

US Selected Practice Recommendations for Contraceptive Use, 2016
 ShareCompartir
ShareCompartir
Combined Hormonal Contraceptives
On This Page
- Initiation of Combined Hormonal Contraceptives
- Examinations and Tests Needed Before Initiation of Combined Hormonal Contraceptives
- Number of Pill Packs that Should Be Provided at Initial and Return Visits
- Routine Follow-Up After Combined Hormonal Contraceptive Initiation
- Late or Missed Doses and Side Effects from Combined Hormonal Contraceptive Use
- Vomiting or Severe Diarrhea While Using COCs
- Unscheduled Bleeding with Extended or Continuous Use of Combined
- FIGURE 2. Recommended actions after late or missed combined oral contraceptives
- FIGURE 3. Recommended actions after delayed application or detachment* with combined hormonal patch
- FIGURE 4. Recommended actions after delayed insertion or reinsertion* with combined vaginal ring
- TABLE 4. Classification of examinations and tests needed before combined hormonal contraceptive initiation
- FIGURE 5. Recommended steps after vomiting or diarrhea while using combined oral contraceptives
Combined hormonal contraceptives contain both estrogen and a progestin and include 1) COCs (various formulations), 2) a transdermal contraceptive patch (which releases 150 µg of norelgestromin and 20 µg ethinyl estradiol daily), and 3) a vaginal contraceptive ring (which releases 120 µg etonogestrel and 15 µg ethinyl estradiol daily). Approximately 9 out of 100 women become pregnant in the first year of use with combined hormonal contraceptives with typical use (14). These methods are reversible and can be used by women of all ages. Combined hormonal contraceptives are generally used for 21–24 consecutive days, followed by 4–7 hormone-free days (either no use or placebo pills). These methods are sometimes used for an extended period with infrequent or no hormone-free days. Combined hormonal contraceptives do not protect against STDs; consistent and correct use of male latex condoms reduces the risk for STDs, including HIV.
Initiation of Combined Hormonal Contraceptives
Timing
- Combined hormonal contraceptives can be initiated at any time if it is reasonably certain that the woman is not pregnant (Box 2).
Need for Back-Up Contraception
- If combined hormonal contraceptives are started within the first 5 days since menstrual bleeding started, no additional contraceptive protection is needed.
- If combined hormonal contraceptives are started >5 days since menstrual bleeding started, the woman needs to abstain from sexual intercourse or use additional contraceptive protection for the next 7 days.
Special Considerations
Amenorrhea (Not Postpartum)
- Timing: Combined hormonal contraceptives can be started at any time if it is reasonably certain that the woman is not pregnant (Box 2).
- Need for back-up contraception: The woman needs to abstain from sexual intercourse or use additional contraceptive protection for the next 7 days.
Postpartum (Breastfeeding)
- Timing: Combined hormonal contraceptives can be started when the woman is medically eligible to use the method (5) and if it is reasonably certain that she is not pregnant. (Box 2).
- Postpartum women who are breastfeeding should not use combined hormonal contraceptives during the first 3 weeks after delivery (U.S. MEC 4) because of concerns about increased risk for venous thromboembolism and generally should not use combined hormonal contraceptives during the fourth week postpartum (U.S. MEC 3) because of concerns about potential effects on breastfeeding performance. Postpartum breastfeeding women with other risk factors for venous thromboembolism generally should not use combined hormonal contraceptives 4–6 weeks after delivery (U.S. MEC 3).
- Need for back-up contraception: If the woman is <6 months postpartum, amenorrheic, and fully or nearly fully breastfeeding (exclusively breastfeeding or the vast majority [≥85%] of feeds are breastfeeds) (27), no additional contraceptive protection is needed. Otherwise, a woman who is ≥21 days postpartum and has not experienced return of her menstrual cycle needs to abstain from sexual intercourse or use additional contraceptive protection for the next 7 days. If her menstrual cycles have returned and it has been >5 days since menstrual bleeding started, she needs to abstain from sexual intercourse or use additional contraceptive protection for the next 7 days.
Postpartum (Not Breastfeeding)
- Timing: Combined hormonal contraceptives can be started when the woman is medically eligible to use the method (5) and if it is reasonably certain that she is not pregnant (Box 2).
- Postpartum women should not use combined hormonal contraceptives during the first 3 weeks after delivery (U.S. MEC 4) because of concerns about increased risk for venous thromboembolism. Postpartum women with other risk factors for venous thromboembolism generally should not use combined hormonal contraceptives 3–6 weeks after delivery (U.S. MEC 3).
- Need for back-up contraception: If a woman is <21 days postpartum, no additional contraceptive protection is needed. A woman who is ≥21 days postpartum and whose menstrual cycles have not returned needs to abstain from sexual intercourse or use additional contraceptive protection for the next 7 days. If her menstrual cycles have returned and it has been >5 days since menstrual bleeding started, she needs to abstain from sexual intercourse or use additional contraceptive protection for the next 7 days.
Postabortion (Spontaneous or Induced)
- Timing: Combined hormonal contraceptives can be started within the first 7 days after first or second trimester abortion, including immediately postabortion (U.S. MEC 1).
- Need for back-up contraception: She needs to abstain from sexual intercourse or use additional contraceptive protection for the next 7 days unless combined hormonal contraceptives are started at the time of a surgical abortion.
Switching from Another Contraceptive Method
- Timing: Combined hormonal contraceptives can be started immediately if it is reasonably certain that the woman is not pregnant (Box 2). Waiting for her next menstrual period is unnecessary.
- Need for back-up contraception: If it has been >5 days since menstrual bleeding started, she needs to abstain from sexual intercourse or use additional contraceptive protection for the next 7 days.
- Switching from an IUD: If the woman has had sexual intercourse since the start of her current menstrual cycle and it has been >5 days since menstrual bleeding started, theoretically, residual sperm might be in the genital tract, which could lead to fertilization if ovulation occurs. A health-care provider may consider any of the following options:
- Advise the women to retain the IUD for at least 7 days after combined hormonal contraceptives are initiated and return for IUD removal.
- Advise the woman to abstain from sexual intercourse or use barrier contraception for 7 days before removing the IUD and switching to the new method.
- If the woman cannot return for IUD removal and has not abstained from sexual intercourse or used barrier contraception for 7 days, advise the woman to use ECPs at the time of IUD removal. Combined hormonal contraceptives can be started immediately after use of ECPs (with the exception of UPA). Combined hormonal contraceptives can be started no sooner than 5 days after use of UPA.
Comments and Evidence Summary. In situations in which the health-care provider is uncertain whether the woman might be pregnant, the benefits of starting combined hormonal contraceptives likely exceed any risk; therefore, starting combined hormonal contraceptives should be considered at any time, with a follow-up pregnancy test in 2–4 weeks. If a woman needs to use additional contraceptive protection when switching to combined hormonal contraceptives from another contraceptive method, consider continuing her previous method for 7 days after starting combined hormonal contraceptives.
A systematic review of 18 studies examined the effects of starting combined hormonal contraceptives on different days of the menstrual cycle (202). Overall, the evidence suggested that pregnancy rates did not differ by the timing of combined hormonal contraceptive initiation (169,203–205) (Level of evidence: I to II-3, fair, indirect). The more follicular activity that occurred before starting COCs, the more likely ovulation was to occur; however, no ovulations occurred when COCs were started at a follicle diameter of 10 mm (mean cycle day 7.6) or when the ring was started at 13 mm (median cycle day 11) (206–215) (Level of evidence: I to II-3, fair, indirect). Bleeding patterns and other side effects did not vary with the timing of combined hormonal contraceptive initiation (204,205,216–220) (Level of evidence: I to II-2, good to poor, direct). Although continuation rates of combined hormonal contraceptives were initially improved by the “quick start” approach (i.e., starting on the day of the visit), the advantage disappeared over time (203,204,216–221) (Level of evidence: I to II-2, good to poor, direct).
Examinations and Tests Needed Before Initiation of Combined Hormonal Contraceptives
Among healthy women, few examinations or tests are needed before initiation of combined hormonal contraceptives (Table 4). Blood pressure should be measured before initiation of combined hormonal contraceptives. Baseline weight and BMI measurements might be useful for monitoring combined hormonal contraceptive users over time. Women with known medical problems or other special conditions might need additional examinations or tests before being determined to be appropriate candidates for a particular method of contraception. U.S. MEC might be useful in such circumstances (5).
Comments and Evidence Summary. Blood pressure: Women who have more severe hypertension (systolic pressure of ≥160 mm Hg or diastolic pressure of ≥100 mm Hg) or vascular disease should not use combined hormonal contraceptives (U.S. MEC 4), and women who have less severe hypertension (systolic pressure of 140–159 mm Hg or diastolic pressure of 90–99 mm Hg) or adequately controlled hypertension generally should not use combined hormonal contraceptives (U.S. MEC 3) (5). Therefore, blood pressure should be evaluated before initiating combined hormonal contraceptives. In instances in which blood pressure cannot be measured by a provider, blood pressure measured in other settings can be reported by the woman to her provider. Evidence suggests that cardiovascular outcomes are worse among women who did not have their blood pressure measured before initiating COCs. A systematic review identified six articles from three studies that reported cardiovascular outcomes among women who had blood pressure measurements and women who did not have blood pressure measurements before initiating COCs (170). Three case-control studies showed that women who did not have blood pressure measurements before initiating COCs had a higher risk for acute myocardial infarction than women who did have blood pressure measurements (222–224). Two case-control studies showed that women who did not have blood pressure measurements before initiating COCs had a higher risk for ischemic stroke than women who did have blood pressure measurements (225,226). One case-control study showed no difference in the risk for hemorrhagic stroke among women who initiated COCs regardless of whether their blood pressure was measured (227). Studies that examined hormonal contraceptive methods other than COCs were not identified (Level of evidence: II-2, fair, direct).
Weight (BMI): Obese women generally can use combined hormonal contraceptives (U.S. MEC 2) (5); therefore, screening for obesity is not necessary for the safe initiation of combined hormonal contraceptives. However, measuring weight and calculating BMI at baseline might be helpful for monitoring any changes and counseling women who might be concerned about weight change perceived to be associated with their contraceptive method.
Bimanual examination and cervical inspection: Pelvic examination is not necessary before initiation of combined hormonal contraceptives because it does not facilitate detection of conditions for which hormonal contraceptives would be unsafe. Women with certain conditions such as current breast cancer, severe hypertension or vascular disease, heart disease, migraine headaches with aura, and certain liver diseases, as well as women aged ≥35 years who smoke ≥15 cigarettes per day, should not use (U.S. MEC 4) or generally should not use (U.S. MEC 3) combined hormonal contraceptives (5); however, none of these conditions are likely to be detected by pelvic examination (145). A systematic review identified two case-control studies that compared delayed and immediate pelvic examination before initiation of hormonal contraceptives, specifically oral contraceptives or DMPA (95). No differences in risk factors for cervical neoplasia, incidence of STDs, incidence of abnormal Papanicolaou smears, or incidence of abnormal wet mounts were found (Level of evidence: II-2 fair, direct).
Glucose: Although women with complicated diabetes should not use (U.S. MEC 4) or generally should not use (U.S. MEC 3) combined hormonal contraceptives, depending on the severity of the condition (5), screening for diabetes before initiation of hormonal contraceptives is not necessary because of the low prevalence of undiagnosed diabetes and the high likelihood that women with complicated diabetes already would have had the condition diagnosed. A systematic review did not identify any evidence regarding outcomes among women who were screened versus not screened with glucose measurement before initiation of hormonal contraceptives (57). The prevalence of diabetes among women of reproductive age is low. During 2009–2012 among women aged 20–44 years in the United States, the prevalence of diabetes was 3.3% (84). During 1999–2008, the percentage of women aged 20-44 with undiagnosed diabetes was 0.5% (85). Although hormonal contraceptives can have some adverse effects on glucose metabolism in healthy and diabetic women, the overall clinical effect is minimal (171–177).
Lipids: Screening for dyslipidemias is not necessary for the safe initiation of combined hormonal contraceptives because of the low prevalence of undiagnosed disease in women of reproductive age and the low likelihood of clinically significant changes with use of hormonal contraceptives. A systematic review did not identify any evidence regarding outcomes among women who were screened versus not screened with lipid measurement before initiation of hormonal contraceptives (57). During 2009–2012 among women aged 20–44 years in the United States, 7.6% had high cholesterol, defined as total serum cholesterol ≥240 mg/dL (84). During 1999–2008, the prevalence of undiagnosed hypercholesterolemia among women aged 20–44 years was approximately 2% (85). A systematic review identified few studies, all of poor quality, that suggest that women with known dyslipidemias using combined hormonal contraceptives might be at increased risk for myocardial infarction, cerebrovascular accident, or venous thromboembolism compared with women without dyslipidemias; no studies were identified that examined risk for pancreatitis among women with known dyslipidemias using combined hormonal contraceptives (89). Studies have shown mixed results regarding the effects of hormonal contraceptives on lipid levels among both healthy women and women with baseline lipid abnormalities, and the clinical significance of these changes is unclear (86–89).
Liver enzymes: Although women with certain liver diseases should not use (U.S. MEC 4) or generally should not use (U.S. MEC 3) combined hormonal contraceptives (5), screening for liver disease before initiation of combined hormonal contraceptives is not necessary because of the low prevalence of these conditions and the high likelihood that women with liver disease already would have had the condition diagnosed. A systematic review did not identify any evidence regarding outcomes among women who were screened versus not screened with liver enzyme tests before initiation of hormonal contraceptives (57). In 2012, among U.S. women, the percentage with liver disease (not further specified) was 1.3% (90). In 2013, the incidence of acute hepatitis A, B, or C was ≤1 per 100,000 U.S. population (91). During 2002–2011, the incidence of liver carcinoma among U.S. women was approximately 3.7 per 100,000 population (92). Because estrogen and progestins are metabolized in the liver, the use of hormonal contraceptives among women with liver disease might, theoretically, be a concern. The use of hormonal contraceptives, specifically COCs and POPs, does not affect disease progression or severity in women with hepatitis, cirrhosis, or benign focal nodular hyperplasia (93,94), although evidence is limited; no evidence exists for other types of combined hormonal contraceptives.
Thrombogenic mutations: Women with thrombogenic mutations should not use combined hormonal contraceptives (U.S. MEC 4) (5) because of the increased risk for venous thromboembolism (228). However, studies have shown that universal screening for thrombogenic mutations before initiating COCs is not cost-effective because of the rarity of the conditions and the high cost of screening (229–231).
Clinical breast examination: Although women with current breast cancer should not use combined hormonal contraceptives (U.S. MEC 4) (5), screening asymptomatic women with a clinical breast examination before initiating combined hormonal contraceptives is not necessary because of the low prevalence of breast cancer among women of reproductive age. A systematic review did not identify any evidence regarding outcomes among women who were screened versus not screened with a breast examination before initiation of hormonal contraceptives (95). The incidence of breast cancer among women of reproductive age in the United States is low. In 2012, the incidence of breast cancer among women aged 20–49 years was approximately 70.7 per 100,000 women (96).
Other screening: Women with anemia, cervical intraepithelial neoplasia, cervical cancer, HIV infection, or other STDs can use (U.S. MEC 1) or generally can use (U.S. MEC 2) combined hormonal contraceptives (5); therefore, screening for these conditions is not necessary for the safe initiation of combined hormonal contraceptives.
Number of Pill Packs that Should Be Provided at Initial and Return Visits
- At the initial and return visits, provide or prescribe up to a 1-year supply of COCs (e.g., 13 28-day pill packs), depending on the woman’s preferences and anticipated use.
- A woman should be able to obtain COCs easily in the amount and at the time she needs them.
Comments and Evidence Summary. The more pill packs given up to 13 cycles, the higher the continuation rates. Restricting the number of pill packs distributed or prescribed can result in unwanted discontinuation of the method and increased risk for pregnancy.
A systematic review of the evidence suggested that providing a greater number of pill packs was associated with increased continuation (232). Studies that compared provision of one versus 12 packs, one versus 12 or 13 packs, or three versus seven packs found increased continuation of pill use among women provided with more pill packs (233–235). However, one study found that there was no difference in continuation when patients were provided one and then three packs versus four packs all at once (236). In addition to continuation, a greater number of pills packs provided was associated with fewer pregnancy tests, fewer pregnancies, and lower cost per client. However, a greater number of pill packs (i.e., 13 packs versus three packs) also was associated with increased pill wastage in one study (234) (Level of evidence: I to II-2, fair, direct).
Routine Follow-Up After Combined Hormonal Contraceptive Initiation
These recommendations address when routine follow-up is recommended for safe and effective continued use of contraception for healthy women. The recommendations refer to general situations and might vary for different users and different situations. Specific populations that might benefit from more frequent follow-up visits include adolescents, those with certain medical conditions or characteristics, and those with multiple medical conditions.
- Advise a woman to return at any time to discuss side effects or other problems or if she wants to change the method being used. No routine follow-up visit is required.
- At other routine visits, health-care providers seeing combined hormonal contraceptive users should do the following:
- Assess the woman’s satisfaction with her contraceptive method and whether she has any concerns about method use.
- Assess any changes in health status, including medications, that would change the appropriateness of combined hormonal contraceptives for safe and effective continued use based on U.S. MEC (e.g., category 3 and 4 conditions and characteristics).
- Assess blood pressure.
- Consider assessing weight changes and counseling women who are concerned about weight changes perceived to be associated with their contraceptive method.
Comments and Evidence Summary. No evidence exists regarding whether a routine follow-up visit after initiating combined hormonal contraceptives improves correct or continued use. Monitoring blood pressure is important for combined hormonal contraceptive users. Health care providers might consider recommending women obtain blood pressure measurements in other settings.
A systematic review identified five studies that examined the incidence of hypertension among women who began using a COC versus those who started a nonhormonal method of contraception or a placebo (123). Few women developed hypertension after initiating COCs, and studies examining increases in blood pressure after COC initiation found mixed results. No studies were identified that examined changes in blood pressure among patch or vaginal ring users (Level of evidence: I, fair, to II-2, fair, indirect).
Late or Missed Doses and Side Effects from Combined Hormonal Contraceptive Use
For the following recommendations, a dose is considered late when <24 hours have elapsed since the dose should have been taken. A dose is considered missed if ≥24 hours have elapsed since the dose should have been taken. For example, if a COC pill was supposed to have been taken on Monday at 9:00 a.m. and is taken at 11:00 a.m., the pill is late; however, by Tuesday morning at 11:00 a.m., Monday’s 9:00 a.m. pill has been missed and Tuesday’s 9:00 a.m. pill is late. For COCs, the recommendations only apply to late or missed hormonally active pills and not to placebo pills. Recommendations are provided for late or missed pills (Figure 2), the patch (Figure 3), and the ring (Figure 4).
Comments and Evidence Summary. Inconsistent or incorrect use of combined hormonal contraceptives is a major cause of combined hormonal contraceptive failure. Extending the hormone-free interval is considered to be a particularly risky time to miss combined hormonal contraceptives. Seven days of continuous combined hormonal contraceptive use is deemed necessary to reliably prevent ovulation. The recommendations reflect a balance between simplicity and precision of science. Women who frequently miss COCs or experience other usage errors with combined hormonal patch or combined vaginal ring should consider an alternative contraceptive method that is less dependent on the user to be effective (e.g., IUD, implant, or injectable).
A systematic review identified 36 studies that examined measures of contraceptive effectiveness of combined hormonal contraceptives during cycles with extended hormone-free intervals, shortened hormone-free intervals, or deliberate nonadherence on days not adjacent to the hormone-free interval (237). Most of the studies examined COCs (215,238–265), two examined the combined hormonal patch (259,266), and six examined the combined vaginal ring (211,267–271). No direct evidence on the effect of missed pills on the risk for pregnancy was found. Studies of women deliberately extending the hormone-free interval up to 14 days found wide variability in the amount of follicular development and occurrence of ovulation (241,244,246,247,249,250,252–255); in general, the risk for ovulation was low, and among women who did ovulate, cycles were usually abnormal. In studies of women who deliberately missed pills on various days during the cycle not adjacent to the hormone-free interval, ovulation occurred infrequently (239,245–247,255,256,258,259). Studies comparing 7-day hormone-free intervals with shorter hormone-free intervals found lower rates of pregnancy (238,242,251,257) and significantly greater suppression of ovulation (240,250,261–263,265) among women with shorter intervals in all but one study (260), which found no difference. Two studies that compared 30-µg ethinyl estradiol pills with 20-µg ethinyl estradiol pills showed more follicular activity when 20-µg ethinyl estradiol pills were missed (241,244). In studies examining the combined vaginal ring, three studies found that nondeliberate extension of the hormone-free interval for 24 to <48 hours from the scheduled period did not increase the risk for pregnancy (267,268,270); one study found that ring insertion after a deliberately extended hormone-free interval that allowed a 13-mm follicle to develop interrupted ovarian function and further follicular growth (211); and one study found that inhibition of ovulation was maintained after deliberately forgetting to remove the ring for up to 2 weeks after normal ring use (271). In studies examining the combined hormonal patch, one study found that missing 1–3 consecutive days before patch replacement (either wearing one patch 3 days longer before replacement or going 3 days without a patch before replacing the next patch) on days not adjacent to the patch-free interval resulted in little follicular activity and low risk for ovulation (259), and one pharmacokinetic study found that serum levels of ethinyl estradiol and progestin norelgestromin remained within reference ranges after extending patch wear for 3 days (266). No studies were found on extending the patch-free interval. In studies that provide indirect evidence on the effects of missed combined hormonal contraception on surrogate measures of pregnancy, how differences in surrogate measures correspond to pregnancy risk is unclear (Level of evidence: I, good, indirect to II-3, poor, direct).
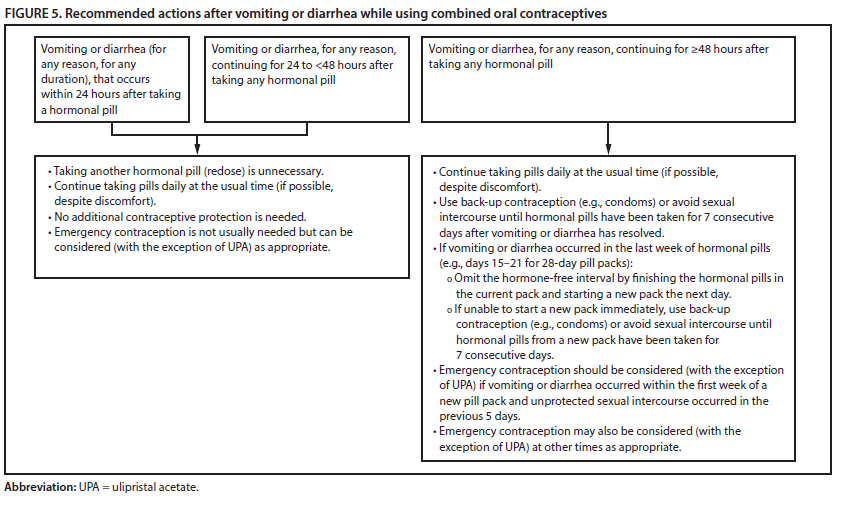
Vomiting or Severe Diarrhea While Using COCs
Certain steps should be taken by women who experience vomiting or severe diarrhea while using COCs (Figure 5).
Comments and Evidence Summary. Theoretically, the contraceptive effectiveness of COCs might be decreased because of vomiting or severe diarrhea. Because of the lack of evidence that addresses vomiting or severe diarrhea while using COCs, these recommendations are based on the recommendations for missed COCs. No evidence was found on the effects of vomiting or diarrhea on measures of contraceptive effectiveness including pregnancy, follicular development, hormone levels, or cervical mucus quality.
Unscheduled Bleeding with Extended or Continuous Use of Combined Hormonal Contraceptives
- Before initiation of combined hormonal contraceptives, provide counseling about potential changes in bleeding patterns during extended or continuous combined hormonal contraceptive use. Extended contraceptive use is defined as a planned hormone-free interval after at least two contiguous cycles. Continuous contraceptive use is defined as uninterrupted use of hormonal contraception without a hormone free interval (272).
- Unscheduled spotting or bleeding is common during the first 3–6 months of extended or continuous combined hormonal contraceptive use. It is generally not harmful and decreases with continued combined hormonal contraceptive use.
- If clinically indicated, consider an underlying gynecological problem, such as inconsistent use, interactions with other medications, cigarette smoking, an STD, pregnancy, or new pathologic uterine conditions (e.g., polyps or fibroids). If an underlying gynecological problem is found, treat the condition or refer for care.
- If an underlying gynecological problem is not found and the woman wants treatment, the following treatment option can be considered:
- Advise the woman to discontinue combined hormonal contraceptive use (i.e., a hormone-free interval) for 3–4 consecutive days; a hormone-free interval is not recommended during the first 21 days of using the continuous or extended combined hormonal contraceptive method. A hormone-free interval also is not recommended more than once per month because contraceptive effectiveness might be reduced.
- If unscheduled spotting or bleeding persists and the woman finds it unacceptable, counsel her on alternative contraceptive methods, and offer another method if it is desired.
Comments and Evidence Summary. During contraceptive counseling and before initiating extended or continuous combined hormonal contraceptives, information about common side effects such as unscheduled spotting or bleeding, especially during the first 3–6 months of use, should be discussed (273). These bleeding irregularities are generally not harmful and usually improve with persistent use of the hormonal method. To avoid unscheduled spotting or bleeding, counseling should emphasize the importance of correct use and timing; for users of contraceptive pills, emphasize consistent pill use. Enhanced counseling about expected bleeding patterns and reassurance that bleeding irregularities are generally not harmful has been shown to reduce method discontinuation in clinical trials with DMPA (124,125,274).
A systematic review identified three studies with small study populations that addressed treatments for unscheduled bleeding among women using extended or continuous combined hormonal contraceptives (275). In two separate randomized clinical trials in which women were taking either contraceptive pills or using the contraceptive ring continuously for 168 days, women assigned to a hormone-free interval of 3 or 4 days reported improved bleeding. Although they noted an initial increase in flow, this was followed by an abrupt decrease 7–8 days later with eventual cessation of flow 11–12 days later. These findings were compared with women who continued to use their method without a hormone-free interval, in which a greater proportion reported either treatment failure or fewer days of amenorrhea (276,277). In another randomized trial of 66 women with unscheduled bleeding among women using 84 days of hormonally active contraceptive pills, oral doxycycline (100 mg twice daily) initiated the first day of bleeding and taken for 5 days did not result in any improvement in bleeding compared with placebo (278) (Level of evidence: I, fair, direct).
FIGURE 2. Recommended actions after late or missed combined oral contraceptives
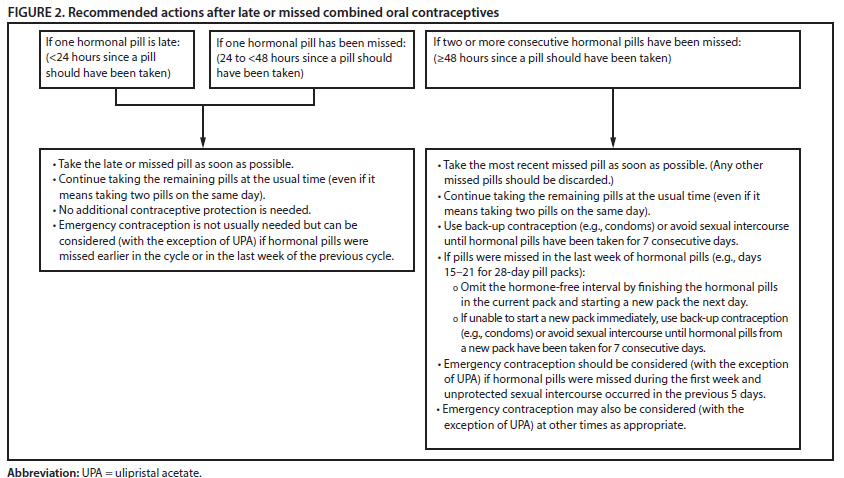
Alternate Text: Flow chart showing recommended actions after late or missed combined oral contraceptives.
FIGURE 3. Recommended actions after delayed application or detachment* with combined hormonal patch
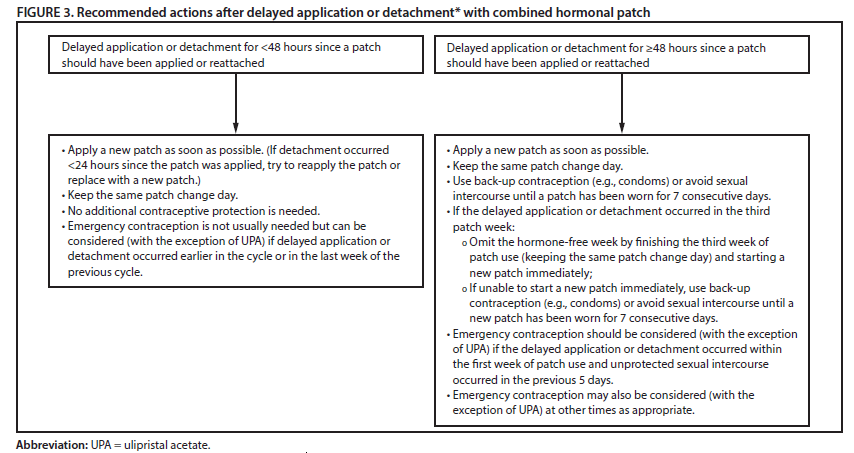
* If detachment takes place but the woman is unsure when the detachment occurred, consider the patch to have been detached for ≥48 hours since a patch should have been applied or reattached.
Alternate Text: Flow chart showing recommended actions after delayed application or detachment with combined hormonal patch.
FIGURE 4. Recommended actions after delayed insertion or reinsertion* with combined vaginal ring
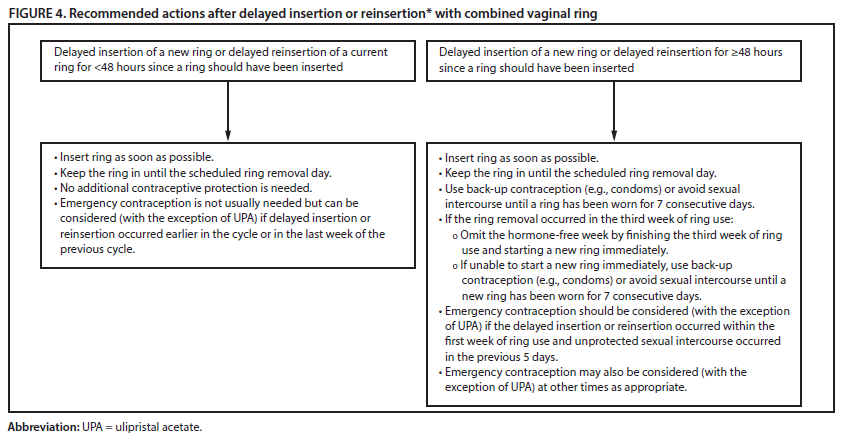
* If removal takes place but the woman is unsure of how long the ring has been removed, consider the ring to have been removed for ≥48 hours since a ring should have been inserted or reinserted.
Alternate Text: Flow chart showing recommended actions after delayed insertion or reinsertion with combined vaginal ring.
|
TABLE 4. Classification of examinations and tests needed before combined hormonal contraceptive initiation |
|
|---|---|
|
Examination or laboratory test |
Class* |
|
Examination |
|
|
Blood pressure |
A† |
|
Weight (BMI) (weight [kg]/height [m]2) |
—§ |
|
Clinical breast examination |
C |
|
Bimanual examination and cervical inspection |
C |
|
Laboratory test |
|
|
Glucose |
C |
|
Lipids |
C |
|
Liver enzymes |
C |
|
Hemoglobin |
C |
|
Thrombogenic mutations |
C |
|
Cervical cytology (Papanicolaou smear) |
C |
|
STD screening with laboratory tests |
C |
|
HIV screening with laboratory tests |
C |
|
Abbreviations: BMI = body mass index; HIV = human immunodeficiency virus; STD = sexually transmitted disease; U.S. MEC = U.S. Medical Eligibility Criteria for Contraceptive Use. * Class A: essential and mandatory in all circumstances for safe and effective use of the contraceptive method. Class B: contributes substantially to safe and effective use, but implementation may be considered within the public health and/or service context; the risk of not performing an examination or test should be balanced against the benefits of making the contraceptive method available. Class C: does not contribute substantially to safe and effective use of the contraceptive method. † In instances where blood pressure cannot be measured by a provider, blood pressure measured in other settings can be reported by the woman to her provider. § Weight (BMI) measurement is not needed to determine medical eligibility for any methods of contraception because all methods can be used (U.S. MEC 1) or generally can be used (U.S. MEC 2) among obese women (Box 1). However, measuring weight and calculating BMI at baseline might be helpful for monitoring any changes and counseling women who might be concerned about weight change perceived to be associated with their contraceptive method. |
|
- Page last reviewed: February 1, 2017
- Page last updated: February 1, 2017
- Content source: