We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Multiple sclerosis
From WikEM
Contents
Background
- CNS myelin destruction causes variable motor, sensory, visual and cerebellar dysfunction
Types
- Relapsing/remitting (most common)
- Relapse (days-months) followed by remission
- Secondary progressive
- Relapses and partial recoveries occur, but disability does not fade away between cycles
- Primary progressive
- Symptoms progress slowly and steadily without remission
- Progressive relapsing
- Similar to primary progressive but with superimposed flares
Clinical Features
- Classic patient has multiple presentations for neuro symptoms of different areas of pathology
- Patient often has resolution of the earlier symptoms
- Symptoms worsen with increases in body temperature (Uhthoff's phenomenon[1])
- Muscle/sensory signs:
- Lower extremity weakness usually worse than upper extremity
- Upper motor neuron signs:
- Hyperreflexia
- Positive Babinski
- Decrease in proprioception / pain/temperature sensation
- Lhermitte sign
- Electric shock sensation radiating down back into arms/egs from neck flexion
- Optic neuritis
- Initial sign in 30% of patients
- Vision loss (usually unilateral) often preceded by retrobulbar pain
- Blurred vision
- Afferent pupillary defect is pathognomonic for optic neuritis
- Nystagus
- Diplopia
- Internuclear ophthalmoplegia
- Abnormal eye adduction bilaterally and horizontal nystagmus
- Convergence (both eyes center medially) is preserved
- Dysautonomia
- Urinary retention (increased risk of UTI/pyelo)
- Constipation or incontinence
- Sexual dysfunction (males)
Differential Diagnosis
Weakness
- Neuromuscular weakness
- UMN:
- CVA
- Hemorrhagic stroke
- Multiple sclerosis
- Amyotrophic Lateral Sclerosis (ALS) (UMN & LMN)
- Spinal cord disease:
- Infection (Epidural abscess)
- Infarction/ischemia
- Trauma (Spinal Cord Syndromes)
- Inflammation (Transverse Myelitis)
- Degenerative (Spinal muscular atrophy)
- Tumor
- Peripheral nerve disease:
- Guillain-Barre syndrome
- Toxins (Ciguatera)
- Tick paralysis
- DM neuropathy (non-emergent)
- NMJ disease:
- Muscle disease:
- Rhabdomyolysis
- Dermatomyositis
- Polymyositis
- Alcoholic myopathy
- UMN:
- Non-neuromuscular weakness
- Can't miss diagnoses:
- ACS
- Arrhythmia/Syncope
- severe infection/Sepsis
- Hypoglycemia
- Periodic paralysis (electrolyte disturbance, K, Mg, Ca)
- Respiratory failure
- Emergent Diagnoses:
- Symptomatic Anemia
- Severe dehydration
- Hypothyroidism
- Polypharmacy
- Malignancy
- Other causes of weakness and paralysis
- Acute intermittent porphyria (ascending weakness)
- Can't miss diagnoses:
Evaluation
Work-Up
- LP
- IgG
- Albumin
- Oligoclonal bands
- myelin basic protein
- Cell count
- Glucose
- Protein
- Gm stain
- CBC, Chemistry
- Urinalysis
- MRI with GAD of brain (+/- spine)
Evaluation
- CSF
- Elevated protein and gamma-globulin (increased oligoclonal bands)
- MRI
- Multiple lesions in supratentorial white matter, paraventricular area, spinal cord
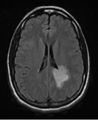
MRI brain with contrast of a patient in her mid-20s with new onset MS. Large lesion in left parietal area.

MRI brain with contrast of same patient with new onset MS with another lesion in the left cerebellum.
Management
- Fever must be reduced to minimize weakness associated with elevated temperature
- Antibiotics for UTI/pyelo
- High-dose steroid therapy for relapses
- Suppression therapies
- IFN B, Glatiramer, Estriol (usually not in ED)
Disposition
- Hospitalization indicated for:
- Any disease exacerbation associated with significant morbidity
- IV antibiotics or steroid therapy required
- Depression and significant risk of suicide
See Also
References
- ↑ Flensner G, et al. "Sensitivity to heat in MS patients: a factor strongly influencing symptomology-an explorative survey". BMC Neurol. 2011. 11:27.