]
Early detection of ASD in children can often occur before a child reaches the age of three years old. Methods that target early behavior can influence the quality of life for a child with ASD. Parents can learn methods of interaction and behavior management to best assist their child's development. A 2013 Cochrance review concluded that there were some improvements when parent intervention was used.[110]
Medical management
Drugs, supplements, or diets are often used to alter physiology in an attempt to relieve common autistic symptoms such as seizures, sleep disturbances, irritability, and hyperactivity that can interfere with education or social adaptation or (more rarely) cause autistic individuals to harm themselves or others.[111] There is plenty of anecdotal evidence to support medical treatment; many parents who try one or more therapies report some progress, and there are a few well-publicized reports of children who are able to return to mainstream education after treatment, with dramatic improvements in health and well-being. However, this evidence may be confounded by improvements seen in autistic children who grow up without treatment, by the difficulty of verifying reports of improvements, and by the lack of reporting of treatments' negative outcomes.[112] Only a very few medical treatments are well supported by scientific evidence using controlled experiments.[111]
Prescription medication
Many medications are used to treat problems associated with ASD.[10] More than half of U.S. children diagnosed with ASD are prescribed psychoactive drugs or anticonvulsants, with the most common drug classes being antidepressants, stimulants, and antipsychotics.[11] Only the antipsychotics have clearly demonstrated efficacy.[12]
Research has focused on atypical antipsychotics, especially risperidone, which has the largest amount of evidence that consistently shows improvements in irritability, self-injury, aggression, and tantrums associated with ASD.[113] Risperidone is approved by the Food and Drug Administration (FDA) for treating symptomatic irritability in autistic children and adolescents.[12] In short-term trials (up to six months) most adverse events were mild to moderate, with weight gain, drowsiness, and high blood sugar requiring monitoring; long term efficacy and safety have not been fully determined.[114] It is unclear whether risperidone improves autism's core social and communication deficits.[12] The FDA's decision was based in part on a study of autistic children with severe and enduring problems of tantrums, aggression, and self-injury; risperidone is not recommended for autistic children with mild aggression and explosive behavior without an enduring pattern.[115]
Other drugs are prescribed off-label in the U.S., which means they have not been approved for treating ASD. Large placebo-controlled studies of olanzapine and aripiprazole were underway in early 2008.[12] Aripiprazole may be effective for treating autism in the short term, but is also associated with side effects, such as weight gain and sedation.[116] Some selective serotonin reuptake inhibitors (SSRIs) and dopamine blockers can reduce some maladaptive behaviors associated with ASD.[117] Although SSRIs reduce levels of repetitive behavior in autistic adults,[118] a 2009 multisite randomized controlled study found no benefit and some adverse effects in children from the SSRI citalopram, raising doubts whether SSRIs are effective for treating repetitive behavior in autistic children.[119] A further study of related medical reviews determined that the prescription of SSRI antidepressants for treating autistic spectrum disorders in children lacked any evidence, and could not be recommended.[120] Reviews of evidence found that the psychostimulant methylphenidate may be efficacious against hyperactivity and possibly impulsivity associated with ASD, although the findings were limited by low quality evidence.[121] There was no evidence that methylphenidate "has a negative impact on the core symptoms of ASD, or that it improves social interaction, stereotypical behaviours, or overall ASD."[121] Of the many medications studied for treatment of aggressive and self-injurious behavior in children and adolescents with autism, only risperidone and methylphenidate demonstrate results that have been replicated.[122] A 1998 study of the hormone secretin reported improved symptoms and generated tremendous interest, but several controlled studies since have found no benefit.[123] Oxytocin may play a role in autism and may be an effective treatment for repetitive and affiliative behaviors;[124] two related studies in adults found that oxytocin decreased repetitive behaviors and improved interpretation of emotions, but these preliminary results do not necessarily apply to children.[125] An experimental drug STX107 has stopped overproduction of metabotropic glutamate receptor 5 in rodents, and it has been hypothesized that this may help in about 5% of autism cases, but this hypothesis has not been tested in humans.[125]
Aside from antipsychotics,[12] there is scant reliable research about the effectiveness or safety of drug treatments for adolescents and adults with ASD.[13] Results of the handful of randomized controlled trials that have been performed suggest that risperidone, the SSRI fluvoxamine, and the typical antipsychotic haloperidol may be effective in reducing some behaviors, that haloperidol may be more effective than the tricyclic antidepressant clomipramine, and that the opioid antagonist naltrexone hydrochloride is not effective.[14] In small studies, memantine has been shown to significantly improve language function and social behavior in children with autism.[126][127] Research is underway on the effects of memantine in adults with autism spectrum disorders.[128] A person with ASD may respond atypically to medications and the medications can have adverse side effects.[15][129]
Dietary supplements
Many parents give their children dietary supplements in an attempt to treat autism or to alleviate its symptoms. The range of supplements given is wide; few are supported by scientific data, but most have relatively mild side effects.[18][111]
A review found some low-quality evidence to support the use of vitamin B6 in combination with magnesium at high doses, but the evidence was equivocal and the review noted the possible danger of fatal hypermagnesemia.[130] A Cochrane Review of the evidence for the use of B6 and magnesium found that "[d]ue to the small number of studies, the methodological quality of studies, and small sample sizes, no recommendation can be advanced regarding the use of B6-Mg as a treatment for autism."[131]
Dimethylglycine (DMG) is hypothesized to improve speech and reduce autistic behaviors,[18] and is a commonly used supplement.[111] Two double-blind, placebo-controlled studies found no statistically significant effect on autistic behaviors,[18] and reported few side effects. No peer-reviewed studies have addressed treatment with the related compound trimethylglycine.[111]
Vitamin C decreased stereotyped behavior in a small 1993 study.[132] The study has not been replicated, and vitamin C has limited popularity as an autism treatment. High doses might cause kidney stones or gastrointestinal upset such as diarrhea.[111]
Probiotics containing potentially beneficial bacteria are hypothesized to relieve some symptoms of autism by minimizing yeast overgrowth in the colon. The hypothesized yeast overgrowth has not been confirmed by endoscopy, the mechanism connecting yeast overgrowth to autism is only hypothetical, and no clinical trials to date have been published in the peer-reviewed literature. No negative side effects have been reported.[111]
Melatonin is sometimes used to manage sleep problems in developmental disorders. Adverse effects are generally reported to be mild, including drowsiness, headache, dizziness, and nausea; however, an increase in seizure frequency is reported among susceptible children.[18] Several small RCTs have indicated that melatonin is effective in treating insomnia in autistic children, but further large studies are needed.[133] A 2013 literature review found 20 studies that reported improvements in sleep parameters as a result of melatonin supplementation, and concluded that "the administration of exogenous melatonin for abnormal sleep parameters in ASD is evidence-based."[134]
Although omega-3 fatty acids, which are polyunsaturated fatty acids (PUFA), are a popular treatment for children with ASD, there is very little high-quality scientific evidence supporting their effectiveness,[135][136] and further research is needed.[2]
Several other supplements have been hypothesized to relieve autism symptoms, including BDTH2,[137] carnosine, cholesterol,[138] cyproheptadine, D-cycloserine, folic acid, glutathione, metallothionein promoters, other PUFA such as omega-6 fatty acids, tryptophan, tyrosine, thiamine (see Chelation therapy), vitamin B12, and zinc. These lack reliable scientific evidence of efficacy or safety in treatment of autism.[18][111]
Diets
Atypical eating behavior occurs in about three-quarters of children with ASD, to the extent that it was formerly a diagnostic indicator. Selectivity is the most common problem, although eating rituals and food refusal also occur;[139] this does not appear to result in malnutrition. Although some children with autism also have gastrointestinal (GI) symptoms, there is a lack of published rigorous data to support the theory that autistic children have more or different GI symptoms than usual;[140] studies report conflicting results, and the relationship between GI problems and ASD is unclear.[2]
In the early 1990s, it was hypothesized that autism can be caused or aggravated by opioid peptides like casomorphine that are metabolic products of gluten and casein.[141] Based on this hypothesis, diets that eliminate foods containing either gluten or casein, or both, are widely promoted, and many testimonials can be found describing benefits in autism-related symptoms, notably social engagement and verbal skills. Studies supporting these claims have had significant flaws, so these data are inadequate to guide treatment recommendations.[24][142]
Other elimination diets have also been proposed, targeting salicylates, food dyes, yeast, and simple sugars. No scientific evidence has established the efficacy of such diets in treating autism in children. An elimination diet may create nutritional deficiencies that harm overall health unless care is taken to assure proper nutrition.[18] For example, a 2008 study found that autistic boys on casein-free diets have significantly thinner bones than usual, presumably because the diets contribute to calcium and vitamin D deficiencies.[143]
Chelation therapy
Based on the speculation that heavy metal poisoning may trigger the symptoms of autism, particularly in small subsets of individuals who cannot excrete toxins effectively, some parents have turned to alternative medicine practitioners who provide detoxification treatments via chelation therapy. However, evidence to support this practice has been anecdotal and not rigorous. Strong epidemiological evidence refutes links between environmental triggers, in particular thiomersal-containing vaccines, and the onset of autistic symptoms. No scientific data supports the claim that the mercury in the vaccine preservative thiomersal causes autism[144] or its symptoms,[145] and there is no scientific support for chelation therapy as a treatment for autism.[146][147]
Thiamine tetrahydrofurfuryl disulfide (TTFD) is hypothesized to act as a chelating agent in children with autism. A 2002 pilot study administered TTFD rectally to ten autism spectrum children, and found beneficial clinical effect.[148] This study has not been replicated, and a 2006 review of thiamine by the same author did not mention thiamine's possible effect on autism.[149] There is not sufficient evidence to support the use of thiamine (vitamin B1) to treat autism.[18]
Chiropractic
Chiropractic is an alternative medical practice whose main hypothesis is that mechanical disorders of the spine affect general health via the nervous system, and whose main treatment is spinal manipulation. A significant portion of the profession rejects vaccination, as traditional chiropractic philosophy equates vaccines to poison.[150] Most chiropractic writings on vaccination focus on its negative aspects,[151] claiming that it is hazardous, ineffective, and unnecessary,[150] and in some cases suggesting that vaccination causes autism[151] or that chiropractors should be the primary contact for treatment of autism and other neurodevelopmental disorders.[152] Chiropractic treatment has not been shown to be effective for medical conditions other than back pain,[153] and there is insufficient scientific evidence to make conclusions about chiropractic care for autism.[154]
Craniosacral therapy
Craniosacral therapy is an alternative medical practice whose main hypothesis is that restrictions at cranial sutures of the skull affect rhythmic impulses conveyed via cerebrospinal fluid, and that gentle pressure on external areas can improve the flow and balance of the supply of this fluid to the brain, relieving symptoms of many conditions.[155] There is no scientific support for major elements of the underlying model,[156] there is little scientific evidence to support the therapy, and research methods that could conclusively evaluate the therapy's effectiveness have not been applied.[155] No published studies are available on the use of this therapy for autism.[17]
Electroconvulsive therapy
Studies indicate that 12–17% of adolescents and young adults with autism satisfy diagnostic criteria for catatonia, which is loss of or hyperactive motor activity. Electroconvulsive therapy (ECT) has been used to treat cases of catatonia and related conditions in people with autism. However, no controlled trials have been performed of ECT in autism, and there are serious ethical and legal obstacles to its use.[157]
Hyperbaric oxygen therapy

One small 2009 double-blind study of autistic children found that 40 hourly treatments of 24% oxygen at 1.3 atmospheres provided significant improvement in the children's behavior immediately after treatment sessions but this study has not been independently confirmed.[158] More recent, relatively large-scale controlled studies have also investigated HBOT using treatments of 24% oxygen at 1.3 atmospheres and have found less promising results. A 2010 double-blind study compared HBOT to a placebo treatment in children with autistic disorder. Both direct observational measures of behavioral symptoms and standardized psychological assessments were used to evaluate the treatment. No differences were found between the HBOT group and the placebo group on any of the outcome measures.[159] A second 2011 single-subject design study also investigated the effects of 40 HBOT treatments of 24% oxygen at 1.3 atmospheres on directly observed behaviors using multiple baselines across 16 participants. Again, no consistent outcomes were observed across any group and further, no significant improvements were observed within any individual participant.[160] Together these studies suggest that HBOT at 24% oxygen at 1.3 atmospheric pressure does not result in a clinically significant improvement of the behavioral symptoms of autistic disorder.
Nonetheless, news reports and related blogs indicate that HBOT is used for many cases of children with autism. HBOT can cost up to $150 per hour with individuals using anywhere from 40 to 120 hours as a part of their integrated treatment programs. In addition, purchasing (at $8,495–27,995) and renting ($1,395 per month) of the HBOT chambers is another option some families use.[160] When considering the financial and time investments required in order to participate in this treatment and the inconsistency of the present findings, HBOT seems to be a riskier and thus, often less favorable alternative treatment for autism. Further studies are needed in order for practitioners and families to make more conclusive and valid decisions concerning HBOT treatments.[161]
Prosthetics
Unlike conventional neuromotor prostheses, neurocognitive prostheses would sense or modulate neural function in order to physically reconstitute cognitive processes such as executive function and language. No neurocognitive prostheses are currently available but the development of implantable neurocognitive brain-computer interfaces has been proposed to help treat conditions such as autism.[162]
Affective computing devices, typically with image or voice recognition capabilities, have been proposed to help autistic individuals improve their social communication skills.[163] These devices are still under development. Robots have also been proposed as educational aids for autistic children.[164]
Transcranial magnetic stimulation
Transcranial magnetic stimulation, which is a somewhat well established treatment for depression, has been proposed, and used, as a treatment for autism.[165] A review published in 2013 found insufficient evidence to support its widespread use for autism spectrum disorders.[166] A 2015 review found tentative but insufficient evidence to justify its use outside of clinical studies.[167]
Stem cell therapy
Mesenchymal stem cells and cord blood CD34+ cells have been proposed to treat autism, but this proposal has not been tested.[168] They may represent a future treatment.[169] Since immune system deregulation has been implicated in autism, mesenchymal stem cells show the greatest promise as treatment for the disorder. Changes in the innate and adaptive immune system have been observed. Those with autism show an imbalance in CD3+, CD4+, and CD8+ T cells, as well as in NK cells.[170] In addition, peripheral blood mononuclear cells (PBMCs) overproduce IL-1β.[170] MSC mediated immune suppressive activity could restore this immune imbalance.
Alternative medicine
Acupuncture has not been found to be helpful.[171] A number of naturopathic practitioners claim that CEASE therapy, a mixture of homeopathy, supplements and 'vaccine detoxing', can help people with autism however no robust evidence is available for this.
Religious interventions
The Table Talk of Martin Luther contains the story of a twelve-year-old boy who some believe was severely autistic.[172] According to Luther's notetaker Mathesius, Luther thought the boy was a soulless mass of flesh possessed by the devil, and suggested that he be suffocated.[173] In 2003, an autistic boy in Wisconsin suffocated during an exorcism by an Evangelical minister in which he was wrapped in sheets.[174]
Ultraorthodox Jewish parents sometimes use spiritual and mystical interventions such as prayers, blessings, recitations of religious text, amulets, changing the child's name, and exorcism.[175]
One study has suggested that spirituality and not religious activities involving the mothers of autistic children were associated with better outcomes for the child.[176]
Anti-cure perspective
The exact cause of autism is unclear, yet some organizations advocate researching a cure. Some autism rights organizations view autism as a way of life rather than as a mental disorder and thus advocate acceptance over a search for a cure.[177][178]
Historical approach
Before autism was well understood, children in Britain and America would often be put in institutions on the instruction of doctors and the parents told to forget about them. Observer journalist Christopher Stevens, father of an autistic child, reports how a British doctor told him that after a child was admitted, usually "nature would take its course" and the child would die due to the prevalence of tuberculosis.[179]
Research
Environmental enrichment has found to be useful in animal models of autism.[180] Two human trials also found benefit in some children.[181][182]
Between the 1950s and 1970s LSD was studied, however, has not been studied since.[183]
See also
- Autism friendly
- Effects of equine assisted therapy on autism
- Ryan's Law
- Autism
- Special education
References
- Powell K. Opening a window to the autistic brain. PLOS Biology. 2004;2(8):E267. doi:10.1371/journal.pbio.0020267. PMID 15314667.
- Myers SM, Johnson CP, Council on Children with Disabilities. Management of children with autism spectrum disorders. Pediatrics. 2007;120(5):1162–82. doi:10.1542/peds.2007-2362. PMID 17967921.
- Ospina MB, Krebs Seida J, Clark B et al.. Behavioural and developmental interventions for autism spectrum disorder: a clinical systematic review. PLOS ONE. 2008;3(11):e3755. doi:10.1371/journal.pone.0003755. PMID 19015734. Bibcode: 2008PLoSO...3.3755O.
- Krebs Seida J, Ospina MB, Karkhaneh M, Hartling L, Smith V, Clark B. Systematic reviews of psychosocial interventions for autism: an umbrella review. Developmental Medicine & Child Neurology. 2009;51(2):95–104. doi:10.1111/j.1469-8749.2008.03211.x. PMID 19191842.
- Rogers SJ, Vismara LA. Evidence-based comprehensive treatments for early autism. Journal of Clinical Child & Adolescent Psychology. 2008;37(1):8–38. doi:10.1080/15374410701817808. PMID 18444052.
- Howlin P, Magiati I, Charman T. Systematic review of early intensive behavioral interventions for children with autism. American Journal on Intellectual and Developmental Disabilities. 2009;114(1):23–41. doi:10.1352/2009.114:23-41. PMID 19143460.
- Eikeseth S. Outcome of comprehensive psycho-educational interventions for young children with autism. Research in Developmental Disabilities. 2009;30(1):158–78. doi:10.1016/j.ridd.2008.02.003. PMID 18385012.
- Kanne SM, Randolph JK, Farmer JE. Diagnostic and assessment findings: a bridge to academic planning for children with autism spectrum disorders. Neuropsychology Review. 2008;18(4):367–84. doi:10.1007/s11065-008-9072-z. PMID 18855144.
- Van Bourgondien ME, Reichle NC, Schopler E. Effects of a model treatment approach on adults with autism. Journal of Autism and Developmental Disorders. 2003;33(2):131–40. doi:10.1023/A:1022931224934. PMID 12757352.
- Leskovec TJ, Rowles BM, Findling RL. Pharmacological treatment options for autism spectrum disorders in children and adolescents. Harvard Review of Psychiatry. 2008;16(2):97–112. doi:10.1080/10673220802075852. PMID 18415882.
- Medications for U.S. children with ASD:
- Oswald DP, Sonenklar NA. Medication use among children with autism spectrum disorders. Journal of Child and Adolescent Psychopharmacology. 2007;17(3):348–55. doi:10.1089/cap.2006.17303. PMID 17630868.
- Mandell DS, Morales KH, Marcus SC, Stahmer AC, Doshi J, Polsky DE. Psychotropic medication use among Medicaid-enrolled children with autism spectrum disorders. Pediatrics. 2008;121(3):e441–8. doi:10.1542/peds.2007-0984. PMID 18310165.
- Posey DJ, Stigler KA, Erickson CA, McDougle CJ. Antipsychotics in the treatment of autism. Journal of Clinical Investigation. 2008;118(1):6–14. doi:10.1172/JCI32483. PMID 18172517. PMC 2171144.
- Angley M, Young R, Ellis D, Chan W, McKinnon R. Children and autism—part 1—recognition and pharmacological management. Australian Family Physician. 2007 [archived 2007-10-25];36(9):741–4. PMID 17915375.
- Broadstock M, Doughty C, Eggleston M. Systematic review of the effectiveness of pharmacological treatments for adolescents and adults with autism spectrum disorder. Autism. 2007;11(4):335–48. doi:10.1177/1362361307078132. PMID 17656398.
- Buitelaar JK (2003). "Why have drug treatments been so disappointing?". Autism: Neural Basis and Treatment Possibilities. Novartis Foundation Symposia. 251. pp. 235–44, discussion 245–9, 281–97. doi:10.1002/0470869380.ch14. ISBN 9780470850992. PMID 14521196.
- Mash, E. J., & Wolfe, D. A. (2016). Abnormal Child Psychology (6th ed.)(pp.181-182). Boston, MA: Cengage Learning.
- Levy SE, Hyman SL. Complementary and alternative medicine treatments for children with autism spectrum disorders. Child and Adolescent Psychiatric Clinics of North America. 2008;17(4):803–20, ix. doi:10.1016/j.chc.2008.06.004. PMID 18775371.
- Angley M, Semple S, Hewton C, Paterson F, McKinnon R. Children and autism—part 2—management with complementary medicines and dietary interventions. Australian Family Physician. 2007 [archived 2007-12-01];36(10):827–30. PMID 17925903.
- Rao PA, Beidel DC, Murray MJ. Social skills interventions for children with Asperger's syndrome or high-functioning autism: a review and recommendations. Journal of Autism and Developmental Disorders. 2008;38(2):353–61. doi:10.1007/s10803-007-0402-4. PMID 17641962.
- Schechtman MA. Scientifically unsupported therapies in the treatment of young children with autism spectrum disorders. Pediatric Annals. 2007;36(8):497–8, 500–2, 504–5. doi:10.3928/0090-4481-20070801-12. PMID 17849608.
- Lack of support for interventions:
- Howlin P. The effectiveness of interventions for children with autism. In: Fleischhacker WW, Brooks DJ. Neurodevelopmental Disorders. Springer; 2005. doi:10.1007/3-211-31222-6_6. ISBN 3-211-26291-1. p. 101–19.
- Sigman M, Spence SJ, Wang AT. Autism from developmental and neuropsychological perspectives. Annual Review of Clinical Psychology. 2006;2:327–55. doi:10.1146/annurev.clinpsy.2.022305.095210. PMID 17716073.
- Williams White S, Keonig K, Scahill L. Social skills development in children with autism spectrum disorders: a review of the intervention research. Journal of Autism and Developmental Disorders. 2007;37(10):1858–68. doi:10.1007/s10803-006-0320-x. PMID 17195104.
- Burgess AF, Gutstein SE. Quality of life for people with autism: raising the standard for evaluating successful outcomes. Child and Adolescent Mental Health. 2007;12(2):80–6. doi:10.1111/j.1475-3588.2006.00432.x.
- Stahmer AC, Collings NM, Palinkas LA. Early intervention practices for children with autism: descriptions from community providers. Focus on Autism and Other Developmental Disabilities. 2005;20(2):66–79. doi:10.1177/10883576050200020301. PMID 16467905.
- Christison GW, Ivany K. Elimination diets in autism spectrum disorders: any wheat amidst the chaff?. Journal of Developmental and Behavioral Pediatrics. 2006;27(2 Suppl 2):S162–71. doi:10.1097/00004703-200604002-00015. PMID 16685183.
- Hazards of chelation therapy:
- Brown MJ, Willis T, Omalu B, Leiker R. Deaths resulting from hypocalcemia after administration of edetate disodium: 2003–2005. Pediatrics. 2006;118(2):e534–6. doi:10.1542/peds.2006-0858. PMID 16882789.
- Baxter AJ, Krenzelok EP. Pediatric fatality secondary to EDTA chelation. Clinical Toxicology. 2008;46(10):1083–4. doi:10.1080/15563650701261488. PMID 18949650.
- Shimabukuro TT, Grosse SD, Rice C. Medical expenditures for children with an autism spectrum disorder in a privately insured population. Journal of Autism and Developmental Disorders. 2008;38(3):546–52. doi:10.1007/s10803-007-0424-y. PMID 17690969.
- Federal Reserve Bank of Minneapolis. "Consumer Price Index (estimate) 1800–". Retrieved January 2, 2019.
- Ganz ML. The lifetime distribution of the incremental societal costs of autism. Archives of Pediatrics & Adolescent Medicine. 2007;161(4):343–9. doi:10.1001/archpedi.161.4.343. PMID 17404130.
- Knapp M, Romeo R, Beecham J. Economic cost of autism in the UK. Autism. 2009;13(3):317–36. doi:10.1177/1362361309104246. PMID 19369391.
- UK Retail Price Index inflation figures are based on data from Clark, Gregory (2017). "The Annual RPI and Average Earnings for Britain, 1209 to Present (New Series)". MeasuringWorth. Retrieved January 27, 2019.
- Aman MG. Treatment planning for patients with autism spectrum disorders. The Journal of Clinical Psychiatry. 2005;66(Suppl 10):38–45. PMID 16401149.
- Sharpe DL, Baker DL. Financial issues associated with having a child with autism. Journal of Family and Economic Issues. 2007;28(2):247–64. doi:10.1007/s10834-007-9059-6.
- Montes G, Halterman JS. Association of childhood autism spectrum disorders and loss of family income. Pediatrics. 2008;121(4):e821–6. doi:10.1542/peds.2007-1594. PMID 18381511.
- Montes G, Halterman JS. Child care problems and employment among families with preschool-aged children with autism in the United States. Pediatrics. 2008;122(1):e202–8. doi:10.1542/peds.2007-3037. PMID 18595965.
- Social Signals – Mike's Crush. American Journal of Sexuality Education. September 2012;7(3).
- Case-Smith J, Arbesman M. Evidence-based review of interventions for autism used in or of relevance to occupational therapy. American Journal of Occupational Therapy. 2008;62(4):416–29. doi:10.5014/ajot.62.4.416. PMID 18712004.
- Rickards AL, Walstab JE, Wright-Rossi RA, Simpson J, Reddihough DS. A randomized, controlled trial of a home-based intervention program for children with autism and developmental delay. Journal of Developmental & Behavioral Pediatrics. 2007;28(4):308–16. doi:10.1097/DBP.0b013e318032792e. PMID 17700083.
- Wheeler D, Williams K, Seida J, Ospina M. The Cochrane Library and Autism Spectrum Disorder: an overview of reviews. Evidence-Based Child Health. 2008 [archived 2012-12-10];3(1):3–15. doi:10.1002/ebch.218.
- Moore TR, Symons FJ. Adherence to behavioral and medical treatment recommendations by parents of children with autism spectrum disorders. Journal of Autism and Developmental Disorders. 2009;39(8):1173–84. doi:10.1007/s10803-009-0729-0. PMID 19333747.
- Dillenburger K, Keenan M. None of the As in ABA stand for autism: dispelling the myths. Journal of Intellectual & Developmental Disability. 2009;34(2):193–5. doi:10.1080/13668250902845244. PMID 19404840.
- Howard JS, Sparkman CR, Cohen HG, Green G, Stanislaw H. A comparison of intensive behavior analytic and eclectic treatments for young children with autism. Research in Developmental Disabilities. 2005;26(4):359–83. doi:10.1016/j.ridd.2004.09.005. PMID 15766629.
- Steege MW, Mace FC, Perry L, Longenecker H. Applied behavior analysis: beyond discrete trial teaching. Psychology in the Schools. 2007;44(1):91–9. doi:10.1002/pits.20208.
- Network, Autistic Self Advocacy. "Autistic Self Advocacy Network - Nothing About Us Without Us". www.autisticadvocacy.org.
- DeVita-Raeburn, Elizabeth (2016-08-11). "Is the Most Common Therapy for Autism Cruel?".
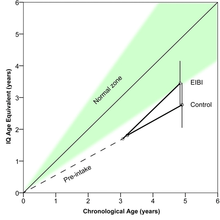
- Narrowing the gap: Effects of intervention on developmental trajectories in autism. Autism. 2015-01-01;19(1):53–63. en. doi:10.1177/1362361313510067. PMID 24212258.
- Ryan Carolyn S., Hemmes Nancy S.. Post-training Discrete-Trial Teaching Performance by Instructors of Young Children with Autism in Early Intensive Behavioral Intervention. The Behavior Analyst Today. 2005;6(1):1–16. doi:10.1037/h0100052.
- Weiss M.J, Delmolino L.. The Relationship Between Early Learning Rates and Treatment Outcome For Children With Autism Receiving Intensive Home-Based Applied Behavior Analysis. The Behavior Analyst Today. 2006;7(1):96–100. doi:10.1037/h0100140.
- Reichow B, Wolery M. Comprehensive synthesis of early intensive behavioral interventions for young children with autism based on the UCLA Young Autism Project model. Journal of Autism and Developmental Disorders. 2009;39(1):23–41. doi:10.1007/s10803-008-0596-0. PMID 18535894.
- Eldevik S, Hastings RP, Hughes JC, Jahr E, Eikeseth S, Cross S. Meta-analysis of Early Intensive Behavioral Intervention for children with autism. Journal of Clinical Child & Adolescent Psychology. 2009;38(3):439–50. doi:10.1080/15374410902851739. PMID 19437303.
- Spreckley M, Boyd R. Efficacy of applied behavioral intervention in preschool children with autism for improving cognitive, language, and adaptive behavior: a systematic review and meta-analysis. The Journal of Pediatrics. 2009;154(3):338–44. doi:10.1016/j.jpeds.2008.09.012. PMID 18950798.
- Jacobson J. W.. Converting to a Behavior Analysis Format for Autism Services: Decision-Making for Educational Administrators, Principals, and Consultants. The Behavior Analyst Today. 2000;1(3):6–16. doi:10.1037/h0099889.
- Pivotal response therapy:
- Koegel RL, Koegel LK. Pivotal Response Treatments for Autism: Communication, Social, & Academic Development. Brookes; 2006. ISBN 1-55766-819-1.
- Koegel LK, Koegel RL, Harrower JK, Carter CM. Pivotal response intervention I: overview of approach. Journal of the Association for Persons with Severe Handicaps. 1999;24(3):174–85. doi:10.2511/rpsd.24.3.174.
- Gonnerman J. School of shock. Mother Jones. 2007 [Retrieved 2008-10-19];32(5).
- Gillis J.M., Butler R.C.. Social skills interventions for preschoolers with Autism Spectrum Disorder: A description of single - subject design studies. Journal of Early and Intensive Behavior Intervention. 2007;4(3):532–548. doi:10.1037/h0100390.
- Scottish Intercollegiate Guidelines Network (SIGN). Assessment, diagnosis and clinical interventions for children and young people with autism spectrum disorders. 2007 [archived 7 April 2008; Retrieved 2008-04-02].
- Schlosser RW, Wendt O. Effects of augmentative and alternative communication intervention on speech production in children with autism: a systematic review. American Journal of Speech-Language Pathology. 2008;17(3):212–30. doi:10.1044/1058-0360(2008/021). PMID 18663107.
- Kasari C, Freeman S, Paparella T. Joint attention and symbolic play in young children with autism: a randomized controlled intervention study. Journal of Child Psychology and Psychiatry. 2006;47(6):611–20. doi:10.1111/j.1469-7610.2005.01567.x. PMID 16712638. Erratum. Journal of Child Psychology and Psychiatry. 2007;48(5):523. doi:10.1111/j.1469-7610.2007.01768.x. "no"
- Gulsrud AC, Kasari C, Freeman S, Paparella T. Children with autism's response to novel stimuli while participating in interventions targeting joint attention or symbolic play skills. Autism. 2007;11(6):535–46. doi:10.1177/1362361307083255. PMID 17947289.
- Matson JL, Matson ML, Rivet TT. Social-skills treatments for children with autism spectrum disorders: an overview. Behavior Modification. 2007;31(5):682–707. doi:10.1177/0145445507301650. PMID 17699124.
- Bellini S, Peters JK, Benner L, Hopf A. A meta-analysis of school-based social skills interventions for children with autism spectrum disorders. Remedial and Special Education. 2007;28(3):153–62. doi:10.1177/07419325070280030401.
- Barry M. Prizant; et al. (2005). The SCERTS manual : a comprehensive educational approach for young children with autism spectrum disorders. Baltimore, Md.: Paul H. Brookes. ISBN 978-1-55766-818-9.
- Galitsky B. A computational simulation tool for training autistic reasoning about mental attitudes. Knowledge-Based Systems. 2013;50:25–43. doi:10.1016/j.knosys.2013.04.018.
- Galitsky B. Exhaustive simulation of consecutive mental states of human agents. Knowledge-Based Systems. 2012;41(3):1–20. doi:10.1016/j.knosys.2012.11.001.
- Evaluation of the Relationship Development Intervention Program. Autism. 1 September 2007;11(5):397–411. doi:10.1177/1362361307079603. PMID 17942454.
- Tarbox, Jonathan (2014). Handbook of Early Intervention for Autism Spectrum Disorders. Springer Science+Business Media. p. 411. ISBN 9781493904013.
- "Richard Solomon, MD Founder of the P.L.A.Y. Project". Archived from the original on 2011-05-14. Retrieved 2011-05-05.
- Solomon R., Necheles J., Ferch C., Bruckman D.. Pilot study of a parent training program for young children with autism. Autism. 2007;11(3):205–224. doi:10.1177/1362361307076842. PMID 17478575.
- Kaufman BN. Son-Rise: the Miracle Continues. HJ Kramer; 1995. ISBN 0-915811-61-8.
- Williams KR, Wishart JG. The Son-Rise Program intervention for autism: an investigation into family experiences. Journal of Intellectual Disability Research. 2003;47(4–5):291–9. doi:10.1046/j.1365-2788.2003.00491.x. PMID 12787161.
- Williams KR. The Son-Rise Program intervention for autism: prerequisites for evaluation. Autism. 2006;10(1):86–102. doi:10.1177/1362361306062012. PMID 16522712.
- Ozonoff S, Cathcart K. Effectiveness of a home program intervention for young children with autism. Journal of Autism and Developmental Disorders. 1998;28(1):25–32. doi:10.1023/A:1026006818310. PMID 9546299.
- The TEACCH program for children and adults with autism: A meta-analysis of intervention studies. Clinical Psychology Review. 2013;33(8):940–953. doi:10.1016/j.cpr.2013.07.005. PMID 23988454.
- Rogers SJ, Ozonoff S. Annotation: what do we know about sensory dysfunction in autism? A critical review of the empirical evidence. Journal of Child Psychology and Psychiatry. 2005;46(12):1255–68. doi:10.1111/j.1469-7610.2005.01431.x. PMID 16313426.
- Research Autism. Sensory integrative therapy [Retrieved 2007-10-08].
- Baranek GT. Efficacy of sensory and motor interventions for children with autism. Journal of Autism and Developmental Disorders. 2002;32(5):397–422. doi:10.1023/A:1020541906063. PMID 12463517.
- Stephenson J, Carter M. The use of weighted vests with children with autism spectrum disorders and other disabilities. Journal of Autism and Developmental Disorders. 2009;39(1):105–14. doi:10.1007/s10803-008-0605-3. PMID 18592366.
- Schaaf RC, Miller LJ. Occupational therapy using a sensory integrative approach for children with developmental disabilities. Mental Retardation and Developmental Disabilities Research Reviews. 2005;11(2):143–8. doi:10.1002/mrdd.20067. PMID 15977314.
- Auditory integration training and other sound therapies for autism spectrum disorders (ASD).. Cochrane Database of Systematic Reviews. 7 December 2011;(12):CD003681. doi:10.1002/14651858.CD003681.pub3. PMID 22161380.
- Hodgetts S, Hodgetts W. Somatosensory stimulation interventions for children with autism: literature review and clinical considerations. Canadian Journal of Occupational Therapy. 2007;74(5):393–400. doi:10.2182/cjot.07.013. PMID 18183774.
- Nimer J, Lundahl B. Animal-assisted therapy: a meta-analysis. Anthrozoös. 2007;20(3):225–38. doi:10.2752/089279307X224773.
- Marino L, Lilienfeld SO. Dolphin-Assisted Therapy: more flawed data and more flawed conclusions. Anthrozoös. 2007 [archived 2008-02-28; Retrieved 2008-02-20];20(3):239–49. doi:10.2752/089279307X224782.
- Coben R, Linden M, Myers TE. Neurofeedback for autistic spectrum disorder: a review of the literature. Applied Psychophysiology and Biofeedback. 2010;35(1):83–105. doi:10.1007/s10484-009-9117-y. PMID 19856096.
- American Academy of Pediatrics. Committee on Children with Disabilities. The treatment of neurologically impaired children using patterning. Pediatrics. 1999;104(5):1149–51. doi:10.1542/peds.104.5.1149. PMID 10545565.
- Spinney L. Therapy for autistic children causes outcry in France. The Lancet. 2007;370(9588):645–6. doi:10.1016/S0140-6736(07)61322-1. PMID 17726792.
- Including Children with Autism in General Education Classrooms. Behavior Modification. 2001;25(5):762–784. doi:10.1177/0145445501255006. PMID 11573339.
- "LEAP Program (Lifeskills and Education for Students with Autism and Other Pervasive Behavioral Challenges)." Kennedy Krieger Institute: Unlocking Potential. 2012. Accessed November 1, 2015.
- Comparative Efficacy of LEAP, TEACCH and Non-Model-Specific Special Education Programs for Preschoolers with Autism Spectrum Disorders. Journal of Autism and Developmental Disorders. 2014;44(2):366–380. doi:10.1007/s10803-013-1877-9. PMID 23812661.
- Nussbaum, Martha (2009). Creating Capabilities: The Human Development Approach. Belknap Press of Harvard University Press. pp. 17–45. ISBN 9780674072350.
- Addressing the Academic Needs of Adolescents With Autism Spectrum Disorder in Secondary Education. Remedial and Special Education. 2014-03-01;35(2):68–79. doi:10.1177/0741932513518823.
- Postsecondary Education and Employment Among Youth With an Autism Spectrum Disorder. Pediatrics. 2012-06-01;129(6):1042–1049. doi:10.1542/peds.2011-2864. PMID 22585766.
- Economic Burden of Childhood Autism Spectrum Disorders. Pediatrics. 2014-03-01;133(3):–520–e529. doi:10.1542/peds.2013-0763. PMID 24515505.
- "The Condition of Education 2015". 2015-05-28. Retrieved 2015-11-10.
- Wall, Patrick (2014-08-11). "Special-education overhaul leaves students less isolated, but schools struggle to keep up". Chalkbeat New York. Retrieved 2015-11-10.
- "The Need Grows for Special Education Teachers in the U.S." CFNC. 2011. Retrieved 2015-11-10.
- Education for All Handicapped Children’s Act of 1975
- Individuals with Disabilities Education Act of 1997
- No Child Left Behind Act of 2001
- Standards.http://www.iies.us/
- Tuman, John P.; Roth-Johnson, Danielle; Baker, Dana Lee; Vecchio, Jennifer (2010-03-26). Autism and Special Education Policy in Mexico. SSRN 1578963.
- "UN Enable - Compilation of International Norms And Standards Relating to Disability". United Nations Enable. July 2002. Retrieved 2015-11-10.
- "Special Rapporteur on Disability of the Commission for Social Development". 2015. Archived from the original on 2015-07-07. Retrieved 2015-11-10.
- World report on disability. World Health Organization, World Bank (eds.). Geneva, Switzerland: World Health Organization. 2011. ISBN 978-92-4-156418-2.CS1 maint: others (link)
- "Global Reports". Retrieved 2015-11-10.
- Massage therapy for children with autism spectrum disorders: a systematic review. The Journal of Clinical Psychiatry. Mar 2011;72(3):406–11. doi:10.4088/JCP.09r05848whi. PMID 21208598.
- Music therapy for people with autism spectrum disorder.. Cochrane Database of Systematic Reviews. 17 June 2014;(6):CD004381. doi:10.1002/14651858.CD004381.pub3. PMID 24936966.
- Music therapy for individuals with autism spectrum disorder: A systematic review.. Review Journal of Autism and Developmental Disorders. 2015;2(1):39–54. doi:10.1007/s40489-014-0035-4.
- Common characteristics of improvisational approaches in music therapy for children with autism spectrum disorder: Developing treatment guidelines. Journal of Music Therapy. 2015;52(2):258–281. doi:10.1093/jmt/thv005. PMID 26019303.
- Diggle TT J, McConachie HH R.. Parent-mediated early intervention for young children with autism spectrum disorder. Cochrane Database of Systematic Reviews. 2003;(2). doi:10.1002/14651858.CD003496. (Retracted, see doi:10.1002/14651858.cd003496.pub2. If this is an intentional citation to a retracted paper, please replace
{{Retracted}}with{{Retracted|intentional=yes}}.) - McConachie H, Diggle T. Parent implemented early intervention for young children with autism spectrum disorder: a systematic review. Journal of Evaluation in Clinical Practice. 2007;13(1):120–9. doi:10.1111/j.1365-2753.2006.00674.x. PMID 17286734.
- Parent-mediated early intervention for young children with autism spectrum disorders (ASD).. Cochrane Database of Systematic Reviews. 30 April 2013;4(4):CD009774. doi:10.1002/14651858.CD009774.pub2. PMID 23633377.
- Levy SE, Hyman SL. Novel treatments for autistic spectrum disorders. Mental Retardation and Developmental Disabilities Research Reviews. 2005;11(2):131–42. doi:10.1002/mrdd.20062. PMID 15977319.
- Schreibman L. The Science and Fiction of Autism. Harvard University Press; 2005. ISBN 0-674-01931-8. Critical evaluation of issues in autism.
- Chavez B, Chavez-Brown M, Sopko MA Jr, Rey JA. Atypical antipsychotics in children with pervasive developmental disorders. Pediatric Drugs. 2007;9(4):249–66. doi:10.2165/00148581-200709040-00006. PMID 17705564.
- Scott LJ, Dhillon S. Risperidone: a review of its use in the treatment of irritability associated with autistic disorder in children and adolescents. Paediatric Drugs. 2007;9(5):343–54. doi:10.2165/00148581-200709050-00006. PMID 17927305.
- Scahill L. How do I decide whether or not to use medication for my child with autism? should I try behavior therapy first?. Journal of Autism and Developmental Disorders. 2008;38(6):1197–8. doi:10.1007/s10803-008-0573-7. PMID 18463973.
- Aripiprazole for autism spectrum disorders (ASD).. Cochrane Database of Systematic Reviews. 26 June 2016;(6):CD009043. doi:10.1002/14651858.CD009043.pub3. PMID 27344135.
- Myers SM. The status of pharmacotherapy for autism spectrum disorders. Expert Opinion on Pharmacotherapy. 2007;8(11):1579–603. doi:10.1517/14656566.8.11.1579. PMID 17685878.
- Volkmar FR. Citalopram treatment in children with autism spectrum disorders and high levels of repetitive behavior. Archives of General Psychiatry. 2009;66(6):581–2. doi:10.1001/archgenpsychiatry.2009.42. PMID 19487622.
- King BH, Hollander E, Sikich L et al.. Lack of efficacy of citalopram in children with autism spectrum disorders and high levels of repetitive behavior: citalopram ineffective in children with autism. Archives of General Psychiatry. 2009;66(6):583–90. doi:10.1001/archgenpsychiatry.2009.30. PMID 19487623.
- Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD). Cochrane Database of Systematic Reviews. 2013-08-20;8(8):CD004677. doi:10.1002/14651858.CD004677.pub3. PMID 23959778.
- Methylphenidate for children and adolescents with autism spectrum disorder. Cochrane Database of Systematic Reviews. 2017-11-21;11:CD011144. en. doi:10.1002/14651858.CD011144.pub2. PMID 29159857.
- Parikh MS, Kolevzon A, Hollander E. Psychopharmacology of aggression in children and adolescents with autism: a critical review of efficacy and tolerability. Journal of Child and Adolescent Psychopharmacology. 2008;18(2):157–78. doi:10.1089/cap.2007.0041. PMID 18439113.
- Francis K. Autism interventions: a critical update [PDF]. Developmental Medicine & Child Neurology. 2005;47(7):493–9. doi:10.1017/S0012162205000952. PMID 15991872.
- Bartz JA, Hollander E (2008). "Oxytocin and experimental therapeutics in autism spectrum disorders". Advances in Vasopressin and Oxytocin — from Genes to Behaviour to Disease. Progress in Brain Research. 170. pp. 451–62. doi:10.1016/S0079-6123(08)00435-4. ISBN 9780444532015. PMID 18655901.
- Opar A. Search for potential autism treatments turns to 'trust hormone'. Nature Medicine. 2008;14(4):353. doi:10.1038/nm0408-353. PMID 18391923.
- Memantine as adjunctive therapy in children diagnosed with autistic spectrum disorders: an observation of initial clinical response and maintenance tolerability. Journal of Child Neurology. May 2007;22(5):574–9. doi:10.1177/0883073807302611. PMID 17690064.
- A retrospective study of memantine in children and adolescents with pervasive developmental disorders. Psychopharmacology. March 2007;191(1):141–7. doi:10.1007/s00213-006-0518-9. PMID 17016714.
- "A Study of Memantine Hydrochloride (Namenda®) for Cognitive and Behavioral Impairment in Adults With Autism Spectrum Disorders".
- Strock M. Autism spectrum disorders (pervasive developmental disorders). 2007 [archived 2007-10-04; Retrieved 2007-10-05].
- Novel and emerging treatments for autism spectrum disorders: a systematic review. Annals of Clinical Psychiatry. 2009 [archived 2015-07-15];21(4):213–236. PMID 19917212.
- Combined vitamin B6-magnesium treatment in autism spectrum disorder. Cochrane Database of Systematic Reviews. 2005;(4):CD003497. doi:10.1002/14651858.CD003497.pub2. PMID 16235322.
- A preliminary trial of ascorbic acid as supplemental therapy for autism. Progress in Neuro-Psychopharmacology and Biological Psychiatry. 1993;17(5):765–774. doi:10.1016/0278-5846(93)90058-Z. PMID 8255984.
- A Practice Pathway for the Identification, Evaluation, and Management of Insomnia in Children and Adolescents With Autism Spectrum Disorders. Pediatrics. 1 November 2012;130(Supplement):S106–S124. doi:10.1542/peds.2012-0900I. PMID 23118242.
- Melatonin in Autism Spectrum Disorders. Current Clinical Pharmacology. 2013;9(4):326–34. doi:10.2174/15748847113086660072. PMID 24050742.
- Bent S, Bertoglio K, Hendren RL. Omega-3 fatty acids for autistic spectrum disorder: a systematic review. Journal of Autism and Developmental Disorders. 2009;39(8):1145–54. doi:10.1007/s10803-009-0724-5. PMID 19333748.
- Omega-3 fatty acids supplementation for autism spectrum disorders (ASD). Cochrane Database of Systematic Reviews. 2011;(11):CD007992. doi:10.1002/14651858.CD007992.pub2. PMID 22071839.
- Tsouderos T. OSR#1: industrial chemical or autism treatment? Chicago Tribune. 2010-01-17 [archived 2010-02-21; Retrieved 2010-02-11].
- Aneja A, Tierney E. Autism: The role of cholesterol in treatment. International Review of Psychiatry. 2008;20(2):165–70. doi:10.1080/09540260801889062. PMID 18386207.
- Dominick KC, Davis NO, Lainhart J, Tager-Flusberg H, Folstein S. Atypical behaviors in children with autism and children with a history of language impairment. Research in Developmental Disabilities. 2007;28(2):145–62. doi:10.1016/j.ridd.2006.02.003. PMID 16581226.
- Erickson CA, Stigler KA, Corkins MR, Posey DJ, Fitzgerald JF, McDougle CJ. Gastrointestinal factors in autistic disorder: a critical review. Journal of Autism and Developmental Disorders. 2005;35(6):713–27. doi:10.1007/s10803-005-0019-4. PMID 16267642.
- Reichelt KL, Knivsberg A-M, Lind G, Nødland M. Probable etiology and possible treatment of childhood autism. 1991;4:308–19.
- Millward C, Ferriter M, Calver S, Connell-Jones G. Gluten- and casein-free diets for autistic spectrum disorder. Cochrane Database of Systematic Reviews. 2008;(2):CD003498. doi:10.1002/14651858.CD003498.pub3. PMID 18425890. (Retracted, see doi:10.1002/14651858.cd003498.pub4. If this is an intentional citation to a retracted paper, please replace
{{Retracted}}with{{Retracted|intentional=yes}}.) - Hediger ML, England LJ, Molloy CA, Yu KF, Manning-Courtney P, Mills JL. Reduced bone cortical thickness in boys with autism or autism spectrum disorder. Journal of Autism and Developmental Disorders. 2008;38(5):848–56. doi:10.1007/s10803-007-0453-6. PMID 17879151.
- Doja A, Roberts W. Immunizations and autism: a review of the literature. Canadian Journal of Neurological Sciences. 2006;33(4):341–6. doi:10.1017/s031716710000528x. PMID 17168158.
- Thompson WW, Price C, Goodson B et al.. Early thimerosal exposure and neuropsychological outcomes at 7 to 10 years. New England Journal of Medicine. 2007;357(13):1281–92. doi:10.1056/NEJMoa071434. PMID 17898097.
- Weber W, Newmark S. Complementary and alternative medical therapies for attention-deficit/hyperactivity disorder and autism. Pediatric Clinics of North America. 2007;54(6):983–1006. doi:10.1016/j.pcl.2007.09.006. PMID 18061787.
- Chelation treatment for autism spectrum disorders: A systematic review. Research in Autism Spectrum Disorders. 2013;7(1):49–55. doi:10.1016/j.rasd.2012.06.005. "The research reviewed here does not support the use of chelation as a treatment for ASD"
- Lonsdale D, Shamberger RJ, Audhya T. Treatment of autism spectrum children with thiamine tetrahydrofurfuryl disulfide: a pilot study. Neuro Endocrinology Letters. 2002 [archived 2008-02-29; Retrieved 2008-02-04];23(4):303–8. PMID 12195231.
- Lonsdale D. A review of the biochemistry, metabolism and clinical benefits of thiamin(e) and its derivatives. Evidence-Based Complementary and Alternative Medicine. 2006 [archived 2007-10-25; Retrieved 2007-10-12];3(1):49–59. doi:10.1093/ecam/nek009. PMID 16550223. PMC 1375232.
- Campbell JB, Busse JW, Injeyan HS. Chiropractors and vaccination: a historical perspective. Pediatrics. 2000;105(4):e43. doi:10.1542/peds.105.4.e43. PMID 10742364.
- Busse JW, Morgan L, Campbell JB. Chiropractic antivaccination arguments. Journal of Manipulative and Physiological Therapeutics. 2005;28(5):367–73. doi:10.1016/j.jmpt.2005.04.011. PMID 15965414.
- Ferrance RJ. Autism—another topic often lacking facts when discussed within the chiropractic profession. 2003;47(1):4–7.
- Ernst E. Chiropractic: a critical evaluation. Journal of Pain and Symptom Management. 2008;35(5):544–62. doi:10.1016/j.jpainsymman.2007.07.004. PMID 18280103.
- Hawk C, Khorsan R, Lisi AJ, Ferrance RJ, Evans MW. Chiropractic care for nonmusculoskeletal conditions: a systematic review with implications for whole systems research. The Journal of Alternative and Complementary Medicine. 2007;13(5):491–512. doi:10.1089/acm.2007.7088. PMID 17604553.
- Green C, Martin CW, Bassett K, Kazanjian A. A systematic review of craniosacral therapy: biological plausibility, assessment reliability and clinical effectiveness. Complementary Therapies in Medicine. 1999;7(4):201–7. doi:10.1016/S0965-2299(99)80002-8. PMID 10709302. An earlier version of the paper is available without a subscription: A systematic review and critical appraisal of the scientific evidence on craniosacral therapy. 1999 [archived 2008-02-29; Retrieved 2007-10-08].
- Hartman SE, Norton JM. Interexaminer reliability and cranial osteopathy. 2002 [Retrieved 2007-10-08];6(1):23–34.
- Dhossche DM, Reti IM, Wachtel LE. Catatonia and autism: a historical review, with implications for electroconvulsive therapy. The Journal of ECT. 2009;25(1):19–22. doi:10.1097/YCT.0b013e3181957363. PMID 19190507.
- Rossignol DA, Rossignol LW, Smith S et al.. Hyperbaric treatment for children with autism: a multicenter, randomized, double-blind, controlled trial. BMC Pediatrics. 2009;9:21. doi:10.1186/1471-2431-9-21. PMID 19284641. PMC 2662857.
- Granpeesheh D., Tarbox J., Dixon D. R., Wilke A. E., Allen M. S., Bradstreet J.. Randomized trial of hyperbaric oxygen therapy for children with autism. Research in Autism Spectrum Disorders. 2010;4(2):268–275. doi:10.1016/j.rasd.2009.09.014.
- Jepson B., Granpeesheh D., Tarbox J., Olive M. L., Stott C., Braud S., Allen M. S.. Controlled evaluation of the effects of hyperbaric oxygen therapy on the behavior of 16 children with autism spectrum disorders. Journal of Autism and Developmental Disorders. 2011;41(5):575–588. doi:10.1007/s10803-010-1075-y.
- Rossignol Daniel A., Rossignol Lanier W., James S. Jill, Melnyk Stepan, Mumper Elizabeth. The Effects of Hyperbaric Oxygen Therapy on Oxidative Stress, Inflammation, and Symptoms in Children with Autism: An Open-label Pilot Study. 2007;7(36):1–13.
- Serruya MD, Kahana MJ. Techniques and devices to restore cognition. Behavioural Brain Research. 2008;192(2):149–65. doi:10.1016/j.bbr.2008.04.007. PMID 18539345.
- Bishop J. The Internet for educating individuals with social impairments. Journal of Computer Assisted Learning. 2003;19(4):546–56. doi:10.1046/j.0266-4909.2003.00057.x.
- el Kaliouby R, Picard R, Baron-Cohen S. Affective computing and autism. Annals of the New York Academy of Sciences. 2006;1093(1):228–48. doi:10.1196/annals.1382.016. PMID 17312261. Bibcode: 2006NYASA1093..228K.
- Novella, Steven (1 July 2013). "Transcranial Magnetic Stimulation for Autism". Neurologica Blog. Retrieved 15 December 2013.
- Use of Transcranial Magnetic Stimulation in Autism Spectrum Disorders. Journal of Autism and Developmental Disorders. October 2013;45(2):524–536. doi:10.1007/s10803-013-1960-2. PMID 24127165.
- Transcranial magnetic stimulation in autism spectrum disorder: Challenges, promise, and roadmap for future research.. Autism Research. February 2016;9(2):184–203. doi:10.1002/aur.1567. PMID 26536383.
- Ichim TE, Solano F, Glenn E et al.. Stem cell therapy for autism. Journal of Translational Medicine. 2007;5(30):30. doi:10.1186/1479-5876-5-30. PMID 17597540.
- Autism Spectrum Disorders: Is Mesenchymal Stem Cell Personalized Therapy the Future?. Journal of Biomedicine and Biotechnology. 2012;2012:1–5. doi:10.1155/2012/480289. PMID 22496609.
- Autism Spectrum Disorders: Is Mesenchymal Stem Cell Personalized Therapy the Future?. Journal of Biomedicine and Biotechnology. 1 January 2012;2012:1–6. doi:10.1155/2012/480289. PMID 22496609.
- Acupuncture for autism spectrum disorders (ASD). Cochrane Database of Systematic Reviews. Sep 7, 2011;9(9):CD007849. doi:10.1002/14651858.CD007849.pub2. PMID 21901712.
- Wing L. The history of ideas on autism: legends, myths and reality. 1997;1(1):13–23. doi:10.1177/1362361397011004.
- Miles M. Independent Living Institute. Martin Luther and childhood disability in 16th century Germany: what did he write? what did he say?; 2005 [Retrieved 2008-12-23].
- Collins D. Autistic boy dies during exorcism. CBS News. 2003-08-25.
- Shaked M, Bilu Y. Grappling with affliction: autism in the Jewish ultraorthodox community in Israel. Culture, Medicine and Psychiatry. 2006;30(1):1–27. doi:10.1007/s11013-006-9006-2. PMID 16783528.
- Ekas NV, Whitman TL, Shivers C. Religiosity, spirituality, and socioemotional functioning in mothers of children with autism spectrum disorder. Journal of Autism and Developmental Disorders. 2009;39(5):706–19. doi:10.1007/s10803-008-0673-4. PMID 19082877.
- Harmon, Amy (2004-12-20). "How About Not 'Curing' Us, Some Autistics Are Pleading". The New York Times. Archived from the original on December 2, 2011. Retrieved 2007-11-07.
- Saner E (2007-08-07). "It is not a disease, it is a way of life". The Guardian. Archived from the original on 20 August 2007. Retrieved 2007-08-07.
- Autism's early child, Guardian, retrieved 13/11/2011
- Environmental enrichment and brain repair: harnessing the therapeutic effects of cognitive stimulation and physical activity to enhance experience-dependent plasticity.. Neuropathology and Applied Neurobiology. February 2014;40(1):13–25. doi:10.1111/nan.12102. PMID 24354721.
- Environmental enrichment as a therapy for autism: A clinical trial replication and extension.. Behavioral Neuroscience. August 2015;129(4):412–22. doi:10.1037/bne0000068. PMID 26052790.
- Environmental enrichment as an effective treatment for autism: a randomized controlled trial.. Behavioral Neuroscience. August 2013;127(4):487–97. doi:10.1037/a0033010. PMID 23688137.
- Flashback to the 1960s: LSD in the treatment of autism.. Developmental Neurorehabilitation. 2006;10(1):75–81. doi:10.1080/13638490601106277. PMID 17608329.
Further reading
- William Shaw, Bernard Rimland, Biological treatments for autism and PDD, 3rd ed., W. Shaw, 2008 ISBN 0-9661238-1-6
- Ministries of Health and Education. New Zealand Autism Spectrum Disorder Guideline [PDF]. Wellington: Ministry of Health; 2008 [Retrieved 2009-01-23]. ISBN 978-0-478-31257-7.
- Fitzpatrick M. Defeating Autism: A Damaging Delusion. London: Routledge; 2008. ISBN 0-415-44981-2. Reviewed in: Guldberg H. spiked. 'Autistic children are now seen as a burden'; 2008-12-19.
- Posey DJ, McDougle CJ. Preface. Child and Adolescent Psychiatric Clinics of North America. 2008;17(4):xv–xviii. doi:10.1016/j.chc.2008.07.001. PMID 18775365. This describes a special issue of the journal Child and Adolescent Psychiatric Clinics of North America, titled "Treating Autism Spectrum Disorders" (volume 17, issue 4, pages 713–932) and dated October 2008.
- Bryson SE, Rogers SJ, Fombonne E. Autism spectrum disorders: early detection, intervention, education, and psychopharmacological management. Canadian Journal of Psychiatry. 2003 [archived 2007-09-29];48(8):506–16. doi:10.1177/070674370304800802. PMID 14574826.
- Erickson CA, Posey DJ, Stigler KA, McDougle CJ. Pharmacologic treatment of autism and related disorders. Pediatric Annals. 2007;36(9):575–85. doi:10.3928/0090-4481-20070901-09. PMID 17910205.