


Captain Dies from Hyperthermia and Exertional Heatstroke While Performing Advanced Survival Training - Texas
 ShareCompartir
ShareCompartir
 Death in the Line of Duty...A summary of a NIOSH fire fighter fatality investigation
Death in the Line of Duty...A summary of a NIOSH fire fighter fatality investigation
F2012-27 Date Released: February 2014
Executive Summary
On September 15–16, 2012, a 46-year-old male volunteer captain (“Captain”) participated in a training course called Smoke Diver. Smoke Diver provides instruction in the advanced use of a self-contained breathing apparatus (SCBA) and advanced fire fighter survival skills. The course was taught by instructors from a component of a state fire fighter’s association at a private nonprofit fire fighter training facility. Participants performed such drills as air consumption, victim rescue, and self-rescue in a variety of situations while wearing personal protective equipment (PPE) that consisted of full turnout gear and SCBA. The training lasted approximately 12 hours on September 15, 2012, and approximately 10 hours on September 16, 2012. The heat index was 92.2 degrees Fahrenheit (°F) on September 15, 2012, and 90.3°F on September 16, 2012. Rehabilitation (rehab), in an unshaded area, occurred several times each day and consisted of doffing SCBA, partially removing turnout gear, resting, and drinking fluids.
On the first day of training, the Captain completed all the drills without incident. However, two trainees required evaluation and treatment by the on-scene paramedics: one for a medical condition exacerbated by heat stress, and the other for heat syncope treated on-scene with intravenous (IV) fluids. In addition, one student quit the program on the first morning because of training difficulties, and two additional students quit at the end of the day because they reportedly considered the training unsafe.
The next day, the Captain completed the drills throughout the day and was nearing the end of the last training drill known as the “tower.” The tower drill consisted of descending six floors of a concrete tower with each floor having an obstacle/drill. On the second floor the Captain had made his way through the “entanglement” simulation and exited the confined space box, when for unclear reasons, he re-entered the confined space room. An instructor monitoring the room noted that the Captain suddenly stopped moving. The instructor found the Captain unresponsive and called a mayday.
The Captain was carried down the interior stairs and outside the tower. Crew members removed the Captain’s gear while the on-scene paramedics and emergency medical technicians began an assessment. The Captain was found to be in cardiac arrest; cardiopulmonary resuscitation (CPR) and advanced life support (ALS) were begun as a transport ambulance was requested. The transport ambulance arrived 6 minutes later, and en route to the emergency department (ED) the ambulance crew found the Captain’s temperature to be 107.9°F (tympanic [ear] membrane). ALS continued as cooling treatments began with cool IV fluids and ice packs applied to the Captain’s skin. The Captain regained a pulse, but remained unconscious as the ambulance arrived at the ED.
In the ED the Captain’s core (rectal) temperature ranged from 104.4°F to 106.6°F. The Captain was hospitalized, and additional treatments for hyperthermia (cold IV fluids, fans, mist, cooling blanket, and ice packs) were administered. Treatment continued for over 24 hours, but complications of heatstroke developed, including rhabdomyolysis, acute renal insufficiency, acute respiratory failure, and hypoxic encephalopathy. On September 17, 2012, a brain scan showed results consistent with brain death. After consulting family members, the attending physician pronounced the Captain dead, and life support machines were turned off. The autopsy report listed the cause of death as “hyperthermia.” NIOSH investigators conclude that the Captain’s hyperthermia was caused by exertional heatstroke following heavy physical exertion in full PPE and severe environmental conditions with insufficient rehab.
According to the Smoke Diver coordinators, this was the first fatality in their 17-year history. However, numerous trainees in previous courses suffered from heat-related illness (HRI), that required emergency medical assistance either on-scene or in the ED. All 10 trainees in this course interviewed by NIOSH investigators reported symptoms consistent with mild to moderate HRI such as feeling hot, tired, fatigued, exhausted, nauseated, and having headaches. In addition to the Captain, two other trainees suffered heat syncope and heat exhaustion. The individual with heat syncope that occurred on September 15, 2012, was treated on-scene and recovered. The individual with heat exhaustion occurring on September 16, 2012, was transported to the ED and was subsequently hospitalized for 2 days. NIOSH considers cases of HRI to be “sentinel health events” [NIOSH 1986]. Sentinel health events are preventable diseases, disabilities, or deaths whose occurrence serves as a warning signal that preventive or therapeutic care may be inadequate [Rutstein et al. 1983].
A number of measures can prevent heat stress and HRI. Although the facility had a heat stress program, many components of the program were not initiated or followed by the instructors administering the training course. Five organizations have developed guidelines for stopping or restricting physical activity to prevent HRI on the basis of environmental conditions and the metabolic work requirements of the tasks being performed. All five organizations (U.S. Army, U.S. Air Force, American College of Sports Medicine [ACSM], the American Conference of Governmental Industrial Hygienists [ACGIH], and NIOSH) would have stopped the Smoke Diver training on both days. Therefore, NIOSH investigators recommend suspending the Smoke Diver program until all aspects of the training can be reviewed by a heat stress expert and a nationally recognized fire service safety officer. NIOSH offers the following recommendations to prevent heat stress and HRI:
Ensure a comprehensive rehabilitation program that complies with National Fire Protection Association (NFPA) 1584,Standard on the Rehabilitation Process for Members During Emergency Operations and Training Exercises, is in place and operating.
Ensure that all organizations that use the training facility comply with the facility’s heat stress program.
Strengthen the facility’s heat stress programby implementing the following recommendations before, during, and after all training courses at the facility:
BEFORE TRAINING
- Ensure trainees are medically cleared by a physician knowledgeable about NFPA 1582, Standard on Comprehensive Occupational Medical Program for Fire Departments, and the exertion required for the planned training.
- Ensure participants complete a screening checklist for heatstroke risk factors and the checklist is reviewed by the paramedics staffing rehab.
- Ensure students and instructors are educated, trained, and well versed in NFPA 1584.
- Schedule training involving heavy physical exertion in turnout gear during cooler seasons.
DURING TRAINING
- Measure environmental heat conditions using a wet bulb globe thermometer (WBGT).
- When WBGT criteria are exceeded:
- Discontinue physically demanding training according to the guidelines developed independently by the U.S. Army/Air Force and ACSM [Pennington et al. 1980; Armstrong et al. 2007; Nunneley and Reardon 2009].
- Implement a work-rest cycle recommended by ACGIH and NIOSH (Appendix 10,11a, and 11b).
- Follow and monitor fire fighters for signs of heat strain (temperature and pulse) regularly, but at a minimum during rehab [NFPA 2008c].
- Ensure trainees are hydrated at all phases of physically demanding tasks.
- Ensure ice water immersion therapy is readily available at the training facility to provide immediate treatment for heatstroke.
AFTER TRAINING
- Consider cases of HRI, particularly severe cases such as heatstroke, heat syncope, or rhabdomyolysis requiring medical treatment (e.g., on-scene IV hydration or transport) as a sign that the current heat stress program is inadequate or not being followed.
- Maintain a record of all injuries and illness suffered by trainees or trainers at the facility.
- Seek input from trainees and instructors about removing barriers, real or perceived, to reporting or seeking medical attention for heat strain or HRI.
- Require safety officers to review the planned training exercise and require their presence on all technically difficult/challenging training activities.
- Ensure that fire fighters, including training instructors, are trained in situational awareness and personal safety and accountability.
The following recommendations address safety issues noted during the NIOSH investigation. Although these safety issues probably delayed the identification and extrication of the Captain from the tower, they were not the primary causes of the Captain’s death.
Ensure that training maze props used in SCBA confidence training have adequate safety features such as emergency egress panels, emergency lighting, ventilation, and a temperature monitoring system to measure the ambient temperature inside the maze.
Ensure that personal alarm safety system (PASS) devices remain on during SCBA drills to signal if a fire fighter is lost or becomes unresponsive.
Ensure that training facility participants are equipped with radios and properly trained in mayday standard operating guidelines and survival techniques.
INTRODUCTION & METHODS
On September 16, 2012, a 46-year-old male volunteer Captain suffered exertional heatstroke during advanced fire fighter survival training and died the next day. NIOSH was notified of this fatality on September 17, 2012, by the deputy state fire marshal and on September 18, 2012, by the United States Fire Administration. On September 18, 2012, NIOSH contacted the Captain’s fire department to gather additional information and initiate the investigation. On October 15, 2012, three safety and occupational health specialists from the NIOSH Fire Fighter Fatality Investigation Team traveled to Texas to investigate the incident.
During the investigation, NIOSH personnel met with and interviewed the following people by phone or in person:
- Deputy state fire marshal
- Fire chief of the Captain’s fire department
- Deputy fire chief of the Captain’s fire department
- Training facility vice president
- Secretary/Treasurer of the Firemen and Fire Marshals Association
- Smoke Diver coordinator
- Lead instructors for the Smoke Diver course
- Floor instructors for the Smoke Diver course
- Paramedics from the standby contract ambulance
- Trainees
- Captain’s spouse
NIOSH personnel reviewed the following documents:
- Training facility safety manual
- Photographs of the training facility
- Fire department standard operating guidelines
- Captain’s personnel folder
- Captain’s training records
- Captain’s primary care physician medical records
- On-scene paramedic treatment records
- Emergency medical service/ambulance incident reports for the Captain and the trainee who was transported to the hospital ED the previous day
- Hospital ED records for the Captain and the trainee
- Autopsy report
RESULTS OF INVESTIGATION
Smoke Diver Course
In 1996, the East Texas Firemen's and Fire Marshals’ Association (ETFFMA) combined the curriculum from three different state programs to form the Texas Smoke Diver course. Also known as the “Advanced SCBA Training and Survival Course,” the program teaches experienced fire fighters advanced survival skills in full PPE including SCBA. The course objectives are to teach and instill proficency of air management techniques to improve survival when faced with an out of air emergency. The website for the course states, “The course is extremely challenging, intensely physical, and will take the student to his/her limit. Because of the difficulties some may experience, paramedics are on hand to monitor students before, during, and after each exercise” [ETFFMA 2012]. It was reported that the curriculum was approved by the state’s two fire fighter training regulatory agencies, the State Firemen’s and Fire Marshals’ Association for volunteer fire fighters and the Texas Commission on Fire Protection for career fire fighters in 1996, although those records were not located.
In the spring of 1996, 12–15 training instructors participated in a train-the-trainer class. Since 1996 there have been some changes to the class curriculum. Training tower obstacles and the rescue/extrication evolution were added to make the course more challenging. In addition, the duration of the course changed from 4 hours of training on Friday, 8 hours on Saturday, and 8 hours on Sunday to 10 hours of training on Saturday and 10 hours on Sunday.
Weather
As stated on the the training facility action plan, the weather forecast for Sunday, September 16, 2012, was a high temperature of 98°F with 58% humidity with a heat index of 107°F. (Note: According to the National Oceanic and Atmospheric Administration calculator, the forecasted heat index should have been 120°F, not 107°F) [NOAA 2012]. The actual weather conditions on September 15, 2012, included a high of 88°F, relative humidity of 53% (heat index of 92.2°F), sunny, with a slight wind of 7 miles per hour (mph). Conditions on September 16, 2012, included a high of 88°F, relative humidity of 48% (heat index of 90.3°F), sunny, with a slight wind of 3 mph [NOAA 2012].
Incident Day 1 – September 15, 2012
Registration began at 0630 hours. A number of “last resort” rescue techniques were taught to students arriving early (Appendix 1). The course began in the classroom with an introduction and 30-minute presentation on Smoke Diver fire safety. The safety presentation consisted of 57 slides that addressed the following: The National Fallen Firefighter Foundation’s 16 Firefighter Life Safety Initiatives, Course Question Attitudes (Photo 1), and Fire Fighter Line of Duty Deaths/Injuries [NFFF 2012]. This safety presentation did not mention heat stress, heat-related illness, rehab protocol, hydration concerns, rest breaks, or NFPA 1584, Standard on the Rehabilitation Process for Members During Emergency Operations and Training Exercises. However, pop-up tents, a rehab trailer, and several 5-gallon coolers filled with water or Gatorade® were available at the training ground.
After the classroom session, paramedics assigned to the Smoke Diver training course took baseline vital signs. The baseline vital signs consisted of heart rate, blood pressure, and an oxygen saturation reading. The Captain’s vital signs were: blood pressure of 147/87 millimeters of mercury [mmHg], heart rate 95 beats per minute, and oxygen saturation of 97%. Several students had high blood pressure; these results were relayed to the instructors, but all students were allowed to participate.
One student arrived late, and the entire class was required to perform push-ups as group punishment. The 22 students were then placed into four teams and completed the drills listed below (Appendix 2). All activities were conducted in full turnout gear (pants, jacket, boots, helmet, and gloves) with the exception of rehab during which the students could remove their jacket, helmet, and gloves, and turn down their turnout pants while wearing their boots and during lunch at which students could remove all their gear.
Morning activities: (0800 – 1200 hours)
- Don/doff the SCBA on the concrete drill pad, approximately 25 minutes
- Rehab on the unshaded metal bleachers, approximately 45 minutes
- Air consumption test on the concrete drill pad, approximately 90 minutes for all students
- Training tower orientation (floors, rooms, obstacles), 45 minutes
- SCBA emergency procedure classroom drill, 45 minutes (wearing turnout pants and boots)
Lunch: shaded pavilion (1200 – 1300 hours)
Afternoon activities: (1300 – 1700 hours)- Partial escape drill breaching walls on the tower’s third floor, 60 minutes for all students (5-10 minutes per student)
- Hot bottle swap (instruction only, no smoke, and not in full gear) on the tower’s fourth floor, 60 minutes for all students (5-10 minutes per student)
- Total escape drill on the tower’s second floor, 60 minutes for all students (5-10 minutes per student), pants and boots only
- Second hot bottle swap in a darkened metal shipping trailer outside the training tower, 30 minutes (10 minutes per student, darkened and smoky environment)
Several students had difficulty during the morning air consumption tests. One student quit the training because of course difficulty, and one other student was evaluated by the paramedics for abdominal pain. The paramedics were advised by the student that he had been recently diagnosed with an upper gastrointestinal bleed. The paramedics recommended to the student and the lead instructor that the student be evaluated in the local hospital’s ED. The student refused, and the lead instructor infomed the other instructors to watch the student for signs of medical problems.
Students reported to NIOSH investigators that their turnout gear was soaked with sweat by lunchtime. During lunch they tried to dry out the gear by turning the jackets inside out, but this was unsuccessful. Students were required to carry their spare SCBA cylinders throughout the course, and most used eight bottles during Day 1.
The Captain did not report any difficulties during Day 1. However, the Captain’s partner from his fire department had trouble with the hot bottle swap in the darkened metal shipping container. The exercise sometimes required the student to hold his or her breath for a short period, or, by using their hood, pulling the hood over the mask-mounted regulator opening and “filter breathe.” It was 120°F inside the trailer (estimated using a thermal imaging camera), and after being in the trailer for 20 minutes, the partner had to be removed by the lead instructor and was taken to the ambulance. The partner had not urinated in approximately nine hours, suggesting he had not consumed enough fluids. The paramedics took his vital signs, gave him “a popsicle, a pickle, and some pickle juice” and mentioned that IV fluids could only be administered at the hospital’s ED.
After resting 15 minutes and consuming the popsickle, pickle, and pickle juice, the Captain’s partner completed the three remaining drills at approximately 1630 hours. At this time he went to the ambulance for rehab, where paramedics administered IV fluids. He reported feeling better and was allowed to return for training the next day. The Captain and his partner left the training facility at approximately 1800 hours, but the Captain’s partner continued to feel ill and vomited throughout the night. Two students who completed the first day of training did not return the next day because they reportedly considered the training unsafe.
Incident Day 2 – September 16, 2012 (Appendix 3)
On Sunday, September 16, 2012, 19 of the original 22 students reported for training. Students’ turnout gear was still drenched with sweat from the first day of training. Vital signs were not taken at any time during the second day of training. The drills are listed below with the details provided in Appendix 3. Again, students were required to wear their turnout gear during all drills, but during rehab they could remove their jacket, helmet, and gloves, and turn down their turnout pants while wearing their boots and during lunch they could remove all gear.
Morning activities: (0800–1200 hours)
- Buddy breathe with mask-mounted regulator in the classroom, 60 minutes for all students
- Maze building drill: navigate numerous entanglements, 90 minutes (20 minutes per student)
- Rehab on the unshaded metal bleachers, 30–45 minutes
- Rescue drill in metal vessel: pull a 180-pound manikin through an open pipe (temperature approximately 120°F), 60 minutes (Photo 2)
Lunch: shaded pavilion (1200 – 1300 hours)
The Captain and his team began the morning with the rescue drill. The team struggled in the metal vessel because of the extremely hot and cramped conditions, and each team member consumed two SCBA bottles of air.
The Captain’s team then went to rehab, during which time they were instructed how to buddy breathe with mask-mounted regulators. However, there was no discussion of other recognized methods of rescue breathing such as RIT bag use, use of the buddy breather connection or the Universal Air Connection/Rapid Intervention Crew (UAC/RIC) connection, or how to make a connection to refill a downed fire fighter’s SCBA cylinder [Delmar Learning 2008]. Although trainees’ SCBAs were from different manufacturers, they all would have had a UAC/RIC connection, per NFPA 1981 [NFPA 2013b]. Therefore, students could have been trained on its use.
After the SCBA regulator instruction, the Captain’s team progressed to the maze building drill. The maze box was dark and hot. The drill was made more difficult by means to raise the students’ stress levels and disrupt the students’ concentration by harrassment (yelling, playing loud music, beating on objects, and throwing firecrackers) from the instructors. The Captain was the only student to complete the drill without running out of SCBA air. The Captain’s partner struggled during this drill. He was still feeling ill from the first day of training and a night of vomiting. He was approximately 15 feet from the door when the instructors continued to entangle him by looping a bungee cord around his SCBA bottle. The partner “feared for his life” and removed his facepiece. Removing one’s facepiece during a Smoke Diver drill causes the student to fail the entire course. Thus, the Captain’s partner was removed from the maze and he exited the maze building; he was withdrawn from the training course. Two additional students voluntarily withdrew from the course.
Afternoon activites – tower drill: (1300–1630 hours)
- Climb six flights of stairs (fire escape) of drill tower in full turnout gear with hand tool and spare SCBA bottle (not on air)
- Stage on sixth floor
- Descend interior stairs between sixth and fifth floors with passage impeded by fire hose strung between staircase handrails
- Fifth floor breech wall drill with obstacles in the room
- Descend stairs between fifth and fourth floors with passage impeded by fire hoses and plastic construction fencing between staircase handrails
- Fourth floor hot bottle swap
- Descend stairs between fourth and third floors with passage barricaded by fire hoses and plastic construction fencing between staircase handrails
- Third floor mazes, obstacles, and wall breech
- Descend stairs between third and second floors with passage barricaded by fire hoses and plastic construction fencing between staircase handrails
- Second floor obstacles and victim search in a room darkened by glycerin-based theatrical smoke
- Descend stairs between second and ground floor with passage barricaded by fire hoses and fencing
- Exit the drill tower
The 16 remaining students climbed the training tower’s exterior stairwell to the sixth floor. The Captain’s group, now comprised of himself and two students, started down the stairway to the fifth floor. Access and egress of the stairwell were hindered by 2-inch hoselines woven between the handrails and strung across the stairway. This required the students to lie on their back with the SCBA tank against the wall and stairs and descend the stairway upside down while carrying a handtool in one hand and a spare SCBA bottle in the other.
The Captain’s team arrived at the fifth floor and conducted a wall breech and maneuvered around several obstacles without incident. However, the SCBA low air alarm sounded on his partner’s SCBA while the other student was falling behind. On the fourth floor the students attempted a hot bottle change. At this point, one of the students on the Captain’s team quit the training course due to having chest pains; he was guided to paramedics who provided on-scene treatment. The student exited the tower through the window and down the fire escape stairway. In the darkness, heat, and harrassment the Captain crossthreaded his spare cylinder, and an instructor gave the Captain another bottle to thread. Spare cylinders were scattered around the floor, adding to the drill’s complexity.
The Captain and his partner, the only two remaining from the original team of four, started to descend the stairwell to the third floor. The hoses and plastic fencing encountered on the previous stairways were now more of a barricade rather than an obstacle. This stairway “barricade” from the second floor to the ground floor was minimally attached for quick removal in case of an emergency.
The Captain and his partner successfully navigated the obstacles and wall breach on the third floor. However, his partner was out of air and began “filter breathing” during his descent down the stairwell. An instructor at the second floor landing noted that the Captain was still “on air” when he went inside the second floor room through a 30-inch opening. The second floor objective was a victim search, described by students as a “hoarder’s house.” The obstacles included hoses and wooden landscaping timbers hanging from the ceiling; tires, pallets, golf balls, metal piping, and marbles were scattered across the floor (Photo 3 and Appendix 3). A large wooden box (Photo 4) was placed on the second floor, which required a right hand search evolution. The Captain was “filter breathing” (defined in Appendix 1) as he entered the wooden box that students had entered the day before without the obstacle.
The Captain and his partner were monitored with a thermal imaging camera as they exited the box and the room. The partner exited first, followed by the Captain. Then after a short time, for unclear reasons, the Captain re-entered the room. The Lead Instructor saw a student enter the room at the floor and start what appeared to be a left-hand search. Assuming the student was part of the next team, he advised the student to begin a right-hand search. The Instructor observed the student move forward another foot or two and witnessed the student stop moving. The Instructor moved toward the student, heard snoring sounds, found the Captain, and called the first mayday (1333 hours). The lead instructor then told the Captain’s partner to exit the room, but as he exited the room, the stairwell landing instructor told him to go back in and get the Captain. Learning of the mayday, the stairwell landing instructor pushed the partner down the stairwell as he rushed under the plywood nailed to the door frame. The partner tumbled down the stairwell, ripping through the construction fencing as he fell. Two instructors at the tower’s ground floor made the partner complete the last wall breach before exiting the tower.
Instructors executed the mayday preplan and carried the Captain out of the south side of the tower (students normally exit the tower on the north side) within about 30-45 seconds. Mayday Instructors removed his turnout gear and SCBA during the extrication process. Upon exiting the Tower, onsite medical personnel found him to be unresponsive, not breathing, and without a pulse; CPR was begun. A transport ambulance from the city fire department was requested (1336 hours). An automated external defibrillator was retrieved and applied, but the monitor revealed poor connectivity, presumably due to sweaty skin and not a defibrillator problem. The standby ambulance crew (one paramedic and two emergency medical technicians) arrived with a cardiac monitor, which revealed asystole. ALS was begun, which included an IV placement, administration of cardiac resuscitation medications, and intubation. At this point the Captain’s collapse was considered by the ambulance crew to be primarily a cardiac arrest rather than heatstroke.
The transport ambulance arrived at 1342 hours, and treatment was transferred to the city fire department ambulance personnel. A cardiac monitor revealed pulseless electrical activity, and intubation tube placement was verified by capnography [Neumar et al. 2010]. ALS continued as the Captain was loaded into the ambulance, which departed the scene at 1346 hours. Upon departure, the ambulance personnel used a digital thermometer to measure the Captain’s temperature. The rectal thermometer confirmed the tympanic temperature of 107.9°F.Treatment for hyperthermia began, including ice packs applied to his skin and infusion of cool IV fluids. En route (1348 hours), the Captain remained unconscious, but his pulse returned (152 beats per minute) with a blood pressure of 90/66 mmHg. Upon arrival at the hospital (1352 hours), his tympanic temperature was 105.2°F, and his blood pressure was 118/76 mmHg.
In the local hospital’s ED a rectal temperature of 104.4°F was noted at 1401 hours; an electrocardiogram showed sinus tachycardia (rapid heart beat), right bundle branch block, inferior infarction (age undetermined), and T-wave abnormalities. A repeat rectal temperature at 1425 hours was 106.6°F. The initial ED diagnoses were hyperthermia, heatstroke, and severe dehydration. The Captain was treated in the ED with ice packs, fans, cool IV fluids, cooling blanket, and cold saline lavage of his stomach and bladder. Approximately 2 hours later (1555 hours), his core temperature had decreased to a normal level of 98.8°F, and he was transferred to the intensive care unit. A repeat electrocardiogram showed the inferior ischemic changes had resolved, but the bundle branch block remained. Blood tests showed massive elevation of the muscle enzyme creatinephosphate kinase, diagnostic of rhabdomyolysis, and elevated troponin T levels, suggestive of myocardial damage [Punukollua et al. 2004].
Although his cardiovascular condition had stabilized, the Captain’s hospital course deteriorated from the following heatstroke complications:
- Rhabdomyolysis (the breakdown/death of muscle fibers resulting in the release of the contents of the muscle cells into the bloodstream) due to heavy physical exertion and/or prolonged hypotension
- Acute renal insufficiency due to rhabdomyolysis and/or prolonged hypotension
- Acute respiratory failure due to prolonged hypotension
- Hypoxic encephalopathy (brain damage due to lack of oxygen) due to prolonged hypotension and heatstroke.
A computed tomography scan of the brain and a nuclear medicine blood-brain barrier study showed results consistent with brain death. At 1740 hours on September 17, 2012, after consulting with family members, the attending physician pronounced the Captain dead, and life support machines were turned off.
Training Continues. Upon learning about the Captain’s heatstroke, cardiac arrest, and transport, the training facility requested that the instructors halt the training activities. The lead instructor, however, felt there was no reason to cancel the training. The training continued, and the lead instructor went to the office to provide his statement on the mayday events.
The remaining instructors were reshuffled to replace the lead instructor on the second floor. The next group of two students came into the second floor training room; both were “filter breathing.” Shortly after the students exited the confined space box, one student collapsed into the hanging hoselines. Another mayday was called as the student was rushed outside for emergency medical care. This student was transported to the ED where he was diagnosed with heat exhaustion and hospitalized for 2 days.
At this point the course was suspended, and all the students were removed from the training tower. Students were staged on the metal bleachers next to the training tower on the concrete training pad. At this time weather conditions included a temperature of 86°F, relative humidity of 55% (heat index of 89°F) with full sunshine and a slight wind of 6 mph. Vital signs were not taken, but the students had access to water and were allowed to doff their SCBA and turnout coat. The ETFFMA, the Texas A&M Engineering Extension Service, and the Smoke Diver instructors had a meeting to discuss continuation of the course. They decided that everyone had too much time and energy invested in the training course and, after consulting with the remaining students, sent the students back into the tower to complete the course. The remaining 13 students completed the tower drill without incident and therefore completed the Smoke Diver training course.
Medical Findings. The autopsy report, completed by the pathologist with the medical examiner’s office, listed the cause of death as “hyperthermia.” Pertinent findings from the autopsy, listed in Appendix 4, included no evidence of significant heart problems or other reason for his collapse other than exertional heatstroke. The Captain’s elevated troponin levels were considered to reflect myocardial damage due to his prolonged hypotension.
The Captain was 5'6″ tall and weighed 153 pounds, giving him a body mass index of 24.7 [CDC 2011]. He was physically fit, active on a daily basis, and acclimatized to hot weather because his duty station was in Texas. Over the past year he had been training for a triathlon and had lost about 57 pounds. He had previously been diagnosed with hypertension and high cholesterol; because of the weight loss, these conditions no longer required prescription medications. He had no history of HRI as a civilian or as a fire fighter. The Captain passed his fire department’s entrance physical agility test (Appendix 5) in July 2008.
DESCRIPTION OF THE FIRE TRAINING FACILITY
The city transferred operational control of the training facility to a nonprofit training and education organization in 2004. The organization allows contractors and other agencies (such as Smoke Divers) to utilize its facilities and the training props for “company sponsored” training programs. When a company sponsored training program such as Smoke Diver is presented, the organization requires the sponsoring company/contractor/agency to present a plan that includes training length, subject matter, field evolutions, oversight, safety, and emergency medical support. The facility provides all participants with a safety manual that identifies requirements for personal protective equipment, heat stress prevention, and facility safety.
Heat Stress Program. The training facility participant safety manual contained a section on heat stress prevention (Appendix 6).
Theatrical Smoke. The Smoke Diver program utilized glycerin-based theatrical smoke to darken some training rooms. This smoke can irritate the respiratory system [NIOSH 2013]. Instructors and students were frequently in training rooms darkened by theatrical smoke without the benefit of air from their SCBAs. The concentrations used would not likely present a health problem. If instructors or students complain of respiratory irritation, the use of the theatrical smoke should be stopped [NIOSH 2013].
Smoke Diver Program Application
- Student application (Appendix 7a)
- Basic SCBA training (Appendix 7b)
- Certification of physical fitness (Appendix 7c)
- Statement of physical fitness and medical history (Appendix 7d)
- Liability release (Appendix 7e)
Each application is reviewed and acceptance determined by two of the 12 ETFFMA elected board members who oversee the Texas Smoke Diver program. The Captain had 4 years of fire fighting experience and was certified as a State Basic Fire Fighter and Apparatus Operator. The Captain completed all these application forms and was accepted for the Smoke Diver training by the ETFFMA.
DISCUSSION
Hyperthermia, Heat-related Illness, and Heatstroke
Hyperthermia is characterized by an uncontrolled increase in body temperature that exceeds the body’s ability to lose heat [CDC 2006]. Exertional hyperthermia is defined as a core body temperature above 104°F during activity [Armstrong et al. 2007]. The Captain, who was involved in heavy physical exertion, had a tympanic membrane temperature of 107.9°F approximately 15 minutes after his collapse [Sund-Levander et al. 2002]. Rectal temperatures taken in the ED after cooling treatments had been initiated were greater than 104°F, confirming hyperthermia. Hyperthermia was listed as the diagnosis in the ED and as a cause of death on the autopsy report.
Heat sources for hyperthermia are external to the body (environmental) and internal to the body (metabolic heat produced during physical exertion). Heat stress is the sum of the heat generated from the body plus heat gained from the environment minus heat lost from evaporation [NIOSH 1986; ACGIH 2011]. Mild to moderate heat stress may cause discomfort, but is not harmful to health. As heat stress increases it causes heat strain, which is a physiologic response of the body. Heat strain manifests as increases in heart rate and core body temperature. As heat strain approaches human tolerance limits and core body temperature rises, the risk of HRI increases.
When individuals with hyperthermia become symptomatic, the condition is known as HRI. HRI represents a wide spectrum of conditions typically ranging in severity from skin rashes and heat cramps to heat exhaustion, heat syncope, and heatstroke. The milder HRI conditions (rash and cramps) do not necessarily precede the more severe conditions and, as this case suggests, heatstroke can be the presenting illness.
Heatstroke, the most severe form of HRI, is a life-threatening condition. It is defined as a core body temperature greater than 104°F with central nervous system disturbances and multiple organ system failure [Donoghue et al. 1997; Armstrong et al. 2007]. In the general population, heatstroke has a mortality rate of 33%–80% [Vicario et al. 1986; Seraj 1992]. When immediate cold/ice water immersion is administered for exertional heatstroke, studies suggest a dramatic reduction in mortality [Bouchama et al. 2007]. The Captain had heatstroke. Immersion/ice water supplies were not available at the facility.
Heatstroke is classified according to the primary source of the heat: internal (exertional) and environmental (classic). Exertional heatstroke tends to occur in younger, healthier persons such as military recruits and athletes. They generally present with sweat-soaked and pale skin at the time of collapse. Classic heatstroke tends to occur in elderly patients with chronic medical conditions. They generally present with dry, hot, flushed skin [Lugo-Amador et al. 2004]. The Captain’s presentation and clinical course, which followed training in severe environmental conditions, was typical of exertional heatstroke. During this training course, all trainees interviewed by NIOSH investigators reported symptoms consistent with mild to moderate HRI, two trainees suffered heat syncope and heat exhaustion, and the Captain suffered fatal heatstroke.
Risk Factors for Heat-related Illness and Exertional Heatstroke
Risk factors for HRI and exertional heatstroke involve metabolic heat generation, environmental heat load, clothing, acclimatization, and personal risk factors.
Metabolic Heat Generated During the Smoke Diver Training. For those engaged in moderate to heavy physical work, metabolic heat is the primary driver of heat stress. The metabolic heat generated by the Smoke Diver drills outside the classroom can be estimated by task analysis. Using the descriptions of the tasks reported to NIOSH during interviews and noted in the written procedures, NIOSH investigators estimate the trainees generated approximately 840 kilocalories per hour (kcal/hr) during the outside training drills (Appendix 8). This energy expenditure is considered very heavy exertion/work. It is consistent with estimates obtained during actual and simulated fire suppression in SCBA and turnout gear (660 to 767 kcal/hr) [Lemon and Hermiston 1977; O’Connell et al. 1986; Bugajska et al. 2007].
Environmental Heat Load. Environmental heat is determined by four factors: air temperature, humidity, air movement, and radiant heat. The commonly used “heat index” reported by the U.S. National Weather Service accounts for air temperature and humidity, whereas the WBGT index also accounts for radiant heat and wind [Minard 1961; Parsons 2006]. Thus, measuring or estimating the WBGT is important for two reasons. First, it is a more accurate index of environmental heat load. Second, it is used in HRI prevention guidelines [NIOSH 1986; Parsons 2006; Armstrong et al. 2007; ACGIH 2011].
In this incident, neither the training facility nor the course instructors had equipment to measure the WBGT. Formulas, however, have been developed that estimate WBGT using routinely collected meteorological data [Liljegren et al. 2008; ABM 2010; Lemke and Kjellstrom 2012]. At 1300 hours, shortly before the Captain collapsed, the dry bulb temperature was 88°F, the wet bulb temperature was 73°F, the humidity was 48%, and the wind was 3 mph with 0% cloud cover. Under these conditions, the Australian Bureau of Meteorology method would estimate the WBGT to be 30°C (86°F) (Appendix 9), although some have questioned the validity of the Australian Bureau of Meteorology method [Lemke and Kjellstrom 2012].
Clothing Adjustment Factor and Fire Fighter Turnout Gear. Heat is removed from the body primarily by evaporation of sweat from the skin. Clothing alters the amount and rate of heat exchange between the skin and the ambient air by convection, radiation, and evaporation [NIOSH 1986]. In general, the thicker the garment and the greater the air and vapor impermeability of the clothing, the more it interferes with the body’s cooling process. In evaluation heat stress, a “clothing adjustment factor” must be applied to the WBGT [NIOSH 1986; ACGIH 2011]. The turnout gear worn by fire fighters is a multilayer garment (three layers of outer shell, moisture barrier, and thermal liner) with partial air/vapor impermeability [Duffy et al. 2008]. A clothing adjustment factor of 6°C to 11°C (10°F to 20°F) for fire fighter turnout gear has been suggested [Pennington 1980; Bernard 1999; Duffy et al. 2008]. Thus, the effective WBGT would have been 36°C to 41°C (96.8°F to 105.8°F).
Acclimatization. Lack of heat acclimatization is another heatstroke risk factor. With heat acclimatization, physiological changes such as sweating at a lower temperature, more sweating, and less electrolyte loss make the body more efficient in dealing with heat stress. Any exercise program that builds and maintains a high level of aerobic fitness partially adapts the body to heat stress [Nunneley and Reardon 2009]. To fully acclimatize, however, the body needs to experience the actual work conditions in consecutively increasing 1½- to 2-hour increments. Adaptive physiological changes occur within 4 days, but complete acclimatization can take up to 3 weeks [Voltaire et al. 2002]. Once heat stress exposure stops, the body’s adaptive mechanisms regress; clinically significant reductions are seen within 4 days [ACGIH 2011]. The Captain in this incident was reasonably fit and acclimatized to hot and humid weather. It is unclear, however, if he was acclimatized to the environmental conditions present during the training, especially when performing physically demanding tasks wearing semipermeable turnout gear.
Personal Risk Factors. Personal risk factors for exertional heatstroke include increased age; obesity; poor physical fitness; a previous history of exertional heatstroke; and various medical conditions such as heart disease, renal disease, diabetes mellitus, skin conditions, sunburn, sweat gland dysfunction, viral illness, and diarrhea. Some medications reduce sweating (e.g., antihistamines); reduce cutaneous blood flow (e.g., stimulants such as cocaine, amphetamines, ephedrine, pseudoephedrine, caffeine, energy drinks, dietary supplements, theophylline); cause dehydration (e.g., diuretics); or inhibit central thermoregulation (e.g., neuroleptics and tricyclic antidepressants) [Armstrong et al. 2007]. The Captain was not known to have had any of these risk factors.
Other Risk Factors. Additional risk factors for HRI and heatstroke include dehydration, sleep deprivation and fatigue, and rhabdomyolysis [Armstrong et al. 2007]. The following discussion provides background on these issues and addresses whether they may have been a factor in this incident.
Dehydration occurs during prolonged exertion when fluid losses from sweating and rapid breathing are greater than fluid intake. The reduced intravascular volume associated with dehydration results in reduced blood flow to the skin (convection heat loss) and reduced sweating (evaporative heat loss), two of the body’s most important cooling mechanisms [Lugo-Amador et al. 2004]. Impaired cooling increases the body’s core temperature, which increases the risk of exertional heatstroke. Although the Captain was reported to have been drinking fluids during rehab and lunch, his autopsy finding of slightly elevated urea nitrogen levels suggested he was dehydrated [Collins 2011].
Although sleep deprivation and fatigue have been associated with exertional heatstroke, the relationship is not well established [Armstrong et al. 1990]. Although the Captain was fatigued from the previous day’s training, he was not sleep deprived.
Rhabdomyolysis. Severe physical exertion can precipitate rhabdomyolysis, the breakdown of muscle cells. This muscle breakdown process has been observed in fire fighters, particularly during physical fitness testing or training [CDC 1990; NIOSH 2012]. The Captain’s rhabdomyolysis and subsequent complications were probably due to three factors: extreme physical exertion, dehydration, and prolonged hypotension [Brown 2004; Sawka et al. 2007].
Guidelines for Workers/Athletes at Risk for Heat-related Illness and Exertional Heatstroke.
Several organizations have developed guidelines for stopping or restricting physical activities on the basis of WBGT, metabolic work requirements, and acclimatization. For heavy (415 kcal/hour) work among acclimatized individuals, the U.S. Army and Air Force cancel all scheduled physical training in acclimatized individuals when WBGT is above 32.0°C [Pennington et al. 1980; Nunneley and Reardon 2009]. The American College of Sports Medicine [ACSM 2009] recommends cancelling all scheduled events when WBGT is above 32.3°C [Armstrong et al. 2007]. For WBGT above 35°C, NIOSH recommends discontinuing heat exposure (work) for acclimatized workers on moderately physically demanding jobs (300 kcal/hour) [NIOSH 1986]. For WBGT above 31.5°C, ACGIH recommends discontinuing heat exposure (work) [ACGIH 2011]. These guidelines are based on an 8-hour workday and a 40-hour workweek. Using the NIOSH estimated WBGT of 36°C to 41°C, all the above organizations would have recommended cancelling the training.
Magnitude of the Problem: Heatstroke Fatalities.
The National Fire Protection Association (NFPA) reported seven heatstroke deaths from 2000 to 2011 [Fahy 2011]. All occurred during training exercises, three during live fire and four during physical fitness training. The occurrence of HRI symptoms and the cases of HRI that occurred during this training should have served as a warning that preventive or therapeutic care was inadequate.
Treatment.
Rapid core body temperature reduction is the most important treatment for exertional heatstroke. Its use has resulted in lower exertional heatstroke mortality rates [Castrini 1990; Bouchama et al. 2007; McDermott et al. 2009]. Cold/ice water immersion is the best method and is endorsed by the ACSM and the National Athletic Trainers’ Association [Binkley et al. 2002; Armstrong et al. 2007]. Cold/ice water immersion was not available on site.
RECOMMENDATIONS
Heat stress and HRI are preventable. Although the facility had a heat stress program, many components of the program were not initiated or followed by the instructors of the training course. NIOSH investigators recommend suspending the Smoke Diver program until all aspects of the training can be reviewed by a heat stress expert and a nationally recognized fire service safety officer. NIOSH recommends the following changes:
Recommendation #1: Ensure a comprehensive rehabilitation program complying with National Fire Protection Association (NFPA) 1584, Standard on the Rehabilitation Process for Members During Emergency Operations and Training Exercises, is in place and operating.
Rehabilitation operations should be provided in accordance with fire department standard operating procedures, NFPA 1500, Standard on Fire Department Occupational Safety and Health Program, and NFPA 1561, Standard on Emergency Services Incident Management System [NFPA 2008b; NFPA 2013a]. Rehabilitation efforts shall include the following:
- Relief from climatic conditions
- Rest and recovery
- Active and/or passive cooling or warming as needed for incident type and climate conditions
- Rehydration (fluid replacement)
- Calorie and electrolyte replacement as appropriate for longer duration incidents
- Medical monitoring
- Member accountability
- Release [NFPA 2008c]
The frequency and duration of the rehab periods were not adequate given the heavy work, extreme environmental conditions, and PPE worn by the trainees.
Recommendation #2: Ensure that all organizations that use the training facility comply with the facility’s heat stress program.
Provide a copy of the facility’s heat stress program to every organization that uses the training facility. When the organization contracts with the training facility, ensure that the organization has read and is capable of complying with the facility heat stress program.
Recommendation #3: Strengthen the facility’s heat stress program by implementing the following recommendations before, during, and after all training courses at the facility:
Recommendation #3a: BEFORE TRAINING
- Ensure trainees are medically by a physician knowledgeable about NFPA 1582, Standard on Comprehensive Occupational Medical Program for Fire Departments, and the exertion required for the planned training.
- Ensure participants complete a screening checklist for heatstroke risk factors and that the checklist is reviewed by the paramedics staffing rehab.
- Ensure students and instructors are educated, trained, and well versed in NFPA 1584.
- Schedule training involving heavy physical exertion in turnout gear during cooler seasons.
Recommendation #3b: DURING TRAINING
- Measure environmental heat conditions using a wet bulb globe thermometer (WBGT).
- When WBGT criteria are exceeded:
- Discontinue physically demanding training according to the guidelines developed independently by the U.S. Army/Air Force and ACSM [Pennington et al. 1980; Armstrong et al. 2007; Nunneley and Reardon 2009].
- Implement a work-rest cycle recommended by ACGIH and NIOSH (Appendix 10, 11a, and 11b).
- Follow and monitor fire fighters for signs of heat strain (temperature and pulse) regularly, but at a minimum during rehab [NFPA 2008c].
- Ensure trainees are hydrated at all phases of physically demanding tasks.
- Ensure ice water immersion therapy is rapidly available at the training facility to provide immediate treatment for cases of heatstroke.
Recommendation #3c: AFTER TRAINING
- Consider cases of HRI, particularly severe cases such as heatstroke, heat syncope, or rhabdomyolysis requiring medical treatment (e.g., on-scene IV hydration or transport) as a sign that the current heat stress program is inadequate or not being followed.
- Maintain a record of all injuries and illness suffered by trainees or trainers at the facility.
- Seek input from trainees and instructors about removing barriers, real or perceived, to reporting or seeking medical attention for heat strain or HRI.
Recommendation #4: Require safety officers to review the planned training exercise and require their presence on all technically difficult/challenging training activities.
NFPA Standard 1403 states that safety officers shall be appointed for all training sessions and have no other duties to interfere with their safety responsibilities. The safety officer should eliminate unsafe conditions, prevent unsafe acts, coordinate lighting of fires with the instructor-in-charge, ensure personal protective equipment compliance, and ensure all participants are accounted for before and after each evolution. The safety officer must have the authority to intervene and control all aspects of the operation [NFPA 2012]. Chapter 6 of NFPA 1521 Standard for Fire Department Safety Officer defines the role of the incident safety officer at various emergency incidents and identifies the necessary duties and responsibilities [NFPA 2008d].
In this incident, there was no appointed incident safety officer. Medical units were on the scene, and the safety role was carried out by the lead and assistant instructors. The multiple roles of the lead and assistant instructors in the training evolution may not have allowed sufficient focus on students’ safety and rehabilitation needs.
Recommendation #5: Ensure that fire fighters, including training instructors, are trained in situational awareness and personal safety and accountability.
All fire fighters operating at an incident or the training ground should maintain situational awareness and conduct a continuous risk assessment throughout the incident, reporting unsafe or changing conditions to the safety officer and the instructor in charge [NIOSH 2013]. Two trainees left the program because they considered the training unsafe. In addition, three trainees suffered severe HRI necessitating medical intervention, and all trainees experienced HRI symptoms. The training instructors were clearly aware of the extreme severe conditions and their effects on the trainees. In fact, the instructor in charge did not change, modify, or cancel the training despite two trainees being hospitalized for HRI. The instructor in charge and the entire Smoke Diver training staff need additional safety training, particularly in regard to heat stress and HRI.
The following recommendations address safety issues noted during the NIOSH investigation. Although these safety issues probably delayed the identification and extrication of the Captain from the tower, they were not the primary causes of the Captain’s death.
Recommendation #6: Ensure that training maze props used in SCBA confidence training have adequate safety features such as emergency egress panels, emergency lighting, ventilation, and a temperature monitoring system to measure the ambient temperature inside the maze.
In this incident, the Captain experienced a medical condition inside the training tower and had to be removed before medical assistance could be provided. The only egress was through the door blocked by a piece of plywood that was screwed into the door frame approximately 2 feet above the floor. When the Captain collapsed, the instructors had to drag the Captain under the plywood obstruction and down the obstructed stairwell in the dark. While these factors were not central to the cause of the Captain’s death, they did hinder his removal from the tower, and contributed to a slight delay of resuscitation efforts. NIOSH investigators recommend the training facility review NFPA 1402, Guide to Building Fire Service Training Centers, to construct a safe training prop [NFPA 2009].
Recommendation #7: Ensure PASS devices remain on during SCBA drills to signal if a fire fighter is lost or becomes unresponsive.
Fire fighters should wear SCBA and PASS whenever they are in immediately-dangerous-to-life-or-health (IDLH) or potentially IDLH environments. When operating in a non-IDLH environment the SCBA and PASS devices should work independently. If the fire fighters in the drill had not turned their PASS devices off after their SCBA ran out of air, the PASS devices would have activated in the alarm mode due to lack of motion. As a result, the instructor (s) may have realized the Captain was unconscious and located him faster.
Recommendation #8: Ensure that training facility participants are equipped with radios and properly trained in mayday standard operating guidelines and survival techniques.
In this incident, the Captain and his partner were out of air and were “filter” breathing as they negotiated a multitude of obstacles in a room darkened with theatrical smoke. The Captain had just exited the last obstacle (a 2′ × 2′ × 10′ plywood box) and appeared lost and confused according to his partner. While it is possible his confusion was due to the darkened conditions with heavy theatrical smoke, it is more likely that the Captain was experiencing heatstroke. If the Captain had a radio and was trained on calling a mayday, he may have alerted instructors that he was in trouble (Appendix 12).
REFERENCES
ABM (Australian Bureau of Meteorology) [2010]. Thermal comfort observations – wet bulb globe temperature. Australian government. [http://www.bom.gov.au/info/thermal_stress/#wbgt]. Date accessed: September 2013.
ACGIH [2011]. Heat stress and strain: documentation of TLVs and BEIs. Cincinnati, OH: American Conference of Governmental Industrial Hygienists.
ACSM [1984]. Prevention of thermal injuries during distance running – American College of Sports Medicine Position Stand. Med J Aust 8(22):876–879.
Armstrong LE, Deluca JP, Hubbard [1990]. Time course of recovery and heat acclimation ability of prior exertional heatstroke patients. Med Sci Sports Exerc 22(1):36-48.
Armstrong LE, Casa DJ, Millard-Stafford D, Moran D, Pyne SW, Roberts WO [2007]. Exertional heat illnesses during training and competition - American College of Sports Medicine Position Stand. Med Sci Sports Exerc 39(3):556–572.
Bachrach A, Egstrom G [1987]. Stress and performance in diving. San Pedro, CA: Best Publishing.
Bass DE [1963]. Thermoregularity and circulatory adjustments during acclimatization to heat in man. In: D Hardy, ed. Temperature: its measurement and control in science and industry. New York: Reinhold Publishing, pp. 299–305.
Bernard TE [1999]. Heat stress and protective clothing – an emerging approach from the United States. Ann Occup Hyg 43(5):321–327.
Binkley HM, Beckett J, Casa DJ, Kleiner DM, Plummer PE [2002]. Exertional heat illnesses – National Athletic Trainers’ position statement. J Athl Train 37(3):329–343.
Bouchama A, Dehbi M, Chaves-Carballo E [2007]. Cooling and hemodynamic management in heatstroke: practical recommendations. Crit Care 11(3):R54.
Brown TP [2004]. Exertional rhabdomyolysis. Early recognition is the key. Physician Sports Med 32(4):15–20.
Bugajska J, Zużewicz K, Szmauz-Dybko M, Konarska M [2007]. Cardiovascular stress, energy expenditure and subjective perceived ratings of fire fighters during typical fire suppression and rescue tasks. JOSE 13(3):323–331.
CDC (Centers for Disease Control and Prevention) [1990]. Exertional rhabdomyolysis and acute renal impairment -- New York City and Massachusetts, 1988. MMWR 39(42):751–756.
CDC (Centers for Disease Control and Prevention) [2006]. Heat-related deaths--- United States, 1999–2003. MMWR 55(29):796–798.
CDC (Centers for Disease Control and Prevention) [2011]. BMI – Body Mass Index. [www.cdc.gov/nccdphp/dnpa/bmi/adult_BMI/english_bmi_calculator/bmi_calculator.htm]. Date accessed: September 2013.
Clark BA [2005]. "Strategy and Tactics" - 500 Mayday called in rookie school. [http://www.firehouse.com/article/10498807/500-maydays-called-in-rookie-school]. Date accessed: September 2013.
Clark BA [2008]. Leadership on the line: firefighter Mayday doctrine—where are we now? Radio@Firehouse.com. [http://www.firehouse.com/podcast/10459336/leadership-on-the-line-firefighter-mayday-doctrine-where-are-we-now]. Date accessed: September 2013.
Collins KA [2011]. Postmortem vitreous analyses. [http://emedicine.medscape.com/article/1966150-overview#showall]. Date accessed: September 2013.
Costrini A [1990]. Emergency treatment of exertional heatstroke and comparison of whole body cooling techniques. Med Sci Sports Exerc 22(1):15–18.
Donoghue ER, Graham MA, Jentzen JM, Lifschultz BD, Luke JL, Mirchandani HG [1997]. Criteria for the diagnosis of heat-related deaths: National Association of Medical Examiners position paper. Am J Forensic Med Pathol 18(1):11–14.
Duffy RM, Roche K, Weider M, Stull J [2008]. Emergency Incident Rehabilitation. Washington, DC: Federal Emergency Management Agency. [http://www.iaff.org/hs/EIRP/index.html]. Date accessed: September 2013.
ETFFMA [2012]. Texas “smoke diver” training. East Texas Firemen’s & Fire marshal’s Association. [http://smokedivers.com/]. Date accessed: September 2013.
Fahy RF [2011]. Firefighter fatalities due to heat stroke in the United States–1999 to 2011. Personal communication. National Fire Protection Association, Quincy, MA.
Grossman D, Christensen L [2008]. On combat: the psychology and physiology of deadly conflict in war and peace. 3rd ed. Millstadt, IL: Warrior Science Publications.
IAFC Safety, Health, and Survival Section [2010]. Rules of engagement of structural firefighting [http://websites.firecompanies.com/iafcsafety/files/2013/10/ROE_Poster_FINAL1.pdf]. Date accessed: September 2013.
IAFF [2013]. IAFF Fire Ground Survival Program. Washington, DC: International Association of Fire Fighters [http://www.iaff.org/HS/FGS/FGSIndex.htm]. Date accessed: September 2013.
ISO (International Organization for Standardization) 8996 [2004]. Ergonomics of the thermal environment – determination of metabolic rate. Geneva, Switzerland.
Lemke B, Kjellstrom T [2012]. Calculating workplace WBGT from meteorological data – a Tool for climate change assessment. Ind Health 50:267–278.
Lemon PWR, Hermiston RT [1977]. The human energy cost of fire fighting. J Occup Med 19(8):558–562.
Liljegren JC, Carhart RA, Lawday P, Tschopp S, Sharp R [2008]. Modeling the WBGT using standard meteorological measurements. J Occup Environ Hyg 5(10):645–655.
Lugo-Amador NM, Rothenhaus T, Moyer P [2004]. Heat-related illness. Emerg Med Clin North Am 22(2):315–327.
McDermott BP, Casa DJ, Ganio MS, Lopez MR, Yeargin SW, Armstrong LE, Maresh CM [2009]. Acute whole-body cooling for exercise-induced hyperthermia: a systematic review. J Athl Train 44(1):84–93.
Minard D [1961]. Prevention of heat casualties in Marine Corps recruits. Mil Med 126(4):261–272.
NFFF [2012]. Everyone goes home. National Fallen Firefighters Foundation. [http://www.everyonegoeshome.com/]. Date accessed: September 2013.
NFPA [2008a]. Standard for fire fighter professional qualifications, Fire Fighter I and Fire Fighter II. Quincy, MA: National Fire Protection Association. NFPA 1001.
NFPA [2008b]. Standard on emergency services incident management system. Quincy, MA: National Fire Protection Association. NFPA 1561.
NFPA [2008c]. Standard on the rehabilitation process for members during emergency operations and training exercises. Quincy, MA: National Fire Protection Association. NFPA 1584.
NFPA [2008d]. Standard for fire department safety officer. Quincy, MA: National Fire Protection Association. NFPA 1521.
NFPA [2009]. Guide to Building Fire Service Training Centers Quincy, MA: National Fire Protection Association. [NFPA 1402.
NFPA [2012]. Standard on Live Fire Training Evolutions. Quincy, MA: National Fire Protection Association. NFPA 1403.
NFPA [2013a]. Standard on fire department occupational safety and health program. Quincy, MA: National Fire Protection Association. NFPA1500.
NFPA [2013b]. Standard on Open-Circuit Self-Contained Breathing Apparatus for Fire and Emergency Services. Quincy, MA: National Fire Protection Association. NFPA 1981.
NIOSH [1986]. Criteria for a recommended standard: occupational exposure to hot environments, rev. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, DHHS (NIOSH) Publication No. 86-113.
NIOSH [2012]. A career captain dies and 9 fire fighters injured in a multistory medical building fire—North Carolina. Morgantown, WV: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health. FACE Report F-2011-18. [http://www.cdc.gov/niosh/fire/reports/face201118.html]. Date accessed: September 2013.
NIOSH [2013]. Health hazard evaluation report: evaluation of chemical exposures during fire fighter training exercises involving smoke simulant. By Fent KW, Musolin K, Methner M. Cincinnati, OH: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, NIOSH HETA Report No. 2012-0028-3190.
NOAA [2012]. Quality controlled local climatological data: Southeast Texas Regional Airport, Beaumont/Port Arthur, TX September 15 and 16, 2012. [http://cdo.ncdc.noaa.gov/qclcd/QCLCD]. Date accessed: September 2013.
Neumar RW, Otto CW, Link MS, Kronick SL, Shuster M, Callaway CW, Kudenchuk PJ, Ornato JP, McNally B, Silvers SM, Passman RS, White RD, Hess EP, Tang W, Davis D, Sinz E, Morrison LJ [2010]. Part 8: Adult advanced cardiovascular life support. 2010 American Heart Association Guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Dallas, TX: American Heart Association.
Nunneley SA, Reardon MJ [2009]. Prevention of heat illness. In: Wenger CB, ed. Medical aspects of harsh environments.
[https://ke.army.mil/bordeninstitute/published_volumes/harshEnv1/Ch6-PreventionofHeatIllness.pdf]. Date accessed: September 2013.O’Connell ER, Thomas PC, Cady LD, Karwasky RJ [1986]. Energy cost of simulated stair climbing as a job-related task in fire fighting. J Occup Med 28(4):282–284.
Parsons K [2006]. Heat stress standard ISO 7243 and its global application. Ind Health 44(3):368–379.
Pennington JD, Crawford DL, Meyer EC, Arentzen WP, Allen L Jr [1980]. Occupational and environmental health – prevention, treatment, and control of heat injury. TB MED 507, NAVMED P-5052-5, AFP 160-1, Headquarters, Departments of Army, Navy, and Air Force. [http://www.med.navy.mil/directives/Pub/5052-5.pdf]. Date accessed: September 2013.
Punukollua G, Gowdaa RM, Khanb IA, Mehtab NJ, Navarroa V, Vasavadaa BC, Sacchi TJ [2004]. Elevated serum cardiac troponin I in rhabdomyolysis. Int J Cardiol 96(1):35–40.
Rutstein DD, Mullan RJ, Frazier TM, Halperin WE, Melius JM, Sestito JP [1983]. Sentinel health events (occupational): a basis for physician recognition and public health surveillance. Am J Public Health 73(9):1054–1062.
Sawka MN, Burke LM, Eichner ER, Maughan RJ, Montain SJ, Stachenfeld NS [2007]. American College of Sports Medicine position stand: exercise and fluid replacement. Med Sci Sports Exerc 39(2):377–390.
Seraj ME [1992]. Heat stroke during Hajj (pilgrimage): an update. Middle East J Anesthesiol 11(5):407–441.
Sund-Levander M, Forsberg C, Wahren LK [2002]. Normal oral, rectal, tympanic and axillary body temperature in adult men and women: a systematic literature review. Scand J Caring Sci 6(2):122–128.
U.S. Fire Administration [2006]. Mayday CD Q133 Firefighter safety: calling the Mayday and H134 Calling the Mayday: hands on training. Emmitsburg, MD: U.S. Department of Homeland Security, U.S. Fire Administration.
Vicario SJ, Okabajue R, Haltom T [1986]. Rapid cooling in classic heatstroke: effect on mortality rates. Am J Emerg Med 4(5):394–398.
Voltaire B, Galy O, Coste O, Racinais S, Callis A, Blonc S, Hertogh C, Hue O [2002].
Effect of fourteen days of acclimatization on athletic performance in tropical climate. Can J Appl Physiol 27(6):551562.INVESTIGATOR INFORMATION
This incident was investigated by one member of the NIOSH Fire Fighter Fatality Investigation and Prevention Program, Cardiovascular Disease Component in Cincinnati, Ohio and two members of the NIOSH Fire Fighter Fatality Investigation and Prevention Program, Traumatic Injury Component in Morgantown, West Virginia. Tommy Baldwin, MS, is a safety and occupational health specialist, a National Association of Fire Investigators certified fire and explosion investigator, an International Fire Service Accreditation Congress Certified Fire Officer I, and a former fire chief and emergency medical technician. Jay Tarley and Steve Miles are safety and occupational health specialists with the Fire Fighter Fatality Investigation and Prevention Program, Fatality Investigations Team, Surveillance and Field Investigations Branch, Division of Safety Research, NIOSH, in Morgantown, West Virginia. Thomas Hales, MD, MPH, provided medical consultation and coauthored the report. Dr. Hales is a member of the NFPA Technical Committee on Occupational Safety and Health, and Vice-Chair of the Public Safety Medicine Section of the American College of Occupational and Environmental Medicine.
Appendix 1
Definitions of “Last Resort” Rescue Techniques
The following training techniques were briefed prior to starting the course (Photo 5).
Hot Bottle Swap. This technique simulates a fire fighter swapping their empty air cylinder with a fresh cylinder while remaining in the hazardous environment of a structural fire. The swap is completed in a darkened room and requires the student to hold their breath during the operation.
The briefing described the technique as: Get down low, full escape from SCBA pack (unassisted), disconnect cylinder straps, take a breath and hold breath, close cylinder valve, bleed pressure with by-pass valve, unthread high pressure (HP) hose, remove cylinder, insert new cylinder, thread HP hose, open cylinder valve, breathe, restrap cylinder, and don SCBA (unassisted). The briefing also described the hazards of such an operation (Photo 6).
Filter Breathing. This technique requires the fire fighters who run out of air to remove their mask mounted regualtor (MMR) from their facemask. They are then required to pull their nomex hood from their neck area up and over the port for the MMR and “filter” breathe (Photo 7).
Bottle Breathing. This technique requires the fire fighters who run out of air to remove their MMR, cup their hand in front of the MMR port, and to breathe directly from their SCBA tank in a structural fire environment.
The briefing described the technique as: Get down low, partial escape, disconnect cylinder from HP hose, adjust bottle valve to control flow, insert air discharge into mask inhalation port or cup hands around face, and breathe from bottle air discharge. The hazards of such an operation were also briefed (Photo 8).
Severed Line Breathing. This technique requires the fire fighter who might have their low pressure line severed to remove their MMR and breathe directly from the low pressure line.
The briefing described the technique as: Get down low, adjust bottle valve to control flow, may require partial escape, insert air discharge into mask inhalation port or cup hands around face, and breathe from air discharge. The hazards of such an operation were also briefed (Photo 9).
Buddy Breathing. This technique is the only nationally approved standard operating procedure for an out-of-air emergency. It was taught in the classroom, but was not practiced during the hands-on training. The briefing did not describe any hazards associated with this technique.
Green – Green. This technique is safety language used between the instructors and students. The instructors would say “Green” and the students were to respond “Green.” It was used during the drills and rehab sessions to determine if the students could continue with the training. However, the teams were identified by color, including green. Therefore a “green” team member could mistakenly respond “green” based on his team designation instead of the health/condition of the member.
Appendix 2
Day One Itinerary/Timeline
TimeEvent/Drill0630
Registration/check-in.
0640Last resort rescue techniques (Appendix 1). 0700Introduction. Classroom session on the course objectives and fire fighter safety. 0730Baseline vital signs taken by paramedics.
0745Participants split into four groups (six firefighters per group).
0750Donning/doffing of SCBA. Four times on concrete drill pad in full turnout gear. One evolution must be 100% complete in less than 1 minute
0815Rehab on the unshaded metal bleachers. Remove turnout coat and turn down pants.
0900Air consumption drill on concrete pad using two bottles. The air consumption test consisted of each student dressing in full turnout gear with a full SCBA. The students were to go on air and navigate a series of obstacles outside on the concrete training pad and then climb the outside tower stairs to determine how long it would take each student to deplete their air supply. When the students consumed nearly all the air in their cylinder, they were instructed to go to a blue line on the concrete training pad and continue to use their SCBA until the air supply was totally depleted and the SCBA facepiece collapsed against their face. Only the instructors were allowed to remove the students’ masks at the end of this drill.
1030Room and obstacle orientation on the third floor of the tower
1115SCBA emergencies in the classroom
1200Lunch on the unshaded metal bleachers.
1300Partial escape breeching walls drill on the fifth floor of training tower. Students were to gear up and go on air in a darkened environment. They would negotiate a wall breach scenario and several obstacles across the floor toward the exit where the students would complete another wall breach that may require the students to remove their SCBA pack from their back in order to pass through simulated wall studs.
1400 Hot bottle swap drill on the fourth floor of the training tower. Students must swap their empty air cylinder with a fresh cylinder while in a darkened environment. This requires students to hold their breath during the operation. The drill’s degree of difficulty was increased by the spare empty cylinders rolling around on the floor. 1500 Total escape drill inside a 2′ × 2′ × 10′ wooden box on the second floor of the training tower (Photo 4). At the exit end of the box, a pole crossed the exit opening, which required the students to remove their SCBA pack inside the box and push the pack out of the box so they could navigate between the pole and the top or bottom of the box in order to exit. Their SCBA facepiece would remain in place and the students would put their SCBA pack back on once outside the box. 1600 Hot bottle swap drill outside the training tower inside a darkened metal shipping trailer. The the enclosed trailer was darkened with glycerin-based theatrical smoke.
1630 Finish drills.
The typical student would consume eight SCBA bottles during Day One.
Appendix 3
Day Two Itinerary/Timeline
TimeEvent/Drill0800
Buddy breathe with mask-mounted regulator in the classroom.
0900Maze building. The maze was constructed inside a 16′ × 32′ concrete block building. Obstacles were constructed from wooden materials to simulate ramps, stairs, drop-offs, windows, holes, and various entrapment hazards. Bungee cords were attached overhead so that instructors could entangle students as the students went through the maze to simulate an entanglement emergency. Instructors screamed, beat on drums, played extremely loud music, and threw lighted firecrackers at students to confuse and distract them.
1030Rehab. 1100Rescue drill in metal vessel. The metal vessel was constructed from large-diameter pipes. Students had to drag the 180-pound mannequin approximately 40 feet through a 5-foot diameter pipe to a “T” connection of a 2½-foot diameter pipe. Inside the smaller pipe students had to navigate the mannequin up and over a series of smaller pipes.
1200Lunch.
1300Tower drill consisting of the following:
a. Walk up fire escape in full turnout gear with hand tool and spare SCBA bottle.
b. Sixth floor staging.
c. Descend stairs to fifth floor while negotiating fire hose strung between handrails.
d. Fifth floor breech wall drill with several obstacles in the room.
e. Descend stairs to fourth floor while negotiating plastic construction fencing.
f. Fourth floor hot bottle swap.
g. Descend stairs to third floor while negotiating plastic construction fencing and fire hoses.
h. Third floor mazes and obstacles the students had to climb over, under, and through. There was another wall breech at the end of the third floor drills. Finally the door was blocked by a box nailed to the door. Students had to climb up and over the box to get out.
i. Descend stairs to second floor while negotiating plastic construction fencing and fire hoses.
j. Second floor, darkened by glycerin-based theatrical smoke, contained obstacles on the floor and dangling from the ceiling. The students were to conduct a right hand search navigating floor obstacles such as 4″ piping and burnt-out box springs. Landscape timbers were suspended 24 inches from the ceiling, 1-inch fire hose were suspended from sprinklers, with chicken wire and a tire with a wooden pallet tied to it. Additional box springs led to a 24″ × 24″ × 10′ wooden box. The far end of the box was off the ground on top of a 30-inch tall plastic barrel that emptied into a floored elevator shaft. Students were to turn around and go back through the box to finish their second floor right hand search. To enter and exit the second floor, students had to crawl under plywood attached to the doorway with a 24-inch crawl space.
k. Students then navigated the plastic construction fencing woven between the handrails down to the first floor and breech a bookcase to exit the structure.Appendix 4
Autopsy Findings
- Hyperthermia:
- 107.9°F (tympanic) at approximately 1345 hours in the field by city emergency medical services
- 105.2°F (tympanic) at approximately 1349 hours in the field by city emergency medical services
- 104.4°F (rectal) at approximately 1401 hours in the ED
- 106.6°F (rectal) at approximately 1425 hours in the ED
- Cardiac:
- Upper normal sized heart (440 grams) [Silver and Silver 2001]
- Left ventricular hypertrophy (1.5 centimeter [cm])
- Normal at autopsy is 0.76–0.88 cm [Colucci and Braunwald 1997]
- Normal by echocardiographic measurement is 0.6–1.0 cm [Connolly and Oh 2012]
- No evidence of conduction system abnormalities
- No evidence of heart valve problems
- Minimal coronary artery (35% stenosis of the left anterior descending coronary artery) atherosclerosis
- No evidence of recent heart attack (no blood clot in the coronary arteries)
- No evidence of a blood clot in the lung arteries (pulmonary embolus)
- Blood tests for drugs, alcohol, stimulants, or controlled substances were negative
- Vitreous (eye fluid):
- Sodium (147 mmol/L [normal is 135–150 mmol/L]), suggesting the Captain was not hyponatremic
- Urea nitrogen (31 mg/dL [normal is 8–20 mg/dL]), suggesting the Captain was dehydrated
REFERENCES
Colucci WS, Braunwald E [1997]. Pathophysiology of heart failure. In: Braunwald, ed. Heart disease. 5th ed. Philadelphia, PA: W.B. Saunders Company, p. 401.
Connolly HM, Oh JK [2012]. Echocardiography. In: Bonow RO, Mann DL, Zipes DP, Libby P, Braunwald E, eds. Heart disease: a text of cardiovascular medicine. 9th ed. Vol. 1. Philadelphia, PA: Elsevier Saunders, p. 216.
Silver MM, Silver MD [2001]. Examination of the heart and of cardiovascular specimens in surgical pathology. In: Silver MD, Gotlieb AI, Schoen FJ, eds. Cardiovascular pathology. 3rd ed. Philadelphia, PA: Churchill Livingstone, pp. 8–9.
Appendix 5
Physical Agility Test
The test is a timed event. Workout attire is permitted. At no time will running be allowed. The test is pass or fail based on the overall average time of the class. All events must be completed to pass. All events will run concurrently.
- The recruit will secure and carry a high rise pack to the top of the tower using each step.
- The recruit will place the high rise pack onto the floor and then hoist a 50-foot section of 1¾-inch hose to the top of the tower.
- The recruit will re-secure the high rise pack and proceed down the tower steps and place the pack on the ground at the base of the tower.
- The recruit will then secure a 100-foot section of 1¾-inch charged attack line and advance it the full length.
Appendix 6
Training Facility Participant Safety Manual
Heat Stress PreventionHeat stress is one of the greatest concerns for individuals involved in hands-on training activities. While heat stress is most prevalent during the warmer months of the year, participants and staff should be monitored for signs of heat stress throughout the year. To prevent heat stress, participants and staff should remove their helmet, hood, coat, and gloves during all critiques, breaks, and when moving from project to project. Increased cool down periods, shortened burn evolutions, and regular re-hydration will also help prevent heat stress. The following hydration guidelines should be followed to reduce the risk of heat stress:
- Drink ample water throughout the day:
- Drink a cup of water before and after each training evolution
- Limit the electrolyte consumption (too much could cause nausea)
- Do not drink the fire water used in training; potable water will be provided under the project shelters
- Limit alcohol consumption at night
- Do not eat a large lunch
- Notify your instructor of the first signs of heat stress
- Each shelter has a sign listing heat-related symptoms
Anyone exhibiting the signs/symptoms of heat stress should be removed immediately from the training activity and taken to a shaded location for cool down. Heat stress is a true medical emergency and can progress rapidly to heat stroke. Therefore, a qualified medic will be called to evaluate the individual’s condition at the first signs of heat stress. Participants and staff should closely monitor each other for the following signs/symptoms of heat stress.
Heat Cramps
- Muscle cramps in the extremities and abdomen
- Respiration rate increase
- Pale and moist skin
- Normal body temperature
- General weakness
Heat Exhaustion
- Heavy/Profuse sweating
- Rapid and weak pulse rate
- Rapid and shallow respiratory rate
- Pale and clammy skin
- Normal or decreased body temperature
- Irritability and restlessness
Heat Stroke
- Hot, dry, flushed skin
- Strong and pounding pulse
- Headache, dizziness, and dry mouth
- Seizure and coma
- Loss of consciousness and airway problems can occur
Appendix 7a
Student Application Package
Thank you for applying to attend the “Smoke Diver” school. The “Smoke Diver” school is an intense advanced SCBA and survival course. Requirements for attendance are very strict. You must be in good physical health with a thorough understanding of your departments SCBA. This course IS NOT the place to learn the basics or donning skills! Advanced survival skills will be taught and the student will graduate as a member of an elite group of “Smoke Divers”.
Class size is strictly limited to the first 24 “qualified firefighters”. Early registration is a must if you hope to have a seat. Enrollment will be limited to two firefighters per department if more than 24 apply. The Education Committee finalizes all decisions. A letter with course location, schedules, and personal equipment requirements will notify all personnel selected.
Participants must commit 100% toward completion of this program. The level of training will begin at a basic level and progress to the more difficult procedures through intermediate steps. Participants will not be subjected to undue difficulty at the beginning of the course, but as the course progresses the level of difficulty will increase. All objectives must be satisfactorily completed or a Certificate of Completion, the “Smoke Diver” patch and graduate tee shirt will not be awarded. Applicants who attend the course but do not pass all objectives will receive a “Certificate of Attendance”.
This school is NOT intended to be a macho firefighter program. It is however designed to train the firefighter to calmly handle potentially dangerous situations. Areas covered will be donning and quality, SCBA Maintenance and Cleaning Program, Air Consumption, Emergency Breathing Procedures, Room Orientation, Restricted Operations, Bottle Change in a hazardous atmosphere (not hazardous materials), Rescue, a Training Maze to simulate common obstacles, and an obstacle course.
Please complete the form below:Name:
MUST have your E-mail address:
Years in Fire Service/ Certification Level:
Basic SCBA Training Hrs?
Dept. Name
Age:
Address:
Home Phone #:
Cell Phone #
Fax #:City / State/ Zip Code:
Type of SCBA:
Shirt Size:
Appendix 7b
Basic SCBA Training
The firefighter named above has had a minimum of 8 hours of BASIC S.C.B.A. training hours.
Fire Chief or Training Officer Signature: _______________________________
ALL APPLICATIONS MUST BE RECEIVED BY . You will be notified in writing by
, if you have been accepted and what you will need to attend the class.
Make all payments to: :
RETURN TO:
Appendix 7c
- CERTIFICATION OF PHYSICAL FITNESS:
I certify that I am physically fit and able to participate in the above mentioned supervised Programs / Projects. I possess a full range of motion and sensory perception and I am able to perform all of the following activities except: (Circle any/all that apply)
Running Pulling Pushing Climbing
Crawling Scaling Lifting Dragging
I have been advised by my Physician to lift no more than _____________ lbs.List any other special limitations or instructions: ______________________________________________
____________________________________________________________________________________
____________________________________________________________________________________Name: _______________________________________ Department: _______________________________________
Address: _______________________________________ Address: _______________________________________ _______________________________________________ ____________________________________________________
Signature: ______________________________________Emer. Contact: _______________________________________
Appendix 7d
STATEMENT OF PHYSICAL FITNESS AND MEDICAL HISTORY
As a minimum requirement, this voluntary statement of Physical Fitness and Medical History Form MUST be completed prior to participation in the "Smoke Diver" Program, the "Flashover Project" and any live fire training. Due to some course intensities, extensive physical exertion and exposure to high temperatures (1000-1600F), students must certify a reasonable level of physical fitness and answer general questions designed to determine if the student has developed any condition which would make it too hazardous to participate in any of these activities.
STATEMENT OF PHYSICAL FITNESS AND MEDICAL HISTORY
II. MEDICAL HISTORY FORMThis MEDICAL HISTORY FORM must be completed in order for the student to participate in fire training activities. These questions are designed to determine if the student has developed any condition, which would make it hazardous to participate in the training activities.
During the past 12 months: Yes No
1. Have you been hospitalized? ____ ____
2. Did you have any injuries requiring medical attention? ____ ____
3. Did you have any illness lasting more than one week? ____ ____
4. Do you take medication regularly? ____ ____
5. Do you know of any reason why there should be limits to your
participation in any fire training activity? ____ ____
6. Have you ever suffered from heat exhaustion or heat stroke? ____ ____
7. Have you ever had a convulsion? ____ ____
8. Are you now under a doctor's care? ____ ____
9. Are you missing any paired organ (eye, kidney, etc.)? ____ ____
10. Are you wearing any removable dental appliance? ____ ____
11. Are you allergic to any medication (aspirin, Tylenol)? ____ ____
12. What year was your last tetanus booster given? ____ ____Any “Yes” answers to questions numbered 1, 2, 3, 4, 5, 6 or 7 will require completion of a PHYSICAL EXAMINATION and RELEASE STATEMENT from your FAMILY DOCTOR or CLINIC.
We will need a copy of this document faxed or mailed to us.
Please take this serious, we do. We have had recent heart surgery patients literally “sneak” into classes only to suffer from the extreme physical and mental demands of this course.
Appendix 7e
Liability Release
It is understood that even though the student will be wearing protective equipment, the possibility of an accident may still remain. Neither the or the
assumes any responsibility in case an accident does occur.
If, in the judgment of any representative of the , I should need immediate care and treatment as a result of any injury or sickness, I do hereby request, authorize, and consent to such care and treatment as may be given to me by any physician, instructor, nurse, or representative. I do hereby agree to indemnity and save harmless the or hospital representative from any claim by any person on account of such care and treatment rendered to me.
If, between this date and the beginning of the training activity, any illness or injury should occur that may limit my participation, I agree to notify the authorities of such illness or injury.Student Signature: _________________________________________
Date: _____________________
Witness Signature: _________________________________________
Date: _____________________Appendix 8
Estimated Metabolic Heat Production (in kilocalories per minute) During the Tower Drill, Day 2 of the Smoke Diver Training Course, by Task Analysis
[ACGIH 2011, ISO 2004, NIOSH 1986]Various Fire Fighter Positionskcal/min*A. Body position and movement
Intermittent walking up/down/crawling
2.0 kcal/min
B. Type of work –
Whole body – heavy7.0 kcal/min
C. Basal metabolism
Metabolic rate per minute
Total metabolic rate per hour1.0 kcal/min
10.0 kcal/min
600 kcal/hrD. Multiply by the weight correction factor**:600 kcal/hr x 1.4 = 840 kcal/hr
Total estimated metabolic rate = 840 kcal/hour
*For a standard male worker of 70 kilograms (kg) (154 pounds) body weight and 1.8 m2 (19.4 feet2) body surface [NIOSH 1986].
**The weight correction factor (WCF) is used when employee weight plus personal protection ensemble and equipment weigh more than 154 pounds (lbs). The WCF is calculated by dividing the sum of the employee’s current body weight (BW) and the PPE plus equipment weight (EW) by 154 lbs [WCF = (BW + EW) ÷ 154 lbs]. The Captain’s correction factor on September 16, 2012, was estimated to be (170 lbs + 60 lbs) ÷ 154 lbs = 1.4. This correction is very similar to the increase reported by the ISO 7243, which estimates an increase of 241 kcal/hour [Parsons 2006].
REFERENCES
ACGIH [2011]. Heat stress and strain: documentation of TLVs and BEIs. Cincinnati, OH: American Conference of Governmental Industrial Hygienists.
International Organization for Standardization (ISO) 8996 [2004]. Ergonomics of the thermal environment – determination of metabolic rate. Geneva, Switzerland.
NIOSH [1986]. Criteria for a recommended standard: occupational exposure to hot environments, rev. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, DHHS (NIOSH) Publication No. 86-113.
Parsons K [2006]. Heat stress standard ISO 7243 and its global application. Ind Health 44(3):368–379.
Appendix 9
Estimating Wet Bulb Globe Temperature
From Temperature and Relative Humidity*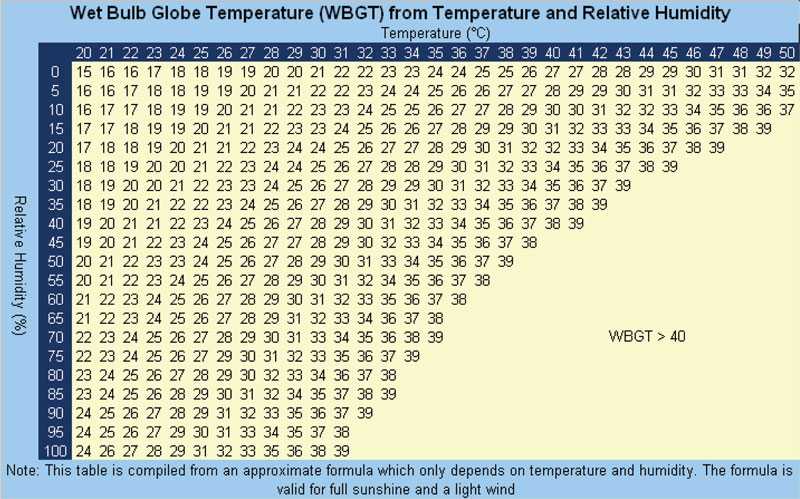
ABM (Australian Bureau of Meteorology) [2010]. Thermal comfort observations – wet bulb globe temperature. Australian government. [http://www.bom.gov.au/info/thermal_stress/#wbgt]. Date accessed: September 2013.
Appendix 10
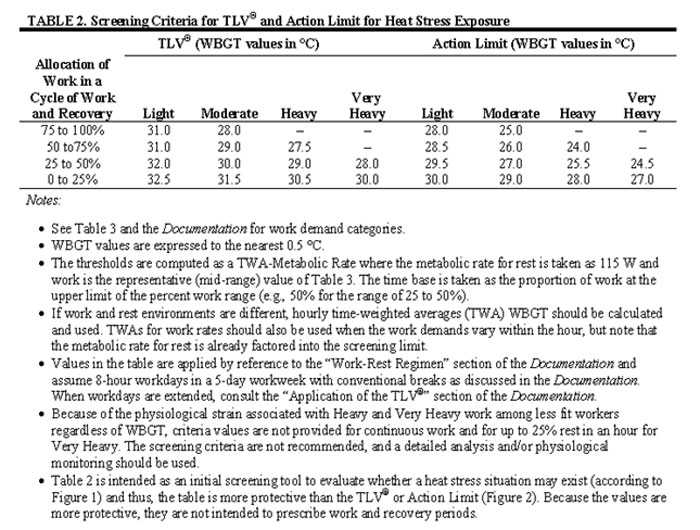
ACGIH [2011]. Heat stress and strain: documentation of TLVs and BEIs. Cincinnati, OH: American Conference of Governmental Industrial Hygienists.
Appendix 11a
NIOSH Recommended Heat Stress Alert and Heat-Stress Exposure Limits
Heat-Unacclimatized Individuals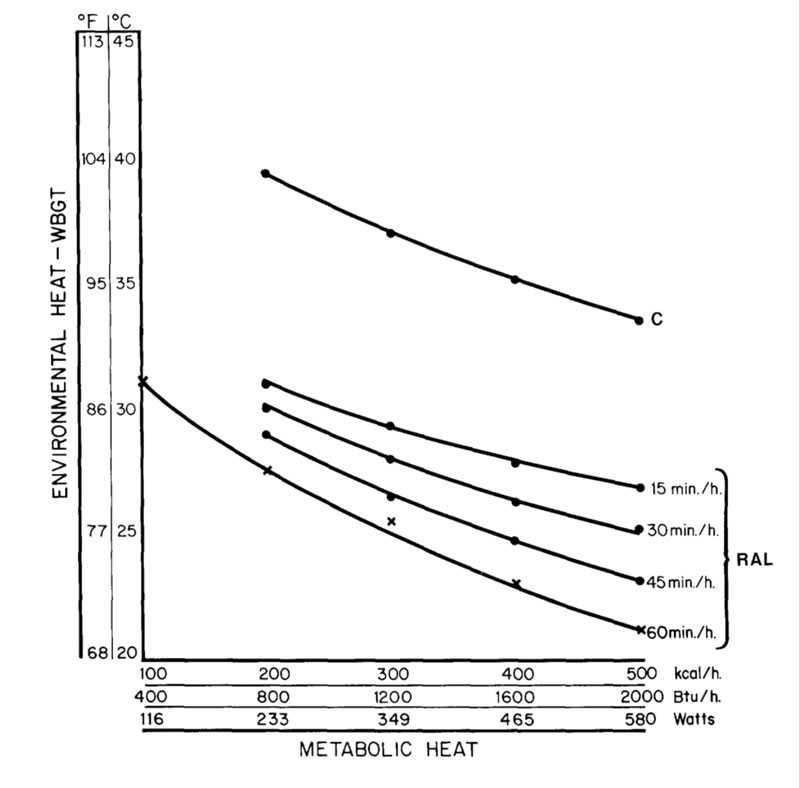
NIOSH [1986]. Criteria for a recommended standard: occupational exposure to hot environments, rev. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, DHHS (NIOSH) Publication No. 86-113.
Appendix 11b
NIOSH Recommended Heat Stress Alert and Heat-Stress Exposure Limits
Heat-Acclimatized Individuals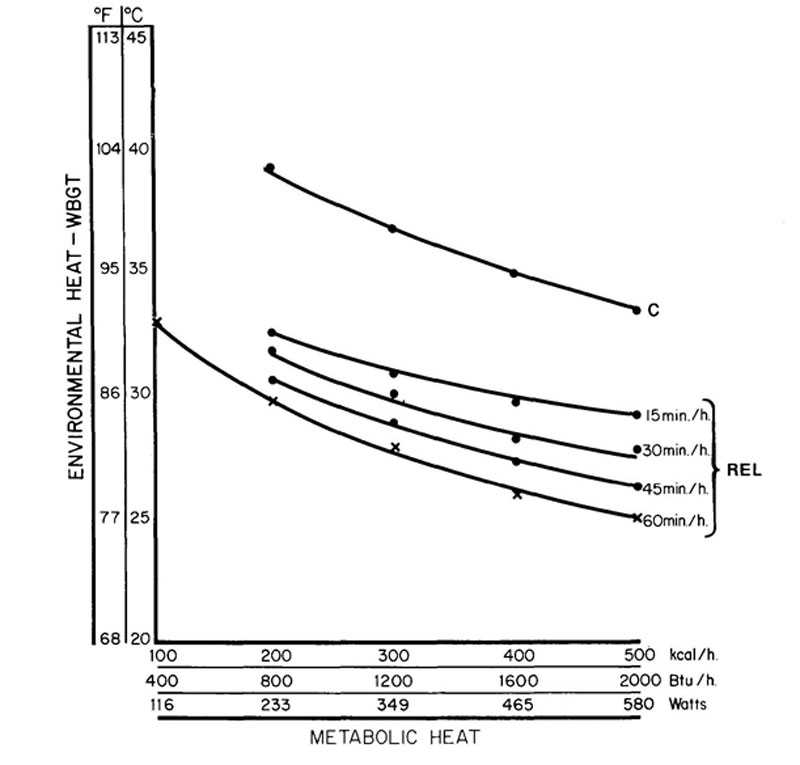
NIOSH [1986]. Criteria for a recommended standard: occupational exposure to hot environments, rev. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, DHHS (NIOSH) Publication No. 86-113.
NIOSH [1986]. Criteria for a recommended standard: occupational exposure to hot environments, rev. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, DHHS (NIOSH) Publication No. 86-113.
Appendix 12
Situational Awareness and Mayday Guidance
Fire fighters need to maintain situational awareness at all times while operating on the training ground. Fire fighters and trainees must understand that their personal protective equipment (PPE) and self-contained breathing apparatus (SCBA) do not provide unlimited protection, nor can an instructor always visually determine when a training participant is having difficulty. The ability of a fire fighter to call a mayday is a complicated behavior that includes the affective, cognitive, and psychomotor domains of learning and performance [Clark 2005; Grossman and Christensen 2008]. Any delay in calling a mayday reduces the chance of survival and increases the risk to other fire fighters trying to rescue the downed fire fighter.
Training should not be any different than what may actually take place on the fire ground. The training facility should ensure that trainees meet the authority having jurisdiction standards for mayday competency throughout their training evolutions. Presently there are no national mayday standards for firefighters to be trained to and most states do not have mayday standards. A rapid intervention team (RIT) will typically not be activated until a mayday is declared. Any delay in calling the mayday reduces the window of survivability and also increases the risk to the RIT [Clark 2005; U.S. Fire Administration 2006; Clark 2008; IAFC Safety, Health, and Survival Section 2010].
There are no rules regarding when a fire fighter must call a mayday, and mayday training is not included in the job performance requirements in NFPA Fire Fighter 1 or 2 standards [NFPA 2008a]. It is up to each authority having jurisdiction to develop rules and performance standards for a fire fighter to call a mayday. The National Fire Academy mayday courses present specific mayday parameters or rules for when a fire fighter must call a mayday. The courses may help fire departments in developing and teaching mayday procedures for fire fighters.
The National Fire Academy has two courses addressing the fire fighter mayday doctrine, Q133 Firefighter Safety: Calling the Mayday, which is a 2-hour program covering the cognitive and affective learning domain of the fire fighter mayday doctrine, and H134 Calling the Mayday: Hands-on Training, which is an 8-hour course that covers the psychomotor learning domain of the fire fighter mayday doctrine. These courses are based on the military methodology used to develop and teach fighter pilots ejection doctrine. A training CD is available to fire departments free of charge from the U.S. Fire Administration Publications office [Clark 2005; U.S. Fire Administration 2006].
Also, the IAFF fire ground survival program is another resource fire departments can use and was developed to ensure that training for mayday prevention and mayday operations are consistent between all fire fighters, company officers, and chief officers [IAFF 2013].
Any mayday communication must contain the location of the firefighter in as much detail as possible and, at a minimum, should include the division (floor) and quadrant. It is imperative that firefighters know their location when in immediately dangerous to life and health environments at all times to effectively be able to give their location in the event of a mayday. Once in distress, firefighters must immediately declare a mayday. The following example uses LUNAR (location, unit, name, assignment/air, resources needed) as a prompt: “Mayday, mayday, mayday, Division 1 quadrant C, Engine 71, Smith, search/out of air/vomited, can't find exit.” When in trouble, a firefighter's first action must be to declare the mayday as accurately as possible. Once the Incident Commander and RIT know the fire fighter's location, the firefighter can then try to fix the problem, such as clearing the nose cup, while the RIT is en route for rescue [U.S. Fire Administration 2006].
A fire fighter who is breathing carbon monoxide quickly loses cognitive ability to communicate correctly and can unknowingly move away from an exit or other fire fighters before becoming unconscious. Without the accurate location of a downed fire fighter, the speed at which the RIT can find them is diminished, and the window of survivability closes quickly because of lack of oxygen and high carbon monoxide concentrations in an immediately dangerous to life and health environment [Clark 2005; U.S. Fire Administration 2006; Clark 2008].
Fire fighters also need to understand the psychological and physiological effects of the extreme level of stress encountered when they become lost, disoriented, injured, run low on air, or become trapped during rapid fire progression. Most fire training curricula do not include discussion of the psychological and physiological effects of extreme stress, such as encountered in an imminently life-threatening situation, nor do they address key survival skills necessary for effective response. Understanding the psychology and physiology involved is an essential step in developing appropriate responses to life-threatening situations [NIOSH 2012]. Reaction to the extreme stress of a life-threatening situation, such as being trapped, can result in sensory distortions and decreased cognitive processing capability [Grossman and Christensen 2008]. In the book Stress and Performance in Diving, the author notes that while all training is important, “We know that under conditions of stress, particularly when rapid problem-solving is crucial, over-learning responses is essential. The properly trained individual should have learned coping behavior so well that responses become virtually automatic requiring less stop and think performance [Bachrach and Egstrom 1987].” Fire fighters should never hesitate to declare a mayday. There is a very narrow window of survivability in a burning, highly toxic building. Any delay declaring a mayday reduces the chance for a successful rescue [IAFC Safety, Health, and Survival Section 2010].
Photo 1. One of the Course Question Attitudes slides that was covered in the safety briefing
(Photo courtesy of course instructor)
Photo 2. Metal vessel that was used to for a rescue drill. (Photo courtesy of State Fire Marshal)

Photo 3. Second floor obstacles.
(Photo courtesy of State Fire Marshal)
Photo 4. Wooden box used for total escape drill and on the second floor where the maydays occurred on September 16, 2012.
Photo 5. Introductory slide to Smoke Diver course.
(Photo courtesy of course instructor)
Photo 6. Description of hazards slide associated with a hot bottle change. This is one of the techniques taught in the class that is not recognized as a nationally approved standard operating procedure for an out of air emergency. (Photo courtesy of course instructor)
Photo 7. Description of hazards slide associated with filter breathing. This is one of the techniques taught in the class that is not recognized as a nationally approved standard operating procedure for an out of air emergency.
(Photo courtesy of course instructor)
Photo 8. Description of hazards slide associated with bottle breathing. This is one of the techniques taught in the class that is not recognized as a nationally approved standard operating procedure for an out of air emergency. (Photo courtesy of course instructor)
Photo 9. Description of hazards slide associated with severed line breathing. This is one of the techniques taught in the class that is not recognized as a nationally approved standard operating procedure for an out of air emergency.
(Photo courtesy of course instructor)The National Institute for Occupational Safety and Health (NIOSH), an institute within the Centers for Disease Control and Prevention (CDC), is the federal agency responsible for conducting research and making recommendations for the prevention of work-related injury and illness. In 1998, Congress appropriated funds to NIOSH to conduct a fire fighter initiative that resulted in the NIOSH “Fire Fighter Fatality Investigation and Prevention Program” which examines line-of-duty-deaths or on duty deaths of fire fighters to assist fire departments, fire fighters, the fire service and others to prevent similar fire fighter deaths in the future. The agency does not enforce compliance with State or Federal occupational safety and health standards and does not determine fault or assign blame. Participation of fire departments and individuals in NIOSH investigations is voluntary. Under its program, NIOSH investigators interview persons with knowledge of the incident who agree to be interviewed and review available records to develop a description of the conditions and circumstances leading to the death(s). Interviewees are not asked to sign sworn statements and interviews are not recorded. The agency's reports do not name the victim, the fire department or those interviewed. The NIOSH report's summary of the conditions and circumstances surrounding the fatality is intended to provide context to the agency's recommendations and is not intended to be definitive for purposes of determining any claim or benefit.
For further information, visit the program Web site at www.cdc.gov/niosh/fire or
call toll free 1-800-CDC-INFO (1-800-232-4636).
- When WBGT criteria are exceeded:
- Page last reviewed: November 18, 2015
- Page last updated: October 15, 2014
- Content source:
- National Institute for Occupational Safety and Health Division of Safety Research