Transverse ligament of atlas
The transverse ligament of the atlas is a thick, strong band, which arches across the ring of the atlas, and retains the odontoid process in contact with the atlas.
| Transverse ligament of the atlas | |
|---|---|
 | |
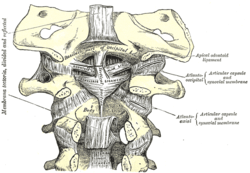 Membrana tectoria, transverse, and alar ligaments. (Transverse ligament visible at center.) | |
| Details | |
| Identifiers | |
| Latin | ligamentum transversum atlantis |
| TA | A03.2.04.006 |
| FMA | 24961 |
| Anatomical terminology | |
Anatomy
It is concave in front, convex behind, broader and thicker in the middle than at the ends, and firmly attached on either side to a small tubercle on the medial surface of the lateral mass of the atlas.[1]
As it crosses the odontoid process, a small fasciculus (crus superius) is prolonged upward, and another (crus inferius) downward, from the superficial or posterior fibers of the ligament.[1]
The former is attached to the basilar part of the occipital bone, in close relation with the membrana tectoria; the latter is fixed to the posterior surface of the body of the axis; hence, the whole ligament is named the cruciate ligament of the atlas.[1]
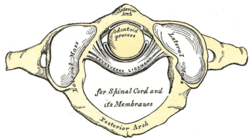
The transverse ligament divides the ring of the atlas into two unequal parts: of these, the posterior and larger serves for the transmission of the medulla spinalis and its membranes and the accessory nerves; the anterior and smaller contains the odontoid process.[1]
The neck of the odontoid process is constricted where it is embraced posteriorly by the transverse ligament, so that this ligament suffices to retain the odontoid process in position after all the other ligaments have been divided.[1]
Role in disease
Excessive laxity of the posterior transverse ligament can lead to atlantoaxial instability, a common complication in patients with Down's Syndrome. Laxity has also been hypothesized as the cause of degenerative hypertrophy and mechanical atlantoaxial stress.[2] Degenerative processes can give rise to transverse ligament cysts, resulting in progressive cervical myelopathy. The treatment of choice for transverse ligament cysts with progressive neurological decline is surgical resection and cervical fusion.[3] Conservative treatment with external neck immobilization is less commonly reported , but may be very useful in select cases where immediate surgical intervention is not indicated.[4][5]
References
- Gray's anatomy, 1918
- Takeuchi, Mikinobu; Yasuda, Muneyoshi; Takahashi, Emiko; Funai, Mikiko; Joko, Masahiro; Takayasu, Msakazu (December 2011). "A large retro-odontoid cystic mass caused by transverse ligament degeneration with atlantoaxial subluxation leading to granuloma formation and chronic recurrent microbleeding case report". The Spine Journal. 11 (12): 1152–1156. doi:10.1016/j.spinee.2011.11.007. ISSN 1878-1632. PMID 22177924.
- Van Gompel, Jamie J.; Morris, Jonathan M.; Kasperbauer, Jan L.; Graner, Darlene E.; Krauss, William E. (April 2011). "Cystic deterioration of the C1-2 articulation: clinical implications and treatment outcomes". Journal of Neurosurgery. Spine. 14 (4): 437–443. doi:10.3171/2010.12.SPINE10302. ISSN 1547-5646. PMID 21314283.
- Sagiuchi, Takao; Shimizu, Satoru; Tanaka, Ryusui; Tachibana, Shigekuni; Fujii, Kiyotaka (August 2006). "Regression of an atlantoaxial degenerative articular cyst associated with subluxation during conservative treatment. Case report and review of the literature". Journal of Neurosurgery. Spine. 5 (2): 161–164. doi:10.3171/spi.2006.5.2.161. ISSN 1547-5654. PMID 16925084.
- Oushy, Soliman; Carlstrom, Lucas P.; Krauss, William E. (2018-03-05). "Spontaneous Regression of a Retroodontoid Transverse Ligament Cyst: A Case Report". Neurosurgery. doi:10.1093/neuros/nyy036. ISSN 1524-4040. PMID 29518219.
| Authority control |
|---|