EBQ:ED Airway Assessment Score Predicting Difficult Intubation
PubMed Full text PDF
Contents
Clinical Question
Can an airway assessment scale based on LEMON methodology predict difficulty of intubation in the ED?
Conclusion
The LEMON airway assessment score based successfully predicts difficult poor laryngoscopic views although not necessarily predict airway intubation failure.
Major Points
Assessment of the airway difficulty prior to intubation allows the emergency physician to stratify the risk of intubation difficulty.[1] Since most emergency department intubations are not elective, it is important to prepare with all airway adjuncts (Bougie, Supraglottic device, and video laryngoscopy) prior to attempt. This study demonstrates that the LEMON mneumonic can successfully stratify risk but not necessarily predict intubation failure. There were no failures in this study and preparation should always anticipate the need for surgical airway management as the end point for patients with respiratory failure and failed intubation.
| Difficult Airway Predictor | Point |
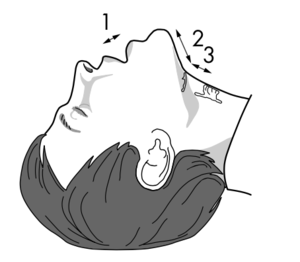
Any of 4 important LOOK criteria:
|
1 point each |
| Mouth opening less than three finger breadths | 1 |
| Hyo-mental distance less than three finger breadths | 1 |
| Thyro-hyoid distance less than two finger breadths | 1 |
| Presence of an obstructed airway | 1 |
| Presence of poor neck mobility | 1 |
Increasing score equates to increasing difficulty for chord visualization but not necessarily intubation failure rates.
Design
- Prospective observational study conducted in the ED of a UK teaching hospital between June 2002 and September 2003
- Intubation was recorded according to Cormack and Lehane scores if the patient required intubation[2]
Population Studied
Inclusion Criteria
- All patients who entered one of the department’s resuscitation rooms
Exclusion Criteria
- Only patients requiring intubation underwent the procedure
Baseline Characteristics
- N= 156
- Median Age= 55yo
- Male= 71%
Interventions
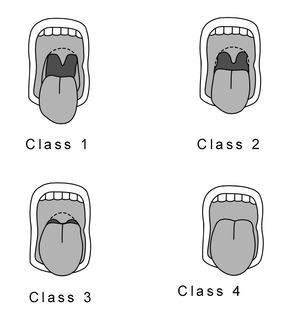
- All patients underwent an airway assessment according to the LEMON method and many underwent the Mallampati score. Only patients requiring intubation had a Cormack and Lehane score recorded and had intubation attempted.
Outcomes
Primary Outcomes
Patients with large incisors, reduced inter-incisor distance and a reduced thyroid to floor of mouth distance were more likely to have worse laryngoscopic view on intubation.
- All patients were successfully intubated
Subgroup Analysis
- There was no statistical difference in intubation grade in patients with:
- Facial trauma (p = 1.0)
- Beard or moustache (p = 0.49)
- Large tongue (p = 0.49)
- Reduced hyoid to chin distance (p = 0.34)
- There was a statistical association in intubation grade in patients with:
- Reduced inter-incisor distance (p=0.05)
- Reduced thyroid to floor of mouth distance (p=0.05)
Discussion
- The airway manager performing the LEMON assessment also performed the intubation introducing the risk for bias.
- Difficulty of intubation was defined by vocal cord views however this did not prevent any failed intubations
- No airway adjuncts were used for intubation however preparation should include appropriate preoxygenation and preparation for cricothyrotomy if all methods of intubation are unsuccessful
Funding
- No industry funding
See Also
- Intubation
- LMA
- ED Preoxygenation
- Cricothyrotomy
- Difficult airway algorithm
- Bag valve mask ventilation
Review Questions
References
- ↑ Murphy MF, Walls RM. The difficult and failed airway. In: Manual of emergency airway management. Chicago: Lippincott Williams and Wilkins, 2000:31–9
- ↑ Cormack RS, Lehane J. Difficult intubation in obstetrics. Anaesthesia 1984;39:1105–11.
- ↑ J Emerg Med 2010; 5:622-631.