We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Lower back pain
From WikEM
Contents
Background
- Pain lasting >6wks is risk factor for more serious disease
- Night pain and unrelenting pain are worrisome symptoms
- Back pain in IV drug user is spinal infection until proven otherwise
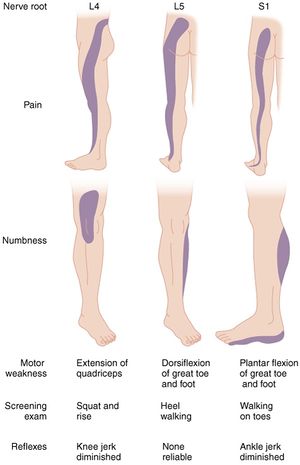
- 95% of herniated discs occur at L4-L5 or L5-S1 (for both pain extends below the knee)
- Lumbago: acute, nonspecific back pain
Clinical Features
- Musculoskeletal pain
- Located primarily in the back with possible radiation into the buttock/thighs
- Pain worse with movement but improves with rest
- Spinal stenosis
- Bilateral sciatic pain worsened by walking (pseudo-claudication), prolonged standing
- Pain relieved by forward flexion, especially sitting
- Sciatica
- Radicular back pain in the distribution of a lumbar or sacral nerve root
- Anything that compresses the nerve roots, cauda equina, or cord can cause sciatica
- Pain worsened by coughing, Valsalva, sitting; relieved by lying in supine position
- Occurs in only 1% of patients with back pain
- Present in 95% of patients who have a symptomatic herniated disk
- Radicular back pain in the distribution of a lumbar or sacral nerve root
- Urinary/bowel disturbances, perineal anaesthesia
- Cauda equina syndrome, due to compression of spinal nerve roots
- Ortho emergency!
- Inflammatory back pain
- Morning stiffness >30minutes
- Consider seronegative spondyloarthropathies, especially if in young adults (eg ankylosing spondylitis, psoriatic arthropathy, IBD arthropathy, Reiter's disease)
| Factor | Post Test Probability |
| Older Age (>65yo) | 9%
(95% CI 3% to 25%) |
| Prolonged corticosteroid | 33%
(95% CI 10% to 67%) |
| Severe trauma | 11%
(95% CI 8% to 16%) |
| Presence of contusion or abrasion | 62%
(95% CI 49% to 74%) |
| Multiple red flags | 90%
(95% CI 34% to 99%) |
| Hx of malignancy | 33%
(95% CI 22% to 46%) |
Waddell's Signs of Non-Organic Back Pain
- Assess for the following[2]:
- Over-reaction to the examination
- Widespread superficial tenderness not corresponding to any anatomical distribution
- Pain on axial loading of the skull or pain on rotation of the shoulders and pelvis together
- Severely limited straight leg raising on formal testing in a patient who can sit forwards with the legs extended
- Lower limb weakness or sensory loss not corresponding to a nerve root distribution
- 3 or more positives suggest non-organic or alternative organic source
Differential Diagnosis

Lower Back Pain
- Spine related
- Acute ligamentous injury
- Acute muscle strain
- Disk herniation (Sciatica)
- Degenerative joint disease
- Spondylolithesis
- Epidural compression syndromes
- Spinal fracture
- Cancer metastasis
- Spinal stenosis
- Transverse myelitis
- Vertebral osteomyelitis
- Ankylosing spondylitis
- Spondylolithesis
- Discitis
- Renal disease
- Intra-abdominal
- Abdominal aortic aneurysm
- Ulcer perforation
- Retrocecal appendicitis
- Large bowel obstruction
- Pancreatitis
- Pelvic disease
- Other
- Retroperitoneal hemorrhage/mass
- Meningitis
Evaluation
Exam
- Straight leg raise testing
- Screening exam for a herniated disk (Sn 68-80%)
- Lifting leg causes radicular pain of affected leg radiating to BELOW the knee
- Pain is worsened by ankle dorsiflexion
- Pain may be relieved by pressing across biceps femoris and pes anserinus tendons behind knee ('bowstringing')
- Crossed Straight leg raise testing (high Sp, low Sn)
- Lifting the asymptomatic leg causes radicular pain down the affected leg
- Nerve root compromise
- Rectal exam, perineal sensation, palpable bladder?
- To rule out cauda equina syndrome
Labs
- Pregnancy test
- Only necessary if concerned for infection, tumor, or rheumatologic cause
- CBC, UA, ESR (90-98% Sn for infectious etiology)
- Consider post void residual
- Can be done with non invasively with Ultrasound
Imaging
- Plain films
- Only necessary if suspect fracture, tumor, or infection
- Part of ACEP Choosing wisely
- MRI
- Only necessary if suspect infection, neoplasm, epidural compression syndromes
- Consider for back pain >6-8wks
- Ultrasound
- Rule-out AAA
Management
Nonspecific Back Pain (musculoskeletal)
- Instruct to continue daily activities using pain as limiting factor
- Medications
- Acetaminophen
- NSAIDs
- 1st line therapy
- Consider gel/patch like diclofenac or ketoprofen (shown to be more effective than PO form and placebo in one study[3])
- Lidocaine Patches
- Capsaicin or Cayenne
- Skin desensitization upon repeated exposure
- Opioids
- Appropriate for moderate-severe pain but only for limited duration (1-2wks)
- Muscle relaxants
- Efficacy appears equal to NSAIDs
- Diazepam 5-10mg PO q6-8hr OR methocarbamol 1000-1500mg PO QID
- Steroids (of questionable effectiveness[4][5])
- Prednisone 40-60mg PO qd x 5-10 days
Sciatica
- Treatment is the same as for musculoskeletal back pain
- 80% of patients will ultimately improve without surgery
- Primary care provider should consider AEDs (gapapentin, titrate slowly) or TCAs (nortriptyline, amytriptyline)
- Gabapentin Oral: Immediate release: 400mg-1,200mg PO TID
Spinal stenosis
- Treatment is the same as for musculoskeletal back pain
Cauda equina syndrome
- Immediate Ortho referral for spinal decompression to avoid permanent bowel/bladder injury
Disposition
- Normally outpatient, as long as no signs of emergent pathology and able to ambulate
See Also
External Links
References
- ↑ Downie A, et al. Red flags to screen for malignancy and fracture in patients with low back pain: systematic review. BMJ. 2013; 347:f7095. [1]
- ↑ Waddell G, et al. Non-organic physical signs in low-back pain. Spine. 1980; 5:117-125.
- ↑ Mazières B, Rouanet S, Velicy J, et al. Topical ketoprofen patch (100 mg) for the treatment of ankle sprain: a randomized, double-blind, placebo-controlled study. Am J Sports Med. 2005;33:515-523
- ↑ Holve, RL, et al. Oral steroids in initial treatment of acute sciatica. J Am Board Fam Med. 2008; 21(5):469-474.
- ↑ Goldberg H, et al. Oral steroids for acute radiculopathy due to a herniated lumbar disk: a randomized clinical trial. JAMA. 2015 May 19;313(19):1915-23. PMID 25988461.