We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
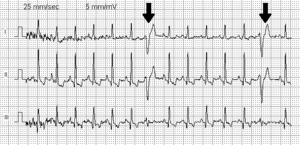
Premature ventricular contraction
From WikEM
Contents
Background
- Abbreviation: PVC
Causes

Clinical Features
- May be asymptomatic, or may have Palpitations
Differential Diagnosis
Palpitations
- Arrhythmias:
- Atrial fibrillation
- Grouped beats on ECG (commonly misdx as A-fib)
- Atrial bigeminy and trigeminy
- Mobitz I or Mobitz II
- Atrial flutter
- SVT
- Ventricular Tachycardia
- Sick sinus syndrome
- Multifocal atrial tachycardia
- PVCs
- Wolff–Parkinson–White syndrome (WPW)
- Sinus node dysfunction
- AV Block
- Lown-Ganong-Levine Syndrome
- Accelerated idioventricular rhythm
- Non-arrhythmic cardiac causes:
- Cardiomyopathy
- CHF
- Mitral valve prolapse
- Congenital heart disease
- Pericarditis
- Valvular disease
- Pacemaker malfunction
- Acute MI
- Psychiatric causes:
- Drugs and Medications:
- Alcohol
- Caffeine
- Meds (i.e. digitalis, theophylline)
- Street drugs (i.e. cocaine)
- Tobacco
- Misc
Evaluation
Workup
- ECG
- If PVC burden is large, consider:
- TSH
- BMP
- Magnesium level
- Ionized calcium
Management[1]
- Benign; generally does not require any treatment or additional workup
- Treat hypoxia/drug toxicity if existing
- Correct electrolyte imbalances, particularly magnesium, calcium, potassium
- Acute ischemia/infarction:
- Complex ectopy frequently seen after patient receives thrombolytics
- 1st line are beta blockers, options below[2]:
- Acute MI: Metoprolol 5mg IV q2 min for x3 doses, then PO metoprolol 50mg q6hrs for 2 days, followed by maintenance of 100mg bid
- Post-MI: Atenolol 5mg IV over 5 min, then repeat in 10 min, then PO atenolol 50mg q12hrs for 7 days post-MI
Disposition
- Generally may be discharged (unless other indications for admission exist)
See Also
External Links
References
- ↑ Keany et al. Premature Ventricular Contraction Treatment & Management. Updated Jan 7, 2014. http://emedicine.medscape.com/article/761148-treatment#d10
- ↑ McAuley DF. Beta Blockers. GlobalRPH. http://www.globalrph.com/beta.htm
Authors
Kevin Lu, Ross Donaldson, Michael Holtz, Neil Young, Daniel Ostermayer