We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
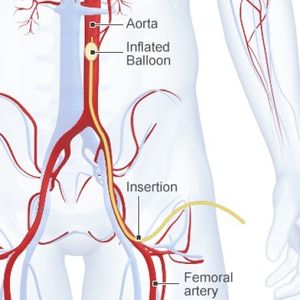
Resuscitative endovascular balloon occlusion of the aorta
From WikEM
Contents
Overview
- Abbreviation: REBOA
- Hemorrhage is a leading cause of trauma-related mortality[1]
- REBOA has been proposed as a less invasive alternative to resuscitative thoracotomy
- Research is ongoing, but has yet to demonstrate a mortality benefit[2]
REBOA Zones
- Zone 1: From left subclavian artery to the celiac trunk
- Zone 2: From the celiac trunk to the lowest renal artery
- Zone 2 is an unused zone because if of difficulty in occluding the bleeding vessel at this aortic location
- Zone 3: From lowest renal artery to the aortic bifurcation
Indications
- Non-compressible hemorrhage below the diaphragm in the abdomen, pelvis or retroperitoneum [3]
- Postive FAST
- Pelvic frature with negative FAST
- Traumatic cardiac arrest without aortic dissection or pericardial tamponade
- Suspected traumatic abdominal hemorrhage (Zone I REBOA)
- Blunt pelvic injury or groin junctional hemorrhage (Zone III REBOA)
Contraindications
- Age ≤18 or ≥70y
- Non traumatic arrest
- Proximal traumatic aortic dissection
- Proximal aortic dissection
- Cardiac tamponade
Equipment Needed
- Ultrasound
- REBOA Kit
Procedure
- Immediately perform a FAST exam to assess for pericardial tamponade (contraindication)
- Access the common femoral artery under ultarsound guid and place a standard 18G arterial line
- Pass a 260cm guidewire through that arterial line up to the level of the left subclavian
- Obtain a chest Xray if feasible to confirm the position of the guidewire
- Estimate length of catheter insertion based on desired location and external landmarks
- Zone 1: Xiphoid process for Zone 1 (aprox 50cm)
- Zone 3: umbilicus for Zone 3 (approx 40cm)
- Place the REBOA 12 French arterial line introducer sheath
- Advance the catheter over the wire through the sheath, then inflate the balloon with saline in the desired zone
- Resistance will be felt as the balloon inflates against the wall of the aorta and blood pressure will increase substantially if successful
Complications
- Not accessing the common femoral artery or accessing it blindly
See Also
External Links
References
- ↑ Tieu BH et al. Coagulopathy: Its pathophysiology and treatment in the injured patient. World J Surg. 2007;31:1055–64
- ↑ Morrison JJ, Galgon RE, Jansen JO, et al. A systematic review of the use of resuscitative endovascular balloon occlusion of the aorta in the management of hemorrhagic shock. J Trauma Acute Care Surg. 2016 Feb;80(2):324-34.
- ↑ Qasim, Zaffer, et al. “Resuscitative endovascular balloon occlusion of the aorta.” Resuscitation 96 (2015): 275-279.
Authors
Daniel Ostermayer, Michael Holtz, Daniel Eggeman, Claire, Ross Donaldson