We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Sulfonylurea toxicity
From WikEM
Contents
Background
- sulfonylureas are a commonly prescribed oral diabetes medication, and include glyburide, glimepiride, glipizide chlorpropamide, tolazamide
- inhibit potassium efflux from pancreatic beta cells→ increased insulin release
Clinical Features
- Hypoglycemia
- can occur at therapeutic doses in renally impaired patients
- hypoglycemia often prolonged and severe
- onset within 8 hours of ingestion
- Pediatrics: one pill can kill!!
Differential Diagnosis
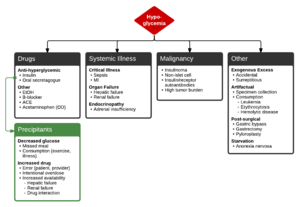
Hypoglycemia
Drugs
- Anti-hyperglycemic
- Insulin
- Oral secretagogue
- Sulfonylurea toxicity
- Other
Systemic Illness
- Critical Illness
- Organ Failure
- Hepatic failure
- Renal failure
- Endocrinopathy
- Seizure
Malignancy
- Insulinoma
- Non-islet cell
- Insulin/receptor autoantibodies
- High tumor burden
Other
- Artifactual
- Specimen collection
- Consumption
- Leukemia
- Erythrocytosis
- Hemolytic disease
- Post-surgical
- Gastric bypass
- Gastrectomy
- Pyloroplasty
- Starvation
Precipitants of anti-hyperglycemic induced hypoglycemia
- Decreased glucose
- Missed meal
- Consumption (exercise, illness)
- Increased drug
- Error (patient, provider)
- Intentional overdose
- Increased availability
- Hepatic failure
- Renal failure
- Drug interaction
Evaluation
- Hypoglycemia + known or suspected ingestion
- BMP, creatinine, decrease in renal clearance may have led to toxicity
- Serial POC glucose measurements
- Routine ingestion labs if suspect intentional OD
- Acetaminophen and salicylate levels
- ECG, look for QRS widening and QTc prolongation
Management
Hypoglycemia from Sulfonylureas[1][2]
Activated charcoal[3]
- Administer activated charcoal, preferably within 1 hr of ingestion
- Multiple doses may be beneficial, especially for glipizide
Glucose Treatment
- Initial Therapy regardless of known cause
- Adults
- 50mL D50W bolus
- Start a D10 1/2NS drip (100mL/hr)
- Children
- 1mL/kg of D50W OR
- 2mL/kg D25W OR 5-10mL/kg D10W
- Neonate: 5-10 mL/kg D10W
Octreotide[4]
- Theoretical benefit to reduce risk of recurrent hypoglycemia
- Hyperpolarization of the beta cell results in inhibition of Ca influx and prevents insulin release
- 50-100 mcg subcutaneous in adults with repeat dosing Q6hrs
- 2 mcg/kg (max 150mcg) subcutaneously Q6hrs should be used in children
- Continuous infusion of 50-125 mcg/hr is an alternative in adults
- Administer octreotide for 24 hours, then after discontinuing, monitor for hypoglycemia for another 24 hours
Special Considerations
- Glucagon 5mg IM may be used as temporizing measure, e.g. while obtaining IV access
Disposition
- Admit
See Also
External Links
References
- ↑ Rowden AK, Fasano CJ. Emergency management of oral hypoglycemic drug toxicity. Emerg Med Clin N Am 2007; 25:347-356
- ↑ Howland MA. Antidotes in Depth: Octreotide. In: Flomenbaum NE, Goldfrank LR, Hoffman RS et al, eds: Goldfrank’s Toxicologic Emergencies. New York NY, 2006;770-773
- ↑ Tran D et al. Oral Hypoglycemic Agent Toxicity Treatment & Management. Jul 14, 2015. http://emedicine.medscape.com/article/1010629-treatment#showall.
- ↑ Fasano CJ et al. Comparison of Octreotide and standard therapy versus standard therapy alone for the treatment of sulfonylurea-induced hypoglycemia. Ann Emerg Med 2008; 51:400-406