


A Career Captain Dies and 9 Fire Fighters injured in a Multistory Medical Building Fire—North Carolina
 ShareCompartir
ShareCompartir
 Death in the Line of Duty...A summary of a NIOSH fire fighter fatality investigation
Death in the Line of Duty...A summary of a NIOSH fire fighter fatality investigation
F2011-18 Date Released: June 25, 2012
Revised on September 27, 2012 to add an Additional Information Section
Executive Summary
On July 28, 2011, a 37-year-old career captain died and 9 fire fighters were injured in a 6-story medical building fire while searching for the seat of the fire. At 1228 hours, dispatch sent four companies (2 engines, 1 truck, and a squad company) to an automatic fire alarm at a multistory medical building. Engine 2 reported a working fire with heavy smoke and fire showing on the top floor rear of structure and requested a second alarm. Instead, the dispatch center sent a Division Chief, Battalion Chief, Safety Officer, Engine Company, Rescue company, and Fire Marshal as the complement for a working fire first alarm. Engine 2 fire fighters connected 100 feet of 2½-inch hoseline to the standpipe in the stairwell on the top floor. Engine 2 flowed water for several seconds when their low-air alarms went off and they exited the structure. Rescue 3 took the hoseline but had issues getting water to flow. The top two floors and north stairwell were now heavy with smoke. Ladder 1 was setting up at the A/B corner to access a window on the 6th level (labeled 5th floor), side B. Two of Rescue 3's members were getting low on air, and the crew moved to the stairwell to exit the building. Two of the members exited the stairwell, but the captain (the victim) went down the hallway and two fire fighters followed him. The low-air alarms of the victim and two fire fighters were sounding when they reached the hallway that was connected to the fire rooms. One of the fire fighters grabbed the victim, who was acting confused, and started back to the stairwell. The other fire fighter got separated in heavy smoke, went toward the fire room, and made it to a window where the platform of Ladder 1 was located just as he ran out of air. The victim ran out of air and told his partner they needed to buddy breath. The victim unclipped his regulator as his partner connected the buddy breather and all the partner's air escaped through the victim's SCBA. The victim transmitted a Mayday and activated his PASS (personal alert safety system). The fire fighter also attempted to activate his PASS, called several Maydays prior to removing his mask and began looking for an escape path. At some point, the victim vomited in his facepiece and removed it. The fire fighter crawled down a hallway trying to open several doors unsuccessfully until he found a door he could open to the south stairwell. The fire fighter placed his axe in the door and then returned to the victim. The fire fighter grabbed the victim and pulled him to the south stairwell where he collapsed and the pair fell down a flight of stairs. The victim and the fire fighter were eventually located in the south stairwell by another officer who had exited the north stairwell and heard the victim's PASS alarm sounding. Medic units transported the victim and the fire fighter to the hospital.

Area of fire origin – A/B corner
(Courtesy of Fire Department)
Contributing Factors
- Arson
- Lack of an automatic fire suppression system
- Multistory/high-rise standard operating procedures not followed
- Air management doctrine not followed
- Reverse stack effect in stairwell
- Inadequate strategy and tactics
- Task saturation of the incident commander
Key Recommendations
- Ensure that the existing standard operating procedures for high-rise fire-fighting operations are reviewed, implemented, and enforced.
- Ensure that a deployment strategy for low-frequency/high-risk incidents is developed and implemented.
- Ensure that the incident commander develops an incident action plan, which is communicated to all fire fighters on scene, and includes effective strategy and tactics for high-rise operations, a timely coordinated fire attack, and a coordinated search plan.
- Ensure that the incident commander utilizes division/group supervisors for effective tactical-level management.
- Ensure that fire fighters are properly trained in air management.
- Ensure that fire fighters are properly trained in out-of-air SCBA emergencies and SCBA repetitive skills training (e.g., buddy breathing and clearing a facepiece)
- Ensure that the incident commander is provided a chief's aide to assist in incident management, including communications and personnel accountability.
- Ensure that the incident commander establishes a stationary command post for effective incident management, which includes the use of a tactical worksheet, enhanced fireground communications, and a personnel accountability system.
- Ensure that fire fighters are properly trained in Mayday standard operating procedures and survival techniques.
Introduction
On July 28, 2011, a 37-year-old career captain died and 9 fire fighters were injured while searching for the seat of the fire in a six-story medical building. On August 1, 2011, the U.S. Fire Administration notified the National Institute for Occupational Safety and Health (NIOSH) of this incident. On August 7–12, 2011, a general engineer and two investigators from the NIOSH Fire Fighter Fatality Investigation and Prevention Program traveled to North Carolina to investigate this incident. The NIOSH investigators conducted an opening meeting with fire department officials. During the investigation NIOSH investigators met with the city's risk manager and with representatives of the North Carolina Occupational Safety and Health Administration. The NIOSH investigators visited the incident scene and conducted interviews with officers and fire fighters who were at the incident. The NIOSH investigators reviewed the fire department's standard operating guidelines, officers' and fire fighters' training records, dispatch audio tapes, and the county medical examiner's autopsy report. In addition, NIOSH investigators met with the Alcohol, Tobacco, and Firearms special agent who investigated the incident.
Fire Department
This career fire department has 12 stations with 237 uniformed members who serve a population of approximately 83,000 residents with a daytime population of 125,000 to 150,000 people within an area of about 60 square miles including contracted areas. The fire department responds to approximately 14,000 to 15,000 emergency calls annually. Specialty units consist of hazardous materials mitigation, swift water rescue, high angle rescue, dive rescue, and confined space rescue. All department members work a 24-hour duty shift (24 hours on, 24 hours off, 24 hours on, 48 hours off, 24 hours on, then 96 hours off). The fire department operates 17 companies consisting of 11 engine companies (includes 1 squad and 1 quint), 4 trucks, 1 rescue and 1 tender.
The fire department has written policies and procedures, which are available to all department members within their stations. Policies and procedures on the incident command system, personnel accountability system, high-rise operations, and truck company operations were in place.
Training and Experience
The state of North Carolina has specific requirements and recommendations to become either a volunteer or a career firefighter. First, you must be 18 years old with a high school diploma or GED and have a valid class C or better North Carolina driver's license. The state recommends a thorough physical exam conducted by a qualified medical practitioner, according to the current edition of the National Fire Protection Association (NFPA) 1582, Standard for Medical Requirements for Fire Service Personnel.1 Second, all fire fighters must complete training equivalent to the NFPA 1001, Standard for Fire Fighter Professional Qualifications, Fire Fighter I and Fire Fighter II.2 Third, a North Carolina Level I firefighter must be certified to Haz Mat (Hazardous Materials) Awareness and Haz Mat Operations. The training and experience for the victim, Captain (initial Incident Commander (IC)), and the IC are included in Table 1.
Table 1. Training and Experience of Key Personnel
Fire Fighter |
Training Courses |
Years experience |
|---|---|---|
Victim |
Fire Fighter I and II, Rapid Intervention Team Training, Hazardous Material Awareness and Operations, Hazardous Waste Operations and Emergency Response, Emergency Response to Terrorism Basic Concepts, Confined Space Rescue, Trench Rescue, High-Angle Rescue, Swift Water Rescue, and various administrative and technical courses. |
13 |
Captain (E2) |
Fire Fighter I and II, National Incident Management System Certification, Hazardous Materials Operations, Fire Ground Company Operations, Vertical Ventilation, and various administrative and technical courses. |
22 |
Division Chief (incident commander (IC)) |
Fire Fighter I, Fire Fighter II, Fire Inspector I, Hazardous Materials Training, National Incident Management System Certification, Command Officer Training, High-Angle Rescue, and various other administrative and technical courses. |
24 |
The fire department has a training classroom at headquarters and a training staff, which are led by the chief of training. The training division is responsible for all aspects of training and education for the department, including recruit training, in-service training for fire fighters and officers, and professional standards testing and certification. The division manages and facilitates much of the training with three training specialists who are assigned to each shift. The shift training officers also serve as incident safety officers (ISOs).
Structure
The incident involved an approximately 122,862-square-foot, six-story commercial structure, which contained numerous medical offices and was built in 1982 (see Photo 1). The commercial structure consisted of 5 upper floors, a ground floor, and a basement. The exterior construction was cast concrete panels reinforced by steel columns and I-beams and large glass window panels on every floor. The roof was flat and constructed of corrugated steel decking finished with a rubber membrane, asphalt, and approximately an inch thick layer of gravel. A parapet wall approximately 3 feet high surrounded the parameter of the roof. A steel and concrete mechanical room, which housed utilities for the structure, was located in the center of the roof.
The interior construction was drywall over metal studs, comprising numerous interior rooms and long hallways. The floors were poured concrete that were covered primarily with carpeting, but some areas were tiled. The ceilings were suspended acoustical tiles supported by a metal grid. A void space approximately 3 feet high was located between the drop ceiling and the steel decking of the floor above. The void spaces contained heating and cooling duct work and other utilities.

Photo 1. Side A of the fire structure;
skywalk and parking garage on the left.
(NIOSH photo.)
The building is accessed at the ground level by two main areas: a set of glass doors near the center of the structure on Side B (north) and Side A. Two steel personnel doors were on Side A, one near each end of the structure. On Side A of the structure, an enclosed skywalk connected floors 1 through 4 to the multilevel parking garage (see Photo 1 and Diagram 1). The structure had two internal stairwells (north and south) with an access to the roof and a set of internal elevators.
The structure was equipped with an automatic fire alarm. Note: The automatic alarm had false alarmed five times within the previous 30 days. The structure only had a single room on the 2nd floor that was sprinklered that contained a hyperbaric chamber. Note: The lack of sprinklers throughout this commercial structure significantly increased the health and safety exposure and risk to fire fighters. The structure was equipped with a wet standpipe system, which was supplied by an underground municipal water main on the east side of the structure. The standpipe went up to the top floor in both the north and south stairwells. Fire department connections (FDC) fed into the basement to the standpipe system, which served as a supplemental water supply. The FDC was designed to provide water to the standpipe system if the pressure in the FDC was greater than the pressure in the municipal water supply. A 2½-inch fire department hoseline connection with shutoff valve was supplied by the standpipe at each floor landing and housed in a metal cabinet. Each cabinet also contained 100 ft of 1½-inch house fire hose, which was for use by trained building occupants. The standpipe system included several screw and yoke valves, two gated shutoff valves, and a backflow preventer. All the valves were verified to be open at the time of the post fire incident investigation.
Several fire fighters stated and recorded radio traffic indicated that no water or water pressure was in the standpipe system. Also, some fire fighters observed a dirty black substance mixed with water at the standpipe fire department hoseline connection, which they believe may have clogged the water supply. During the incident, the hoseline that was deployed in the north stairwell was prematurely charged causing numerous kinks in the hoseline and possibly a partially open valve, which greatly inhibited water flow. Notes: 1) The Bureau of Alcohol, Tobacco, and Firearms (ATF) inspected, flow tested, pressure tested, and concluded that the standpipe was fully operational and functional as designed. In addition, the fire department, with NIOSH investigators observing, recreated the standpipe connection process and concluded that when the hoseline was properly deployed there was enough water pressure to put water on the fire. 2) The fire stairwell in the building had a significant volume of smoke from the 5th floor down to the lobby level due to entrainment from a phenomenon known as reverse stack effect. Reverse stack effect results from a temperature difference between warm outside and cooler inside air that creates a buoyancy driven downward flow of air (and smoke) from the top to the bottom of a tall building. Firefighters described the smoke in the stairwells as being very dense, stating that they were forced to breathe supplied air prior to arriving at the fire floor.
Personnel and Equipment
The fire department dispatched to the automatic alarm two engines, one truck, and a squad. Upon notification of a working fire, an additional engine, rescue company, division chief, battalion chief, safety officer, and a fire marshal were dispatched. Note: Engine 2 requested a second alarm, but due to multiple radio transmissions on the dispatch channel, it was missed by the communication center. The communication center never acknowledged the request and only dispatched the working fire units. Another alarm was not dispatched for 25 minutes. The 3rd alarm requested was actually the 2nd alarm dispatched. Table 2 identifies the apparatus and staff dispatched on the first-alarm and upgraded working fire, along with their approximate dispatch and on-scene arrival times (rounded to the nearest minute).
Table 2. First Alarm Equipment and Personnel Dispatched
Resource Designation |
Staffing |
Dispatched (rounded to minute) |
On-Scene |
|---|---|---|---|
Engine 1 |
Acting Captain |
1228 hrs |
1230 hrs |
Engine 2 (E2) |
Captain |
1228 hrs |
1229 hrs |
Ladder 1 (L1) |
Acting Captain |
1228 hrs |
1230 hrs |
Squad 1 (SQ1) |
Captain |
1228 hrs |
1230 hrs |
Division Chief 4 (DC4) |
Division Chief |
1233 hrs |
1235 hrs |
Safety Officer (SO) |
Safety Officer |
1233 hrs |
1235 hrs |
Battalion Chief 1 (BC1) |
Battalion Chief |
1233 hrs |
1246 hrs |
Engine 6 (E6) |
Captain |
1233 hrs |
1240 hrs |
Rescue 3 (R3) |
Captain (victim) EngineerFire fighter Second fire fighter (injured) arrived by POV |
1045 hrs |
1054 hrs |
Fire Marshal (FM) |
Fire Marshal |
1233 hrs |
1308 hrs |
Timeline
An approximate timeline summarizing the significant events of the incident is listed below. The times are approximate and were obtained by studying available dispatch records, photos, run sheets, witness statements, and fire department records. The times are rounded to the nearest minute. The timeline is not intended, nor should it be used, as a formal record of events.
- 1228 Hours
E1, E2, L1, and SQ1 are dispatched to an automatic alarm. - 1229 Hours
E2 arrived on scene, reports smoke showing, in command, and calls for 2nd alarm. - 1230 Hours
DC4, BC1, E6, R3, SO, and FM are dispatched to working fire; E1, L1, and SQ1 arrive on scene - 1232 Hours
E2 headed to 6th level (labeled 5th floor); evacuation process begins. - 1234 Hours
E1 hooked to FDC; E2 connected high-rise pack to 5th floor standpipe in north stairwell; E2 reported heavy smoke on 5th floor; E2 reported lower floors are clear of civilians. - 1235 Hours
DC4 and SO arrived on scene. - 1239 Hours
R3 arrived on scene and is assigned to conduct secondary search. - 1240 Hours
Engine 6 arrived on scene and is assigned fire attack; E1 established water supply to FDC. - 1243 Hours
R3 are on 1st floor. - 1244 Hours
E6 looked for mechanicals/utilities to shut down ventilation to 5th floor. - 1246 Hours
BC1 arrived on scene; SQ1 and E2 on fire floor. - 1248 Hours
Air Truck is requested; L1 on north side of structure. - 1249 Hours
E6 partially shut down ventilation to 5th floor. - 1250 Hours
SQ1 on the 5th reported heavy smoke and heat; E2 low on air and came out. - 1251 Hours
Fire room not located; High-rise pack stretched about 115 feet but has numerous kinks on 5th-floor landing and doorway. - 1252 Hours
R3 picked up hoseline but has no water; E1 connected to FDC to parking garage in case FDC was mislabeled. - 1254 Hours
E6 took air bottles to 3rd floor; Air Truck arrives. - 1255 Hours
L1 set up to attempt to flow water through 5th-floor window. - 1256 Hours
Fire room located; both FDCs charged; 3rd alarm dispatched (actually 2nd). - 1257 Hours
E1 reported still no water. - 1258 Hours
L1 repositioned for setup to 5th floor; R3 low on air and headed to north stairwell; Engine 8 (E8) en route. - 1259 Hours
R3 at stairwell; E2 back on fire floor; L1 does not deploy master stream due to crews on floor but broke window on north side to hand in a hoseline. - 1302 Hours
E2 got on their original hoseline and reported they are 30 feet short of the fire room and requested more hoseline; R3 exited structure. - 1304 Hours
E6 on ladder had 1¾-inch hoseline to hand through window. - 1308 Hours
E2 took out windows on west side but thought they were on north side (the 5th floor stairwell door was 90 degrees off from the pre-planned diagram); still no water on the fire; FM arrived on scene and starts taking photos. - 1309 Hours
E2 could not get to E6 with hoseline at north window because of fire and heat. - 1310 Hours
E6 made entry through window off ladder; E2 low on air and came out; R3 (now a crew of 5 (an E1 fire fighter and R3 fire fighter that had arrived by personal vehicle had joined up)), E1, Q5, and E8 made entry. - 1311 Hours
E6 got water on the fire for the first time. - 1314 Hours
R3 on original hoseline but reported to IC that there is no water; IC ordered R3 out. - 1315 Hours
E6 requested air bottles on fire floor. - 1316 Hours
E8 on fire floor, reported heavy smoke and heat, and requested ventilation of north stairwell. - 1317 Hours
R3 headed to the north stairwell. - 1318 Hours
Flames vented out broken windows on west side; a ladder truck was requested to west side. - 1319 Hours
E6 needed additional hoseline to hit fire on west side. - 1320 Hours
Mayday transmitted by victim in reception area. - 1321 Hours
Second Mayday transmitted by R3 fire fighter—out of air; E1 officer out of air and made it to T1's ladder at window and confirmed he did not call the Mayday. - 1322 Hours
Command realizes it is R3 that called Mayday, requests fireground channel change, and calls for a personnel accountability report PAR. Last Mayday transmitted by victim. - 1323 Hours
Mayday from R3 fire fighter on 5th floor on new fireground channel. - 1327 Hours
Last Mayday and report from R3 fire fighter—out of air. - 1341 Hours
E8 officer located victim and R3 fire fighter on stairwell landing between 2nd and 3rd floor of south stairwell.
Personal Protective Equipment
The victim and injured fire fighters were wearing a structural fire-fighting coat and pants, gloves, hood, boots, structural fire-fighting helmet with eye protection, self-contained breathing apparatus (SCBA) with an integrated personal alert safety system (PASS), and a radio. The National Personal Protective Technology Laboratory (NPPTL) evaluated the SCBAs of the victim and injured R3 fire fighter and the summary evaluation report is included as Appendix 1. The full report can be provided upon request. The victim and injured R3 fire fighter's structural fire-fighting gear and personal protective equipment (PPE) were also examined by NPPTL to determine conformity to the National Fire Protection Association (NFPA) voluntary consensus standards. Note: This evaluation report will be added to this report as Appendix 2, when completed. NIOSH investigators do not believe that the PPE had any direct contribution to the fire fighter's death. NIOSH investigators did observe dried vomitus inside the nose cup of the victim's facepiece.
Weather
The weather was clear with an approximate temperature of 87°F. The relative humidity was 46% and the wind was variable at 4 - 6 miles per hour.3 The weather may have had an impact on the incident (see Note in Recommendation #6).
Investigation
On July 28, 2011, at1228 hours, dispatch sent E1, E2, T1, and SQ1 to an automatic fire alarm at a multistory medical building. Upon arrival at 1229 hours, the E2 captain reported a working fire with heavy smoke and fire showing on the top floor rear of the structure and requested a second alarm. DC4, BC1, E6, R3, SO, and FM were dispatched to fill the "working fire" dispatch, but a second alarm was not dispatched as it was missed by the communications center due to multiple radio transmissions on the dispatch channel. At 1232 hours, E2's captain and fire fighter made entry on Side A of the structure with 150 feet of 2½-inch hoseline in a high-rise pack. They met the structure's maintenance personnel near the lobby who had been evacuating civilians. The E2 crew used the elevator without putting it in "fireman mode" and took it to the 4th floor. On the 4th floor, the E2 captain passed command to the next arriving officer and advised civilians to evacuate. After observing the 5th floor A/B corner from the 4th floor parking garage skywalk, the E2 crew went back and took the elevator to the 5th floor.
At 1234 hours, E1 staged on Side C to hook up to the FDC and to pump through the standpipe system. The E2 crew went on air and reported heavy smoke and intense heat as they located the standpipe connection at the 5th floor landing of the north stairwell. They began to connect the high-rise pack. DC4 arrived on scene and assumed Command of the incident. The safety officer (SO) arrived and tried to initiate accountability. L1, E1, and SQ1 crews were conducting primary searches on lower floors to evacuate civilian personnel. At 1239 hours, R3 arrived on scene and was assigned secondary search and rescue responsibilities.
A minute later, E6 arrived and was assigned fire attack (see Diagram 1). The E1 engineer notified Command that water was established at the FDC to the standpipe system. At 1244 hours, E6 was looking for the mechanical room to shut down ventilation to the 5th floor while R3 was going up the north stairwell. At 1246 hours, BC1 arrived on scene and was assigned rehab and to assist with the personnel accountability. L1 set up on Side B of the building near the A/B corner. Within the next several minutes, E6 had partially shut down the ventilation to the 5th floor, and E2 had stretched the uncharged hoseline about 115 ft clockwise around the north stairwell and elevators to a large room (reception area) just prior to the hallway to the A/B corner (see Diagram 2). Note: In the pre-plan of the structure, the doorway of the North stairwell opened into the west hallway but the door was moved 90 degrees. Also, the door adjacent the stairwell door was closed and thought initially to be a wall. This prompted the E2 crew to go clockwise stretching the hoseline.
Several crews using the stairwell had dropped additional high-rise packs in the stairwell. The hoseline was inadvertently charged, causing multiple kinks on the 5th floor between the standpipe connection and the 5th floor doorway. The E2 crew, stretching the hoseline, noticed it was charged and flowed water for a few seconds to cool down the area. At 1251 hours, the E2 crew's SCBA low-air alarm began going off so they used the elevators to return to the ground floor to change SCBA cylinders. Approximately one minute later, the R3 crew on the 5th floor grabbed the hoseline, could not get water to flow, and reported it to Command. The E1 engineer proceeded to connect to the FDC for the parking deck standpipe system in case they had been mislabeled.
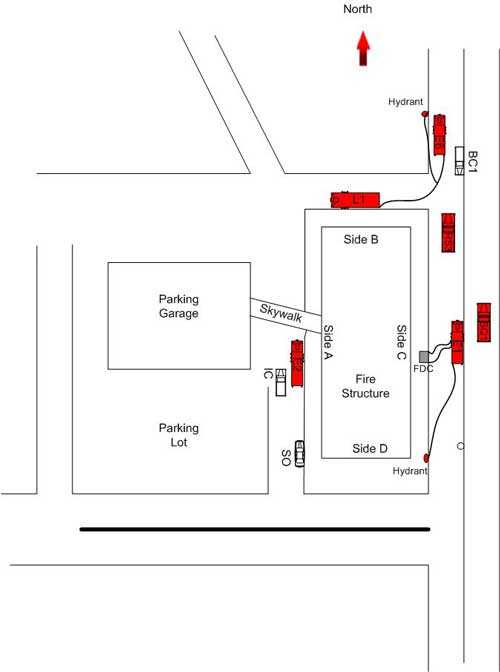 Diagram 1. Placement of 1st alarm apparatus.
Diagram 1. Placement of 1st alarm apparatus.
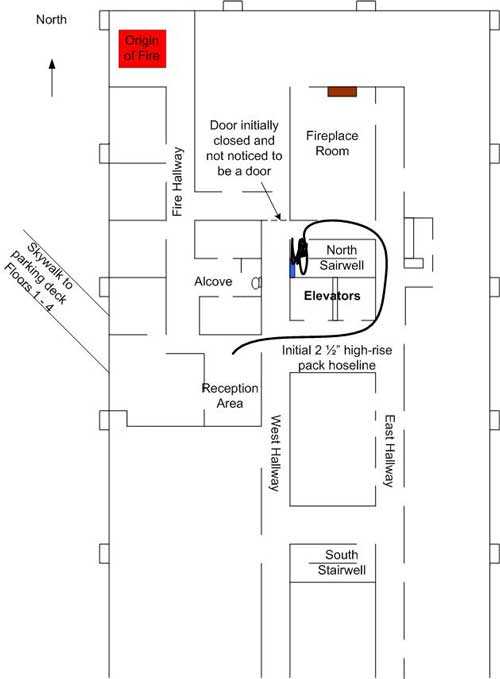 Diagram 2. Placement of initial hoseline at 5th floor standpipe. Hoseline on landing had numerous kinks in it.
Diagram 2. Placement of initial hoseline at 5th floor standpipe. Hoseline on landing had numerous kinks in it.
At 1255 hours, E2 requested that L1 attempt to get water on the fire at the A/B corner using the master stream. The IC and SO did not grant the request due to the interior crews on the 5th floor. At 1256 hours, crews located the fire room and E1 was connected to both standpipe systems (see Photo 2). E1 reported that there was still no water in the hoseline. At this time, command requests a third alarm. T1 had to reposition to deploy the ladder and was told that crews are on the fire floor so they were not to use the master stream. The R3 crew's low air alarms were going off so they headed to the north stairwell. At 1259 hours, the E2 crew was back on the fire floor after taking the elevator to the 5th floor. T1 broke a window on side B and E6 was preparing an 1¾-inch hoseline to bring up the ladder to hand through the window. The E2 crew picked up their original hoseline and moved it into the hallway but reported they were 30 feet short and needed another section of hose. E2 was feeling intense heat and thinking they were on side B took out a window on side A to cool down. At 1309 hours, E2 tried to get to the side B window to retrieve the hoseline from E6 on the ladder but could not get to it due to fire and heat. E6 made entry through the window as E2's low air alarms were going off again. They made their way to the elevators and were coming out as R3, E1, Q5, and E8 (dispatched on 3rd alarm) were headed to the north stairwell.
At 1311 hours, E6 got water on the fire for the first time. R3 was back on E2's original hoseline but reported to Command that there was no water and the IC ordered them out. E6 requested air bottles be brought to fire floor. At 1316 hours, E8 was on the fire floor, reported heavy smoke and heat and requested that the north stairwell be ventilated. Flames began venting out the side A windows that were broken. BC1 requested a ladder truck be positioned on side A for possible use in getting water on the fire venting from the windows. E6 requested additional hoseline to reach the fire venting on side A. The R3 crew, at the 5th floor north stairwell door, noticed the E8 captain and another fire fighter were untangling high-rise hoseline in the stairwell. One of the fire fighters from R3 was extremely low on air and the victim (R3 Captain) told the R3 engineer to take him down the stairs. The victim proceeded down the hallway instead of exiting down the stairwell. Another R3 fire fighter (with only a few years' experience) and an E1 fire fighter noticed the victim headed down the hallway so they followed after the victim. The victim and two fire fighters ended up in a small alcove with a bathroom at the end of it off the hallway to the fire room. All 3 fire fighters' SCBA low air alarms were going off. The two fire fighters grabbed the victim and headed back into the Side A hallway. The victim was following the R3 fire fighter but the E1 fire fighter got separated from them in the hallway due to the heavy smoke. The E1 fire fighter realized he was extremely low on air and thought about calling a Mayday. He took about ten steps and ran into the E6 fire fighter on the hoseline from T1. Shortly after, the E1 fire fighter followed the E6 hoseline to the window and got on the ladder just as he ran out of air (see Photo 3).
The victim told his partner they needed to buddy breath as he dropped to his knees. The fire fighter told the victim to call a Mayday which he did. Note: When the victim made his buddy breather connection, he did not control the release of air and all of the partner's air escaped through the victim's unclipped regulator. A minute or two later, the victim experienced an uncontrolled SCBA emergency and vomited in his facepiece and removed his mask. The victim told his partner to activate his PASS. The victim activated his PASS but inadvertently the R3 fire fighter turned his off. At 1320 hours, a Mayday was transmitted by the R3 fire fighter. The E6 captain had radioed Command and confirmed it was not the E1 fire fighter who had called the Mayday. The R3 fire fighter crawled to the elevators, decided not to use them, then crawled to a reception desk. Being out of air, he removed his mask, and called another Mayday, and dropped his portable radio in haste. He crawled down the Side C hallway toward Side D. Trying numerous doors as he went along, he came across the door to the south stairwell. He placed his axe tool in the doorway and then crawled back down the hallway to the victim. The R3 fire fighter removed his helmet, gloves, and hood and drug the victim on his back by his SCBA straps to the south hallway. The fire fighter pulled on and rolled with the victim down the stairs until they ended up at the landing between the 3rd and 2nd floor. At 1341 hours, the E8 captain exited the north stairwell and located the victim and R3 fire fighter in the south stairwell when he heard the victim's PASS alarm sounding. The E8 captain tried to give the victim air from his facepiece. Note: The victim's PASS alarm likely saved the life of his partner who had fallen down the south stairwell with the victim and lost consciousness. The officer who heard the PASS alarm was down a hallway and had just exited the north stairwell. The PASS alarm was heard through the fire door of the south stairwell. Two members from SQ1 and a member from E2 and R3 assisted in moving the victim as they all made their way to the 2nd floor elevator and took it to the ground floor. Medic units transported the victim and R3 fire fighter to the hospital where the victim was pronounced dead and the fire fighter was treated.


Photo 2. Fire room at A/B corner of structure.
View from the end of Side A hallway.
(NIOSH photo)
Photo 3. Interior studs of east wall of the fire room that the E1 fire fighter went through to get to the T1 platform at the window.
(NIOSH photo)
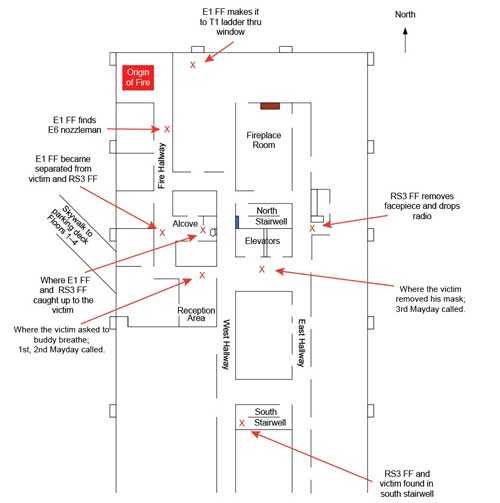
Diagram 3. Critical movement of the E1 fire fighter, RS3 fire fighter, and the victim.
Cause and Origin
Per the ATF report, the origin of the fire was in a records office on the 5th floor (6th story) at the A/B corner. The cause of the fire was arson via a flammable liquid.4
Contributing Factors
Occupational injuries and fatalities are often the result of one or more contributing factors or key events in a larger sequence of events that ultimately result in the injury or fatality. NIOSH investigators identified the following items as key contributing factors in this incident that ultimately led to the fatality:
- Arson
- Lack of an automatic fire suppression system
- Multistory/high-rise standard operating procedures not followed
- Air management doctrine not followed
- Inadequate strategy and tactics
- Task saturation of the incident commander
Cause of Death
The medical examiner's report states that the victim's cause of death was smoke and fume inhalation in an oxygen-depleted environment. Postmortem toxicological testing revealed a carboxyhemoglobin saturation of 22%.
Recommendations
Recommendation #1: Fire departments should ensure that the existing standard operating procedures for high-rise fire-fighting operations are reviewed, implemented, and enforced.
Discussion: The difference between a successful emergency operation that is brought to an early conclusion and one that becomes a prolonged effort, often heavily taxing a department's resources, depends greatly on actions taken by first-arriving companies. Experience has shown that initial actions at a high-rise emergency must fall into a priority order if the operation is to progress smoothly to a successful conclusion. A high-rise fire takes a considerable commitment of staffing and resources and differs greatly from a residential or other commercial structure fires. Most importantly, the incident management system structure must be developed from the bottom up, initiated by the first-arriving officer. 5
Standard operating procedures (SOPs) play an integral role in establishing order and consistency in operations at any emergency scene. They are especially important in high-rise incidents because of the inherent complexities of fighting a high-rise fire. SOPs should be written to achieve these purposes:
- Establish a high-rise strategic and tactical organization that fits the needs of the department and most importantly the needs of the incident.
- Establish levels of response (i.e., number of units assigned on each alarm).
- Establish roles and responsibilities of arriving companies by alarm (e.g., first alarm – fire attack, staging, lobby control, and base to assure overall management and resource accountability prior to the second alarm) and the company officers.
- Establish a system of fire-fighting operations familiar to all members of the organization.5
In this incident, the department did not follow these guidelines from their existing SOPs. Command did request a second alarm, which was never dispatched by the communications center and went unnoticed for more than 20 minutes. The department's standard operating procedure (SOP) requires a third alarm be struck upon the confirmation of a "working fire" in a high-rise. Also, lobby control was never established and stairwell support for evacuation and fire-fighting operations was never established. The north stairwell became charged with smoke due to the door on the fifth floor being propped open by an uncharged hose, which contaminated the stairwell down to at least the first floor if not the ground floor. Additionally, fire fighters from one of the first-alarm companies used the elevator three times to go directly to the fire floor rather than two floors below the fire floor or walk up the stairs. Windows were taken out on the fire floor, which helped with ventilation on the fire floor only.
Additionally, an SOP provides the framework of a fire department's response to a high-rise incident plus the special challenges that are presented and the strategies and tactics that must be employed to perform safely and effectively in a high-rise environment. An SOP establishes a degree of order to an emergency scene, which by nature is usually chaotic and very hectic. Basic topics to cover in a high-rise SOP are listed below, which is not an all-inclusive list:
- Level of response (i.e., number and type of apparatus dispatched)
- Deployment of resources upon arrival (1st, 2nd, 3rd, 4th due (fire attack, staging, lobby control , and base need to be established))
- Establishment and structure of the incident management system (develop an SOP for the deployment of Chief Officers upon arrival)
- Personnel accountability system
- Fire fighter safety
- Lobby control
- Use of elevators and stairwells
- Evacuation and rescue
- Water supply
- Supplementing and supporting fire protection systems
- Proper hose and nozzles for interior operations
- Ventilation
- Contingency plans for failure of fire protection systems6, 7
The fire department involved in this incident had developed an SOG in February 2004 for a response to a high-rise fire. The guideline had been reviewed by their SOG Committee in February 2011. The guideline defined a "high-rise" occupancy as any structure over three stories or a structure that has a standpipe system. The department's SOG discussed the following responsibilities:
- Command
- Deployment of resources–first-alarm assignment (called Operations in the SOG);
- Lobby Control
- Enclosed stairwells/towers
- Elevators
- Ventilation
- High-rise kits
Recommendation #2: Fire departments should ensure that a deployment strategy for low-frequency/high-risk incidents is developed and implemented.
Discussion: Since no two fire departments are alike, there is no standard scale to measure and evaluate frequency and severity of risk. Some fire departments will have a greater or lesser degree of tolerance for risk than others. The intent of the risk management process is for a fire department to develop a standard level of safety. This standard level of safety defines the parameters of the acceptable degree of risk for which members perform their job functions.8
When commanding and controlling a high-rise fire, fire officers may resort to what they did at a similar incident, or what they've seen and heard most frequently. These individuals use memory recall to try and find a match in terms of training, experience, and competencies for developing effective strategy and tactics. If there is nothing to draw from, the individuals will resort to actions that they are familiar with or comfortable with relating the incident.9 The process is methodical and must start from the beginning of the incident with the arrival of the first-alarm companies. If steps are skipped or missed, it becomes very difficult to change the outcome as the incident progresses. There is very little room for deviation at a high-rise fire on the tactical and task level. The tactics for fire-fighting operations at a high-rise fire has to occur based upon departmental procedures or guidelines. During this incident, the fire department did not develop an incident action plan to lay out the strategy and tactics for the fire.
By definition, frequency is how often something does, or might happen. Severity (risk) is a measure of the consequences if an undesirable event occurs. Each risk will have its own set of factors that will dictate how the fire department determines the severity of the consequences. Priority of the risk is in direct relation to inherent risks that have had a harmful effect on the fire department and its members.10
High-rise fires are low-frequency/high-risk events from the standpoint that they do not occur on a regular basis, but when they do occur the risks are significant. A fire department must have a deployment strategy in place to effectively manage a high-rise fire. This deployment strategy must address the staffing, incident management, appropriate strategy and tactics, use of fixed fire protection, adequate water supply, and other resource/logistical management issues. In order to effectively contain and extinguish a fire in a high-rise structure, a fire department must also have in place a standard operating procedure for high-rise fire-fighting operations that addresses training for high-rise operations due to the complexity of these incidents, knowledge of fire protection systems, a pre-incident planning process for high-rise structures, proper high-rise hose and nozzle configurations, compartmentalization of the fire, and evacuation of occupants.6
Because high rise fires are low frequency events, it has proven beneficial that an agency's high rise procedures be utilized at all high rise alarms. When a fire department responds to high rise building alarms it enables on-scene Department personnel the ability to exercise the agency's high rise procedures. Therefore, the fire attack company becomes familiar with the access to upper floors by checking two floors below the reported fire floor for floor layout familiarization, establish staging and communicating this to the IC. The assignment of a company to Lobby Control allows this company to become familiar with the building systems (annunciator, elevator system and elevator recall, and fire control room if provided), location of stairwell access for companies and stairwell pressurization. The apparatus drivers become familiar with the FDCs.
In this incident, the use of the elevator by E2 in a six story high rise could have added to the seriousness of this incident especially by not putting the elevators in "fireman mode" and taking the elevator three times to the fire floor. Historical incidents have occurred where firefighters have died by taking the elevator to the fire floor where the fire ended up being in proximity to the elevator shaft. This is an example of the need for periodic or refresher high rise training identifying safety concerns regarding the use of elevators.
This building did not have complete sprinklers and the elevator doors were not protected by a vestibule. In a six story building, the advantage of taking the stairwell from the ground floor reduces the risk for responders going above a known working fire, allows the fire attack company the ability to check two floors below the fire floor for Staging, and allows the fire attack company the ability to quickly see a typical floor layout.
Procedures for fire attack have shown connecting the first hose line to the standpipe outlet on the floor below the fire floor allows the hose lines to be flaked out in the stairwell before charging with water prior to opening the stairwell door on the fire floor. This is especially important if the fire turns out to be adjacent to the access door in the stairwell and if the firefighters have to fight their way into the floor. It also allows fire fighters the ability to extend the hose line on the floor below instead of doing it in front of the door used for access to the fire floor. Departments should develop a deployment plan for sequentially arriving chief officers and should consider assigning the second chief officer to whatever floor is involved in a high rise incident.
Often 2 ½-inch high rise hose packs are carried and utilized by fire departments. These departments should evaluate the use of an additional smaller light weight hose on high rise hose packs (2-inch light weight hose with 1½-inch couplings and 1½-inch nozzles) that provides 200 gallon per minute (gpm) in comparison to the 2 ½-inch hose lines and nozzles that produces 250-325 gpm. At high rise fires in Los Angeles, these lighter weight hose lines have proven to be beneficial because they are more mobile when stretching a line from the stairwell into the fire floor, easier to remove kinks, and can be extended easier with less staffing. Also, the fire department may want to evaluate the use of a 2 ½-inch hose pigtail approximately six foot in length with a pre-connected 2 ½-inch X 1 ½-inch gated wye that allows for the connection of two hose lines and the movement of hose lines within the stairwell. The option to use 2 ½-inch hose lines can still be used based upon the size and magnitude of the fire.
Below is an example model of a first-alarm response to a reported high-rise fire. The resources deployed are four engine companies, two truck companies, one heavy-rescue company, and one battalion chief. Every fire department having high-rise buildings in their response area should develop a deployment model for a high-rise response. The model can be modified to meet a department's deployment strategy for a high-rise response.
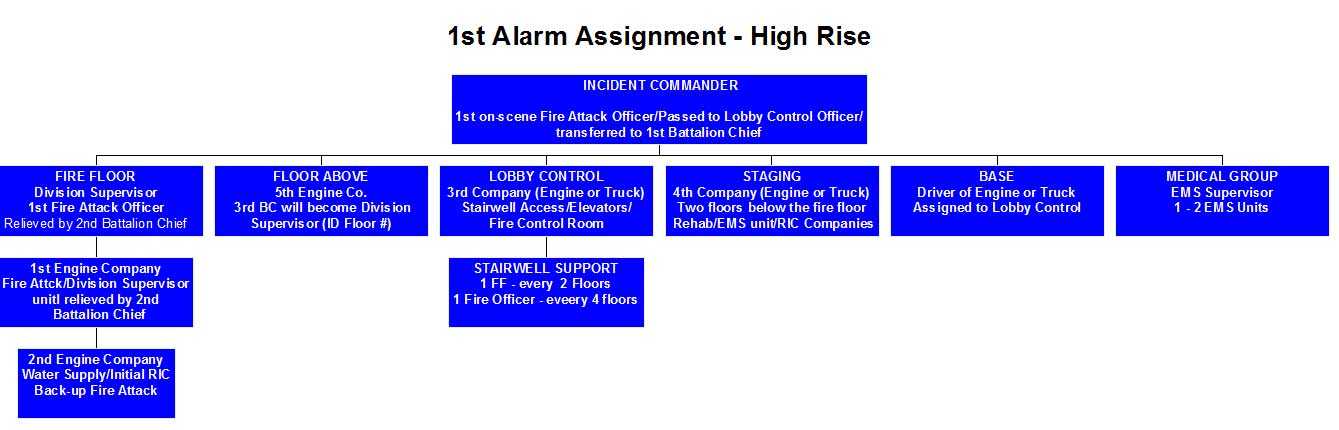
It is important for responders assigned to truck companies to understand that they may be used to perform fire attack, relief of engine companies, or other functions at high rise incidents. The first alarm must establish fire attack, staging, lobby control, and base to assure a system is in place for the overall management and resource accountability at a high rise incident.6, 7
Recommendation #3: Fire departments should ensure that the incident commander develops an incident action plan, which is communicated to all fire fighters on scene and includes effective strategy and tactics for high-rise operations, a timely coordinated fire attack, and a coordinated search plan.
Discussion: When establishing "Command" at any incident, one of the most important responsibilities of the incident commander is to create an appropriate incident action plan. This is especially important at high-rise incidents due to the fact that these incidents are low-frequency/high-risk events. Based upon the initial size-up, the incident commander has to absorb and process a lot of information in a very short period of time and develop an initial incident action plan that is based upon the department's standard operating procedures/guidelines, encompassing effective strategy and tactics, and incorporates the incident priorities (life safety, incident stabilization, and property conservation).8-10
A high-rise fire is completely different from a residential or other commercial structure fire in terms of strategy in that seldom is there an option of going defensive. The incident commander must have the ability to deploy a lot of fire fighters in a short period of time to effectively command and control these types of incidents. The tactics must not only include the standard tactical assignments such as search, rescue, fire attack, and ventilation, but must include the ability to get resources to the fire floor in a short period of time and in a "ready to work" mode. These considerations must include adequate staffing, water supply, supporting fire protection systems (sprinkler systems and standpipe systems), and various incident command system roles and responsibilities such as lobby control, establishing and supporting base operations, stairwell support, system control, and ground support.5
Each department needs to develop an SOP on how to assign resources to a high rise incident to cover fire attack, back-up fire attack, lobby control and base, staging, and covering the floor above the fire floor. Department staffing and the number of companies needed should be considered in developing SOPs to locate the fire; relocate or evacuate occupants; access, identify, and gain control of the building systems; confine and extinguish the fire; considerations for connecting to the FDC, especially if the building has a dry standpipe system; positive pressure of the stairwells; movement of equipment from Base/Lobby to Staging; and any other incident needs.
Regarding the development of the initial strategy at a high-rise incident, the incident commander has to determine the scope of the problem:
- Where is the emergency located, where is it going?
- Is there an immediate life hazard?
- Is there a need to control evacuation?
- Does the building inventory plan or private building plan (e.g., Massey Plans) indicate any unusual features that will assist or complicate operational or logistical planning?
- Will a medical group be required?
- Will an elevator group be required?
- Will a search group be required?
One of the most critical factors for high-rise fire-fighting operations is the lead time necessary to get personnel and equipment in position at their assignments. This is the single greatest difference between controlling an incident in a high-rise structure as opposed to an incident at ground level. The incident commander must keep this in mind. 6
A coordinated fire attack is another essential element that must occur as quickly as possible. Consideration must be given to the time it takes to get adequate resources to the fire floor and to apply water to the fire. The first company on the scene, by the use of a safe route, shall proceed to the area where the emergency exists, assess the scope of the emergency, communicate this information to the incident commander, and take measures to mitigate the emergency. Once the first-in company officer commits to a tactical objective (i.e., fire attack) and other resources arrive on scene, command of the incident should be "passed" to another on-scene officer or transitioned to a higher-ranking officer. No matter what the scenario, the first-in engine company conducting offensive operations must get the proper size and length of hoseline to the fire without delay. Fire fighters from the engine company can prepare the proper high-rise hose for standpipe operations. After confirming the size and length of the line to be stretched with the company officer and verifying the route into the building, the engine company can begin the attack. A proper stretch to the seat of the fire is key to efficient suppression. Not only must the optimal route be used, but the line must also be of sufficient flow rate (gallons per minute) and length to work the fire area and immediate interior exposures. Fire fighters must then operate effectively to control fire and heat conditions. This action will allow safe and rapid searches by the truck companies and will give any trapped victims their best chance at survival.11
Any successful fire suppression operation includes a concurrent search component to ensure the accountability and safety of building occupants. The establishment of a search group ensures that a primary and secondary search for building occupants is conducted and completed. Simultaneous to fire suppression efforts, primary searches should be initiated, and a systematic approach to searching all areas compromised by smoke should be immediately addressed. The search group should work in concert with the evacuation group (if or when established).
The search group supervisor works closely with the evacuation group supervisor and manages all building occupants located above the ground floor of the involved building. Searches need to be conducted on a priority basis, beginning with the fire floor and all areas above the fire. Search efforts can be extremely labor and personnel intensive due to the area required to be covered. Even though the incident might dictate the relocation of occupants from the immediate area surrounding the fire floor to safe refuge areas, all areas above the fire floor and subsequently all areas of the building need to be searched. This includes all hallways and stairways. Attention should be given to continually monitoring stairwells, particularly the fire attack stairwell above the fire floor. Conditions in the evacuation stairwell should also be continuously monitored. The stairwell door to the fire floor should not be opened into the evacuation stairwell. The only exception is when it necessitates a civilian and/or fire-fighter rescue. 6
Another key factor is ventilation. When properly setup and correctly operated, positive pressure ventilation is a tool which the fire service can use to improve the safety and effectiveness of fire ground operations. Positive pressure ventilation fans utilized correctly can increase the effectiveness of fire fighters and survivability of occupants in high-rise buildings. In a high-rise building it is possible to increase the pressure of a stairwell to prevent the infiltration of smoke if fire crews configure the fans properly. When configured properly, PPV fans can meet or exceed previously established performance metrics for fixed smoke control systems. Proper configuration requires the user to consider a range of variables including, fan size, set back and angle, fan position inside or outside of the building, and number and alignment of multiple fans. The data collected during a limited set of full-scale experiments in a 30-story office building demonstrated that in order to maximize the capability of PPV fans the following guidelines should be followed:
- Regardless of size, portable PPV fans should be placed 1.2 m (4 ft) to 1.8 m (6ft) set back from the doorway and angled back at least 5 degrees. This aximizes the flow through the fan shroud and air entrainment around the fan shroud as it reaches the doorway.
- Placing fans in a V-shape is more effective than placing them in series.
- When attempting to pressurize a tall stairwell, portable fans at the base of the stairwell or at a ground floor entrance alone will not be effective.
- Placing portable fans inside the building below the fire floor is a way to generate pressure differentials that exceed the NFPA 92A minimum requirements. For example, if the fire is on the 20th floor, placing at least one fan at the base of the stairwell and at least one
near the 18th floor blowing air into the stairwell could meet the NFPA 92A12 minimum requirements. - Placing a large trailer-mounted type fan at the base of the stairwell is another means of generating pressure differentials that exceed the NFPA 92A minimum requirements.
- Fans used inside the building should be set back and angled just as if it were positioned at an outside doorway.13
In this incident, the incident commander had personnel with hoseline on the fire floor and conducting a search of the fire floor. However, an effective fire attack never occurred due to issues with air management and getting water from the standpipe system, which caused a multitude of issues. Also, the fire floor was searched multiple times, but with no consistency or plan. Building maintenance personnel assisted with the evacuation of occupants on the floors below the fire floor. The floors below the fire floor were not searched by the fire department until after the fire was controlled. When issues develop that impact or alter the incident action plan, this information must be communicated to Command. These issues have to be resolved or overcome in order to successfully control the incident.
Recommendation #4: Fire departments should ensure that the incident commander utilizes division/group supervisors for effective tactical level management.
Discussion: For any incident involving a high-rise building, the need for effective span of control and the effective use of staffing and resources requires effective tactical level management.8 In this case, the incident commander could have used divisions and/or groups to manage the available resources committed to this incident.
A Division is the organizational level having responsibility for operations within a defined geographic area. A Group is an organizational level responsible for a specified functional assignment at an incident. The use of Divisions/Groups in the ICS organization provides a standard system to divide the incident scene into smaller subordinate management units or areas. Complex emergency situations often exceed the capability of one officer to effectively manage the entire operation. Divisions/Groups reduce the span-of-control to more manageable smaller-sized units. Divisions/Groups allow the incident commander to communicate principally with these organizational levels, rather than multiple, individual company officers providing for command and incident scene organization.14
A span of control of three to seven resources with five being the optimum is considered desirable in most cases. To maintain an effective span of control at each level of the command structure, the organization should be expanded whenever the need is identified. This can be accomplished by adding levels or reassigning responsibilities within existing levels or a combination of both. The incident commander also should consider activating additional levels within the command structure where activities become highly complex or are conducted over a large geographical area. In this incident, the incident commander could have assigned an operations section chief to oversee fire-fighting operations.
Generally, Division/Group responsibilities should be assigned early in the incident, typically to the first company assigned to a geographic area or function. This early establishment of Division/Group provides an effective incident management organization framework on which the operation can be built and expanded. The number of Divisions/Groups that can be effectively managed by the incident commander varies. Normal span-of-control is three to seven. In fast moving, complex operations, a span of control of no more than five Divisions/Groups is indicated. In slower moving less complex operations, the incident commander may effectively manage more Divisions/Groups. Division/Group guidelines provide an array of major functions which may be selectively implemented according to the needs of a particular situation. This places responsibility for the details and execution of each particular function on a Division/Group. When effective Divisions/Groups have been established, the incident commander can concentrate on overall strategy and resource assignment, allowing the Division/Group Supervisor to supervise their assigned units. The incident commander determines strategy and assigns tactical objectives and resources to the Divisions/Groups.14
Each Division/Group Supervisor is responsible for the tactical deployment of the resources at their disposal, in order to complete the tactical objectives assigned by the incident commander. Division/Group Supervisors are also responsible for communicating needs and progress to the incident commander. Divisions/Groups reduce the overall amount of radio communications. Most routine communications within a Division/Group should be conducted in a face-to-face manner between company officers and their Division/Group supervisor. This process reduces unnecessary radio traffic and increases the ability to transmit critical radio communications. The safety of fire-fighting personnel represents the major reason for establishing Divisions/Groups. Each Division/Group supervisor must maintain communication with assigned companies to control both their position and function. The Division/Group supervisor must constantly monitor all hazardous situations and risks and communicate these situations to personnel. The Division/Group supervisor must take appropriate action to ensure that companies are operating in a safe and effective manner.6
For high rise incidents, the numerical numbering within a high rise building would be used as the Division Supervisor identifier on the assigned floor. For example, the Officer assigned in charge of the 5th floor would be Division 5 Supervisor. This Division Supervisor is responsible for coordinating fire attack and to maintain resource accountability for the geographic area of the floor. Functional assignments that may cover more than one floor such as Ventilation would be identified as the Ventilation Group Supervisor. The first company on scene is normally fire attack and the officer serves as the IC until passed to another on-scene company officer or transferred to a higher ranking officer, and upon arrival at the fire floor the fire attack officer becomes the floor Division Supervisor until relieved.6
Recommendation #5: Fire departments should ensure that the incident commander designates a staging area at least two floors below the fire floor.
Discussion: The challenging nature of high-rise incidents requires modification to the standard incident command system (ICS) concept of a staging area. The limited access and vertical travel distance of large high-rise buildings require establishment of a resource staging area within the building. The high-rise staging area must also serve multiple functions, including stockpiling equipment, reserve personnel, rehab, and medical treatment. The staging area is generally located a minimum of two floors below the emergency, as long as the atmosphere is tenable.6
The staging area manager verifies the location of the staging area with the incident commander, including a plan layout of the area and its ability to manage all staging activities. The staging area must have the following:
- Separate areas for control of reserve and rehab personnel.
- Separate areas to stockpile reserve and expended equipment.
- Area for a medical treatment station/rehabilitation for incident personnel.
- Space to maintain complete, accurate record of resource status to assure accountability.
- When available, a building sound-powered/emergency/direct communication phone.15
The staging area manager is subordinate to the incident commander/operations chief. The staging area manager will be located in or adjacent to the staging area to facilitate effective control of its activities. Resources should arrive at the staging area via a common route. Staging personnel should be positioned to meet, check in, and direct personnel to the appropriate area. All stairwell access to staging must be controlled to prevent companies from bypassing the staging area.15
Some tactical considerations for the staging area manager include:
- Consult with the incident commander/operations section chief to determine minimum staffing reserve.
- Order additional resources through the incident commander/operations section chief as resources are dispatched from the staging area.
- Use, when feasible, an alternative communication system—e.g., a separate tactical channel, building telephone system, messengers—to access logistics.
An effective communications link must be maintained with the incident commander/operations section chief. 6
The staging area manager must develop an equipment inventory and be able to order specific quantities from base, so the following should be considered:
- Air bottles
- Air hose with fittings
- SCBA
- Smoke ejectors
- Forcible entry tools
- Salvage equipment
- Pike poles
- Ladders
- Medical supplies/resuscitator
- Drinking water or fluids for rehab of fire fighters
- Spare radio batteries6
Additional companies directed to Staging should bring priority equipment from the Base/Lobby. Spare SCBA air cylinders are always a first priority. An agency should provide guidance for utilizing a sling to connect two SCBA bottles together so fire fighters can carry extra SCBA air cylinders in one hand or over one shoulder when leaving Base to go to Staging. The staging area manager must maintain a record of equipment ordered, time ordered, and time delivered. This equipment or any equipment ordered must be separated and stored so it is readily accessible. The storage areas can be identified by taping signs to the walls.6
At this incident, no interior staging area was established. When companies ran out of breathing air or were fatigued, they had to walk from the 5th floor to the ground floor (five flights of stairs). Once they had completed "Rehab" and were assigned back to the fire floor, they had to walk up five flights of stairs while "on air." With 1200-liter (30-minute) cylinders, this left about 5–7 minutes of work time before the low-air alarm activated.
Recommendation #6: Fire departments should ensure that fire fighters are properly trained in air management.
Discussion: Chief Bobby Halton, retired chief and Editor in Chief of Fire Engineering notes, "If you run out of air in a working fire today, you are in mortal danger. There is no good air at the floor anymore, no effective filtering methods, no matter what others may say to the contrary."16 The only protection for fire fighters in the toxic smoke environments in today's fires is the air that they carry on their backs. Like SCUBA divers, fire fighters must manage their air effectively and leave enough reserve air to escape in case of unforeseen occurrences while inside a structure fire. Fire fighters must manage their air so that they leave the immediately dangerous to life or health (IDLH) atmosphere before the low-air alarm activates. This leaves an adequate emergency reserve [air] and removes the noise of the low-air alarm from the fireground.16 Air management is a program that the fire service can use to ensure that fire fighters have enough breathing air to complete their primary mission and to escape an unforeseen emergency. Fire departments and fire fighters need to recognize that the smoke in modern construction is an IDLH atmosphere and manage their air along with their work periods so the fire fighters exit the IDLH with their reserve air intact. NFPA 1404 Standard for Fire Service Respiratory Protection Training states that fire fighters should exit from an IDLH atmosphere before the consumption of reserve air supply begins; a low-air alarm is notification that the individual is consuming the reserve air supply and that the activation of the reserve air alarm is an immediate action item for the individual and the [fire-fighting] team.17
In this incident, the fire fighters (including the victim and his partner) had to ascend the high-rise medical office building to the 5th floor (five flights up) via an interior stairwell that was full of smoke. The fire fighters had to ascend the stairwell (on air from their SCBA) while carrying all of their equipment up the stairs. Once the crews got to the fire floor, the air in their 1200-liter (30-minute) cylinders was already depleted and was not sufficient for fire-fighting and search efforts. Note: "Firefighters' personal experience has demonstrated that the 1200L cylinder [30-minute] will not provide a working firefighter with 30 minutes of air. The 1200L cylinder will last an average firefighter actively engaged in suppression activities about 15–18 minutes.16 Many fire fighters reported during interviews with NIOSH investigators that their end-of-service-time indicators (EOSTI) sounded on the fire floor. There were heavy fire and smoke conditions on the fire floor and heavy smoke conditions in the stairwell used by fire fighters. In order to exit the IDLH atmosphere, fire fighters had to exit the fire floor and then climb down five flights of stairs to the ground level. There was no staging area set up on the lower floors that would have provided an area of non-IDLH refuge where the fire fighters could have rehabbed and replenished their air supply. Another option in a high-rise building would be to increase the pressure of a stairwell to prevent the infiltration of smoke if fire crews configure PPV fans properly which could provide a non-IDLH refuge.
Note: The fire stairwell in the building had a significant volume of smoke from the 5th floor down to the lobby level due to entrainment from a phenomenon known as reverse stack effect. Reverse stack effect results from a temperature difference between warm outside and cooler inside air that creates a buoyancy driven downward flow of air (and smoke) from the top to the bottom of a tall building. Firefighters described the smoke in the stairwells as being very dense, stating that they were forced to breathe supplied air prior to arriving at the fire floor. The victim ascended, descended and re-ascended the smoke filled stairs (reportedly only on air for the top 2 floors), as he reentered the fire building a second time after replenishing his initial air supply. Prior to exhausting his supplied air, firefighters report that the victim's behavior was somewhat atypical, with bouts of apparent confusion, disorientation and impaired psychomotor ability. The victim's cause of death was determined to be "smoke and fume inhalation in an oxygen depleted environment" with a carboxyhemoglobin (COHb) level of 22%. It is possible that the victim would exhibit only mild to moderate symptoms of the toxic effects of CO until 15-20% COHb was achieved. Confusion, disorientation and impaired psychomotor ability are documented symptoms for mild to moderate CO exposure, especially in active individuals.18 Accordingly, the victim could have experienced mild to moderate CO poisoning from his exposure to smoke in the stairwell, leading to his observed bouts of apparent confusion, disorientation and impaired psychomotor ability. These symptoms of CO exposure likely contributed to the events that resulted in the victim exhausting his air supply while attempting to locate the exit stairwell and removing his air regulator. In active individuals, unconsciousness can result with only a small increase in COHb levels. At this point, the victim's COHb levels were likely already elevated and the additional CO exposure on the fire floor compounded with the initial CO exposure in the stairwell may have contributed to his rapid loss of consciousness as compared to his firefighting partner.19
Recommendation #7: Fire departments should ensure that fire fighters are properly trained in out-of-air SCBA emergencies and SCBA repetitive skills training (e.g., buddy breathing and clearing a facepiece).
Repetitive skills training with SCBA is vital for fire fighters working inside an IDLH atmosphere. SCBA skills training is an ongoing process that should be performed regularly to ensure that fire fighters "know their SCBA." The benefits of repetitive skill training with SCBA are an increased comfort and competency level, decreased anxiety, lower air consumption, increased awareness of the user's air level (noticing and using the heads-up display (HUD), and an automatic muscle memory response of the vital function controls, such as the don/doff buttons, main air valve, emergency bypass operating valve, and auxiliary air connections (i.e., rapid intervention crew/universal air connection (RIC/UAC) connection and the buddy breather connection). Repetitive skills training can also provide the user with an increased ability to operate these functions and controls in a high-anxiety moment or an emergency. Many times these skills will be necessary with gloved hands, limited vision, and reduced ability to hear commands from others. Performed in conditions that are non-IDLH, repetitive skills training helps build the fire fighters' muscle memory skills so their hands will be able to activate the controls with gloves on and the operation will be a conditioned or second-nature response. Fire fighters have died in IDLH conditions because they did not react properly to an out-of-air emergency, such as vomiting in a facepiece.20
The victim in this incident likely vomited in his SCBA facepiece while he still had the facepiece on. The victim's partner noticed the victim had the mask off his face when the victim told him that he needed to hook up the buddy-breathing connection. When the partner plugged in his connection to the victim's connection, all of the air in the partner's SCBA escaped out of the victim's SCBA. It is likely that the victim did not activate his doff button because he had ran out of air. This would have left his second-stage regulator in the flow position, and when the partner connected his buddy breather to the victim's connection, the line was open, allowing the partner's air to escape. Fire fighters need to be trained to properly use their equipment, and the repetitive skills training reinforces the muscle memory to properly activate the correct controls. Overcoming out-of-air emergencies is an important goal of repetitive skills training.
Fire fighters should never remove their facepiece in an IDLH atmosphere. Self-contained breathing apparatus have undergone many changes over the past decades, one of which is the incorporation of a nose cup. The nose cup helps eliminate fogging/condensation of the facepiece lens and reduces the percentage of exhaled CO2 in the facepiece. However, it has a very limited area of free space if a fire fighter gets sick and the potential to clog the exhalation valve is high. It is important that fire fighters know how to operate the emergency bypass valve to remove any obstructions, such as vomitus, assuming there is sufficient air in the cylinder. Depending on the manufacturer, nose cups can be removed rather quickly and the facepiece may remain fully functional, providing breathable air, without it. Currently, a validated best practice for an emergency training protocol could not be found for this particular model SCBA. An emergency training protocol should be established for the removal or clearing of the nose cup in an emergency situation for each type of SCBA. The International Association of Fire Fighters (IAFF) and other fire-fighting agencies are currently working to develop a standardized protocol to educate and train fire fighters on how to deal with debris-clogged facepieces.
Note: The practice of "buddy breathing" is the subject of much discussion in the fire service. OSHA 29 CFR 1910.156(f)(1)(iii) states, "Approved self-contained breathing apparatus may be equipped with either a buddy breathing device or a quick disconnect valve, even if these devices are not certified by NIOSH. If these accessories are used, they shall not cause damage to the apparatus or restrict the air flow of the apparatus, or obstruct the normal operations of the apparatus."
Note: NFPA 1404 Standard for Fire Service Respiratory Protection Training states, "until and unless NIOSH approves an auxiliary device for buddy breathing, the practice of buddy breathing is not endorsed in any way by the Technical Committee on Fire Service Training".17 In 2011, NIOSH NPPTL sought comments on a proposed change in the interpretation of the prohibition of "buddy breather connections" on SCBA. The NFPA technical committee on respiratory protective equipment21 appointed a task group to develop performance requirements for an Emergency Buddy Breathing Safety System (EBBSS). The committee is currently revising the language in the proposed document to include performance criteria for an EBBSS connection.
Recommendation #8: Fire departments should ensure that the incident commander is provided a chief's aide to assist in incident management, including communications and personnel accountability.
Discussion: A chief's aide, staff assistant, or field incident technician (FIT) is a position designed to assist an IC with various operational duties during emergency incidents. The chief's aide is an essential element for effective incident management and for a successful outcome of the incident. The importance of having a chief's aide assigned to a battalion chief is to insure that the tasks associated with incident management can be initiated even before arrival on scene. The benefit of having a chief's aide is that the battalion chief can focus on radio communications, initiate the development of the strategy and tactics for the incident, and began to develop an incident action plan. The battalion chief is able to focus on the critical incident management tasks versus trying to operate the vehicle and locate the incident scene under emergency response conditions. If a chief's aide is not provided for a battalion chief, the tasks are delayed until a fire fighter or fire officer is appointed to this position. At an emergency incident, the staff assistant can assist with key functions, such as managing the tactical worksheet; maintaining personnel accountability of all members operating at the incident (resource status and situation status); monitoring radio communications on the dispatch, command, and fireground channels; control information flow by computer, fax, or telephone; and access reference material and pre-incident plans.
The personnel accountability system is a vital component of the fire fighter safety process. The system is designed to account and track personnel as they perform their fireground tasks. In the event of an emergency or "Mayday," the personnel accountability system must be able to provide the rapid accounting of all responders at the incident. This is one of the chief's aide's essential responsibilities. Another important chief's aide function is the role of a driver in addition to their role as part of the command team. Chief officers are required to respond quickly to emergency incidents. In their response, they have to be fully aware of heavy traffic conditions, construction detours, traffic signals, and other conditions. More importantly, the chief officer must also monitor and comprehend radio traffic to assess which companies are responding, develop a strategy for the incident based upon input from first-arriving officers, and develop and communicate an incident action plan that defines the strategy of the incident. A chief's aide can assist the battalion chief or chief officer in processing information without distraction and complete the necessary tasks en route to the scene.22
Departments should consider the aide to be an individual who has the experience and authority to conduct the required tasks. Other potential functions for the chief's aide include serving as group or division supervisors, training position to facilitate officer development, and non-emergency functions that are vital to the daily operations of the department (e.g., daily staffing and leave management).
Recommendation #9: Fire departments should ensure that the incident commander establishes a stationary command post for effective incident management, which includes the use of a tactical worksheet, enhanced fireground communications, and a personnel accountability system.
Discussion: When a chief officer (e.g., battalion chief, district chief, deputy chief) arrives on scene, he/she should automatically assume a standard stationary, exterior, and remote command position and immediately assume "Command" and begin functioning as the incident commander. Command officers generally establish and continue command and control functions inside their vehicles or at the rear of the vehicle, which has a command board.
According to NFPA 1561 Standard on Emergency Services Incident Management System, §5.3.1 states, "The incident commander shall have overall authority for management of the incident." In addition to conducting an initial size-up, the incident commander must establish and maintain a command post outside of the structure to assign companies and delegate functions, and continually evaluate the risk versus gain of continued fire-fighting efforts. 22 Also, NFPA 1561 requires all members working in an IDLH atmospheres to work in pairs. Any supervisor given an assignment in a potential IDLH atmosphere needs to have an aide or assistant to provide safety and accountability. This is very important at a high rise incident. 23
In establishing a command post, the incident commander shall ensure the following (NFPA 1561, §5.3.7.2):
- The command post is located in or tied to a vehicle to establish presence and visibility.
- The command post includes radio capability to monitor and communicate with assigned tactical, command, and designated emergency traffic channels for that incident.
- The location of the command post is communicated to the communications center.
- The incident commander, or his/her designee, is present at the command post.
- The command post should be located in the incident cold zone.23
The tactical worksheet is a critical piece of equipment because it helps the incident commander organize these and other tasks by providing reminders, prompts, and a convenient workspace for tracking companies and apparatus. It allows them to slow down during what could be a large, multi-alarm incident (although the worksheet can be used for fires big and small, as well as EMS incidents, to help develop proficiency) and record vital information that may help them make future operational decisions. By documenting the assignments of division/group officers, and division/group resources, the incident commander creates a visual reference of the overall fireground organization and deployment. 23
The tactical worksheet is also an excellent tool when the "passing of command" must occur. On the fireground, the officer taking over command can quickly check the worksheet and obtain a strong understanding of the initial deployment of resources, the need for additional apparatus and equipment, and the status of units in the staging area.
A communication system should include a dispatch, command, and tactical channels, though for many organizations this may be only one or two channels. In some jurisdictions, several communities may share several radio channels for public safety operations or localities may share radio channels within its government agencies (e.g., fire, law enforcement, EMS, and public works). A fire department must ensure that the needed radio channels are available when a large-scale or complex incident occurs. This can include the use of a common radio frequency, which can be designated as a "mutual aid frequency" to ensure proper communications is available during a large-scale or complex incident such as a wildland urban interface fire, which requires resources from mutual aid fire departments as well as assisting agencies and cooperating agencies. Standard operating procedures, radio equipment and other hardware, the ability to record and capture all radio channel transmissions, and dispatch and communication protocols must be in place to ensure that available radio channels are available when needed. 23
The function of resource accountability should be assigned to personnel who are responsible for maintaining the location and status of all assigned resources at an incident. As the incident escalates, this function would be placed under the planning section. This is separate from the role of the incident commander. The incident commander is responsible for the overall command and control of the incident. Due to the importance of responder safety, this function should be assigned to dedicated accountability personnel as the size and complexity of the incident dictates. A number of positions could function in this role including a staff assistant(s), chief officer(s), or another responder(s)
There are many means of accounting for resources. Components can include tactical worksheets, command boards, apparatus riding lists, company responder boards, electronic bar-coding systems, and so forth. These components can be used in conjunction with one another to facilitate the tracking of responders by both location and function. The components of the personnel accountability system should be modular and expand with the size and complexity of the incident. 23
Recommendation #10: Fire departments should ensure that fire fighters are properly trained in Mayday standard operating guidelines and survival techniques.
Discussion: Fire fighters need to maintain situational awareness at all times while operating on the fireground. Fire fighters need to understand that their personal protective equipment (PPE) and self-contained breathing apparatus (SCBA) do not provide unlimited protection. Fire fighters should be trained to stay low when advancing into a fire as extreme temperature differences may occur between the ceiling and floor. When confronted with an emergency situation, the best action to take may be immediate egress from the building or to a place of safe refuge (e.g., behind a closed door in an uninvolved compartment, in a staging area on a lower floor) and manually activate the PASS device. A charged hoseline should always be available for a tactical withdrawal while continuing water application or as a lifeline to be followed to egress the building. Conditions can become untenable in a matter of seconds. Fire fighters must understand that when they are faced with a life-threatening emergency, there is a very narrow window of survivability, and any delay in egress and/or to transmit a Mayday message reduces the chance for a successful rescue. Knowledge and skill training on how to prevent a Mayday situation or how to call a Mayday should be mastered before a fire fighter engages in fireground activities or other immediately dangerous to life and health (IDLH) environments.24 Fire fighter training programs should include training on such topics as air management; familiarity with SCBA, a radio, and PPE; crew integrity; reading smoke, fire dynamics and behavior; entanglement hazards; building construction, and signs of pending structural collapse. If fire fighters find themselves in a questionable position (dangerous or not), they must be able to recognize this and be trained on procedures for when and how a Mayday should be called. A fire fighter's knowledge, skill, and ability to declare a Mayday must be at the mastery level of performance. This performance level should be maintained throughout their career through training offered more frequently then annually.25
The ability of a fire fighter to call a Mayday is a complicated behavior that includes the affective, cognitive, and psychomotor domains of learning and performance.26,27 Any delay in calling a Mayday reduces the chance of survival and increases the risk to other fire fighters trying to rescue the downed fire fighter.
Firefighters should be 100% confident in their competency to declare a Mayday for themselves. Fire departments should ensure that any personnel who may enter an IDLH environment meet the Authority Having Jurisdiction standards for Mayday competency throughout their active duty service. Presently there are no national Mayday standards for firefighters to be trained to and most states do not have Mayday standards. A rapid intervention team (RIT) will typically not be activated until a Mayday is declared. Any delay in calling the Mayday reduces the window of survivability and also increases the risk to the RIT.27, 28, 29, 30
There are no rules on when a fire fighter must call a Mayday, and Mayday training is not included in the job performance requirements in NFPA Fire Fighter 1 or 2 standards.2 It is up to each authority having jurisdiction to develop rules and performance standards for a fire fighter to call a Mayday. The National Fire Academy Mayday courses present specific Mayday parameters or rules for when a fire fighter must call a Mayday. The courses may help fire departments in developing and teaching Mayday procedures for fire fighters.
The National Fire Academy has two courses addressing the fire fighter Mayday Doctrine, Q133 Firefighter Safety: Calling the Mayday, which is a 2-hour program covering the cognitive and affective learning domain of the fire fighter Mayday Doctrine, and H134 Calling the Mayday: Hands-on Training, which is an 8-hour course that covers the psychomotor learning domain of the fire fighter Mayday Doctrine. These courses are based on the military methodology used to develop and teach fighter pilots ejection doctrine. A training CD is available to fire departments free of charge from the U.S. Fire Administration Publications office.27, 28
Also, the IAFF Fire Ground Survival program is another resource fire departments can use and was developed to ensure that training for Mayday prevention and Mayday operations are consistent between all fire fighters, company officers, and chief officers.23
Any Mayday communication must contain the location of the firefighter in as much detail as possible and, at a minimum, should include the division (floor) and quadrant. It is imperative that firefighters know their location when in IDLH environments at all times to effectively be able to give their location in the event of a Mayday. Once in distress, firefighters must immediately declare a Mayday. The following example uses LUNAR (Location, Unit, Name, Assignment/Air, Resources needed) as a prompt: "Mayday, Mayday, Mayday, Division 1 Quadrant C, Engine 71, Smith, search/out of air/vomited, can't find exit." When in trouble, a firefighter's first action must be to declare the Mayday as accurately as possible. Once the IC and RIT know the fire fighter's location, the firefighter can then try to fix the problem, such as clearing the nose cup, while the RIT is en route for rescue.28
A fire fighter who is breathing carbon monoxide (CO) quickly loses cognitive ability to communicate correctly and can unknowingly move away from an exit, other fire fighters, or safety before becoming unconscious. Without the accurate location of a downed fire fighter, the speed at which the RIT can find them is diminished, and the window of survivability closes quickly because of lack of oxygen and high CO concentrations in an IDLH environment.27, 28, 29
Fire fighters also need to understand the psychological and physiological effects of the extreme level of stress encountered when they become lost, disoriented, injured, run low on air, or become trapped during rapid fire progression. Most fire training curricula do not include discussion of the psychological and physiological effects of extreme stress, such as encountered in an imminently life-threatening situation, nor do they address key survival skills necessary for effective response. Understanding the psychology and physiology involved is an essential step in developing appropriate responses to life-threatening situations. Reaction to the extreme stress of a life-threatening situation, such as being trapped, can result in sensory distortions and decreased cognitive processing capability.26 In the book Stress and Performance in Diving, the author notes that while all training is important, "We know that under conditions of stress, particularly when rapid problem-solving is crucial, over-learning responses is essential. The properly trained individual should have learned coping behavior so well that responses become virtually automatic requiring less stop and think performance."31 Fire fighters should never hesitate to declare a Mayday. There is a very narrow window of survivability in a burning, highly toxic building. Any delay declaring a Mayday reduces the chance for a successful rescue.30
In this incident, the victim and his partner were already low on air and their low-air alarms were sounding when they passed the stairwell exit, possibly to check on the progress on the fire-fighting operation. The pair made it to the hallway that was involved in fire and started back to the exit when the victim ran out of air and told his partner they needed to buddy breath. The victim experienced an uncontrolled SCBA emergency and likely vomited in his facepiece and removed his mask. When the victim asked his partner to connect his buddy breather connection, he did not control the release of air and all of the partner's air escaped through the victim's SCBA. The victim told his partner to transmit a Mayday and activate his PASS. A Mayday was transmitted by the victim's partner and the partner removed his SCBA and began looking for an escape path.
Recommendation #11: Fire departments should ensure that the incident commander designates a incident safety officer and assistant incident safety officers as necessary.
Discussion: NFPA 1561 Standard on Emergency Services Incident Management System, 2008 edition, states in Paragraph 5.3.1 that "The incident commander shall have overall authority for management of the incident."23 Moreover, NFPA 1561 Paragraph 5.3.2 states, "The incident commander shall ensure that adequate safety measures are in place."23 With the advent of the Incident Command System, the goal was to ensure that the incident commander was responsible for the safety and welfare of all members and other first responders that were on-scene at an incident.
Based upon the size and complexity (e.g. high-rise fire) of an incident, the incident commander must delegate responsibilities that include safety. The Incident Command System can be expanded to include functions necessary to command and control of the incident. Though the incident commander is still responsible for the safety and welfare of all members and first responders on-scene, this responsibility is delegated to the incident safety officer.8
A fire department should develop response procedures that ensure a pre-designated incident safety officer, independent of the incident commander, responds automatically to pre-designated incidents. Upon arrival at the incident, the designated safety officer should meet with the incident commander to confirm the incident safety officer assignment and be integrated into the personnel accountability system. Upon confirmation, the incident safety officer should obtain the following information:
- Overall situation status and resource status.
- The incident action plan.
- Known hazards and concerns plus the establishment of control zones.
- Status or rapid intervention crews.
- Establishment of the Rehabilitation Group.
- Confirmation of established radio communication channels (Command Channel, Tactical Channels).
Once the information is obtained, the incident safety officer should don the personal protective equipment appropriate for the potential hazards that he/she will be exposed to. Also, the incident safety officer should be identified by a vest or helmet. The incident safety officer should perform a reconnaissance of the incident and began initiating functions of this position.
Based upon the size and complexity of the incident, such as this incident in a high-rise structure, the incident safety officer may request the appointment of assistant incident safety officers.
Types of incidents that might require expansion of the safety officer role include the following:
- Incidents covering a large geographical area (e.g. high-rise structure) that include numerous branches, divisions, or groups.
- Incidents where significant acute or chronic responder health concerns require coordination and input to the Planning section (responsible for accounting for the organizational structure, availability of resources, deployment of resources, and the situation status reports).
- Incidents requiring interface with local, state, federal, or other health and safety representatives.
- Multi-agency incidents where Unified Command is established.
- Incidents where Area Command is established.32
Assistants to the Incident Safety Officers (AISOs) assigned to sections, branches, divisions, or groups can be addressed according to their area of responsibility. For example, an assistant incident safety officer assigned to "Division 5" can be addressed as "Division 5 Assistant Incident Safety Officer." The assistant incident safety officers assigned to sections, branches, divisions, or groups report to and follow direction from the safety officer in the command staff, but the assistant safety officer works with the supervisory person in the assigned section, branch, division, or group to assure safety conditions are being met.7, 14, 23
At this incident, the department's pre-designated incident safety officer responded to this incident but was deployed to other functions. The functions included deploying fire line tape and assisting the Incident Commander with strategy and tactics plus personnel accountability.
Recommendation #12: Fire departments should ensure that staffing levels are maintained and effectively utilized.
Discussion: The National Fire Protection Association (NFPA) 1710 Standard identifies the minimum resources for an effective fire-fighting force to perform critical tasks. These tasks include establishing water supply, deploying an initial attack line, ventilating, performing search and rescue, and establishing a RIT. NFPA 1710 recommends that the minimum staffing levels for an engine company to perform effective and efficient fire suppression tasks is four, and may not be from the same unit.33 In addition, a recently released study by the National Institute for Standards and Technology (NIST), Report on Residential Fireground Field Experiments, concluded that a three-person crew started and completed a primary search and rescue 25 percent faster than a two-person crew and that four- or five-person crews started and completed primary search and rescue 6 percent faster than a three-person crew.34
Staffing deficits cause tactical difficulties, reduced information flow and may indirectly impact proper command decisions. Staffing levels must be sufficient to perform the critical fireground tasks (which in the case of a commercial structures are more complex) to save life (which includes the fire fighters themselves) and property. It is essential that staffing levels are sufficient to have a dedicated RIT crew at every fireground and that any on-scene assignments will not hamper the RIT team's immediate response to the fire fighter down or Mayday situation.30, 31, 33 The RIT crew, as well as being a dedicated crew, must have specialized rapid intervention equipment dedicated to the priorities of locating the downed fire fighter, determining respiratory needs, supplying air if needed, conducting extraction from the IDLH if possible, and/or protecting trapped fire fighters in place if necessary.34 The RIT training should comply with NFPA 1407.35
During this incident, several engines were riding a person short. Several engineers that were not required to staff the pump could have been utilized as a crew member to help stretch the high-rise pack hoselines.
Recommendation #13: Fire departments should use thermal imaging cameras (TICs) during the search and fire-fighting operations.
Discussion: Thermal imaging cameras (TIC) provide a technology with potential to greatly enhance fire fighter safety and improve the ability to perform tasks such as size-up, search and rescue, fire attack, and ventilation.
At a structure fire, the thermal imaging camera may help identify the location of the fire or the extent of fire involvement prior to fire fighters being deployed into a structure. Knowing the location of the fire may help fire fighters determine the best approach to the fire and avoid structural damage in a building that might have otherwise been undetectable.
The TIC provides information that crews making the fire attack would not previously have due to poor visibility and building construction. Using this information, fire fighters can locate the fire more quickly and ensure that the water application is effective. One of the most important aspects of the TIC is the ability to detect a fire that is isolated or hidden within parts of structure. While TICs provide useful information to aid in locating the seat of a fire, they cannot be relied upon to assess the strength or safety of floors and ceilings.36 TICs should be used in a timely manner, and fire fighters should be properly trained in their use and be aware of their limitations.37-38 While the use of a TIC is important, research by Underwriters Laboratories has shown that there are significant limitations in the ability of these devices to detect temperature differences behind structural materials, such as the exterior finish of a building or outside compartment linings (i.e., walls, ceilings, and floors).39
Of all the operations in which the TIC can improve a fire fighter's efforts, this technology has the most dramatic impact on search and rescue. Fire fighters using thermal imagers can see the room, which enables them to quickly navigate and identify victims. Without a thermal imager, fire fighters search burning buildings by crawling on their hands and knees through blinding smoke to try and locate possible victims. Thermal imagers can also provide a method for fire fighters to track and locate other fire fighters in limited visibility conditions.
From a ventilation perspective, fire fighters can use the thermal imaging camera to identify areas of heat accumulation, possible ventilation points, and significant building construction features. This helps ensure proper and effective ventilation that successfully removes smoke and heat from a building.
At this incident, the fire department had TICs on all truck companies and the heavy rescue company, but they were not used in the building. Engine companies did not have TICs and were operating in blinding conditions on the fire floor.
Recommendation #14: Fire departments should ensure that a respiratory protection plan includes consideration for using larger-volume SCBA cylinders in target areas (e.g., high-rise) that may require longer-duration work times.
A typical 30-minute (1200L) SCBA may not provide an effective quantity of breathing air for fire fighters working in high-rise buildings or large, complex structures. The 1200L cylinder will last an average firefighter actively engaged in suppression activities about 15–18 minutes. 16 NFPA 1852 Standard on Selection, Care and Maintenance of Open-Circuit Self-Contained Breathing Apparatus for Emergency Services A.5.1.5(18) 40 states, during extreme exertion, for example, actual service time can be reduced by 50 percent or more. In addition to the degree of user exertion, other conditions that effect the SCBA service time include:
- Physical condition of the fire fighter.
- Emotional conditions, such as fear or excitement that can increase the user’s breathing rate.
- Degree of training or experience the user has had with such equipment.
- Whether or not the cylinder is fully charged at the beginning of use.
- Facepiece fit.
- Use in a pressurized tunnel or caisson [at two atmospheres of pressure (29.4 psig), the duration is one-half the duration obtained at one atmosphere].
- Condition of the SCBA
- The SCBA dead space [a volume proportional to the carbon dioxide (CO2) concentration in the inhaled breathing gas. An increase of CO2 in the inhalation air leads to increased ventilation and, consequently, shorter service time for a given air supply. Reducing CO2 in the inhalation air by using, for example, a well-fitting nose cup has been demonstrated to give longer service time].
Fire departments must ensure that fire fighters have enough air in their SCBA's to complete the mission in their areas. A 30-minute (1200L) SCBA might be sufficient for companies responding to a typical 2- or 3-bedroom suburban residential area, but might not be sufficient for companies responding to high-rise or large complex structures. The fire fighters must have enough air by volume to effectively provide a work period inside an IDLH atmosphere and still contain enough air volume to exit the IDLH with their reserve air intact. An assessment can identify areas in a jurisdiction that demand additional breathing due to the type of occupancy or hazard, and companies assigned to those areas can be equipped with the larger cylinders. A modern SCBA cylinder is made of significantly lighter materials and contains higher pressure, greater volume, and smaller profile. All SCBA manufacturers are now offering these SCBA cylinders, and some manufacturers are offering higher pressure (5500 psi) SCBA, which reduce the weight and increase the volume over existing SCBA. The IAFF is currently working with a manufacturer to develop a significantly reduced profile SCBA that can also increase the available breathing air ("flat-pack" SCBA). 41 Currently, many fire departments perform a needs assessment for hazards, such as tunnel rescues, and provide those specialty companies with closed circuit SCBA (re-breathers) to increase the amount of time fire fighters have to complete a mission. The most important part of the needs assessment is to identify the areas of the jurisdiction that need the increased air volumes and then provide the equipment and training to those companies that respond or could be called upon to respond to incidents in those areas. NFPA 1852 Standard on Selection, Care and Maintenance of Open-Circuit Self-Contained Breathing Apparatus for Emergency Services,40 provides fire departments with basic criteria for evaluation and selecting open-circuit SCBA.
In this incident the fire department provided current edition, certified SCBAs with 4500 psi composite 1200L (30-minute) cylinders to all fire fighters throughout the department. Many fire fighters reported that EOSTIs were sounding inside the high-rise structure in the IDLH atmospheres. Fire departments should ensure that a plan is in place to provide spare cylinders in areas free from an IDLH atmosphere (such as a staging area on the upper floors below the fire) where fire fighters can replenish their air supply in the event of great distances to get to a suitable exit.
Additionally,
Recommendation #15: States and municipalities should adopt and enforce regulations for automatic fire sprinkler protection in new buildings and renovated structures.
Discussion: The International Code Council's International Residential Code and the NFPA 101 Life Safety Code require sprinkler protection in all new one- and two-family dwellings and in most other properties.42-43 Fire development beyond the incipient stage is one of the greatest hazards that fire fighters are exposed to. This exposure and risk to fire fighters can be dramatically reduced when fires are controlled or extinguished by automatic sprinkler systems. NFPA statistics show that most fires in sprinklered buildings are controlled by the activation of one or two sprinkler heads prior to fire department arrival. The presence of automatic fire sprinklers also reduces the exposure risk to fire fighters in rescue situations by allowing the safe egress of building occupants before the fire department arrives on scene. Finally, by controlling fire development, the exposure to hazards such as building collapse and overhaul operations are greatly reduced, if not eliminated.
References
- NFPA [2007]. NFPA 1582 Standard for medical requirements for fire service personnel. Quincy, MA: National Fire Protection Association.
- NFPA [2008]. NFPA 1001 Standard for fire fighter professional qualifications, Fire Fighter I and Fire Fighter II. Quincy, MA: National Fire Protection Association.
- Weather Underground Inc. [2011]. Weather History http://www.wunderground.com/history/index.html.
- ATF [2011]. Agency report #763056-11-0036. Washington, DC: The Bureau of Alcohol, Tobacco, and Firearms.
- USFA [1996]. Special report: operational considerations for high-rise firefighting. Emmitsburg, MD: Federal Emergency Management Agency, United States Fire Administration http://www.usfa.fema.gov/downloads/pdf/publications/tr-082.pdf.
- Los Angeles Fire Department [2007]. Los Angeles Fire Department high-rise manual, 2007 ed. Los Angeles, CA: Los Angeles Fire Department.
- National Incident Management System Consortium [2008]. Incident Command System (ICS) Model Procedures Guide for Incidents Involving Structural Fire Fighting, High-Rise, Multi-Casualty, Highway, and Managing Large-Scale Incidents Using NIMS ICS, Book 1. Fire Protection Publications, Oklahoma State University.
- NFPA [2007]. NFPA 1500 Standard on Fire Department Occupational Safety and Health Program, 2007 ed. Quincy, MA: National Fire Protection Association.
- National Fire Academy [2005]. Advanced Safety Operations and Management. Emmitsburg, MD: Federal Emergency Management Agency, United States Fire Administration. 8. National Fire Academy [2004]. Incident safety officer (ISO), 2004 ed. Emmitsburg, MD: Federal Emergency Management Agency, United States Fire Administration.
- National Fire Academy [2006]. ICS 300: Intermediate ICS for expanding incidents for operational first responders (p65), 2006 ed. Emmitsburg, MD: Federal Emergency Management Agency, United States Fire Administration.
- Norman J [2005]. Fire officer's handbook, 3rd ed. Tulsa, OK: Penn Well Corporation, Fire Engineering.
- NFPA [2006]. NFPA 92A. Standard for Smoke-Control Systems Utilizing Barriers and Pressure Differences.
- NIST [2007]. NISTR 7412. Evaluating Positive Pressure Ventilation In Large Structures: High-Rise Pressure Experiments. [http://www.firehouse.com/article/ 10498807/500-maydays-called-in-rookie-school].
- FIRESCOPE [2007]. Field operations guide, 2007 ed. Riverside, CA. FIRESCOPE. ICS 420-1
- FIRESCOPE [2007]. High-rise structure fire operational system description. Riverside, CA: FIRESCOPE, ICS-HR-120-1.
- Gagliano M, Phillips C, Jose P, Bernocco S [2008]. Air management for the Fire Service. Tulsa, OK: Penn Well Corporation, Fire Engineering.
- NFPA [2006]. NFPA 1404 Standard for fire service respiratory protection training. Quincy, MA: National Fire Protection Association.
- Purser, David A., Assessment of Hazards to Occupants from Smoke, Toxic Gases, and Heat. "The SFPE Handbook of Fire Protection Engineering, Fourth Edition" 2008.
- Bureau of Alcohol, Tobacco, Firearms and Explosives. Subject: Acute Carbon Monoxide Exposure Research. February 16, 2012.
- NIOSH [2011]. Career fire fighter dies while conducting a search in a residential house fire–Kansas. Morgantown, WV: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, Fatality Assessment and Control Evaluation (FACE) Report F2010-13 http://www.cdc.gov/niosh/fire/reports/face201013.html.
- NFPA [2007]. NFPA 1981 Standard on open-circuit self-contained breathing apparatus for emergency services. Quincy, MA: National Fire Protection Association.
- Ciarrocca M, Harms T [2011]. Help on the scene. Fire Rescue Magazine 29(2):40–48.
- NFPA [2008]. NFPA 1561 Standard on emergency services incident management system, 2008 ed. Quincy, MA: National Fire Protection Association.
- Sendelbach TE [2004]. Managing the fireground Mayday: the critical link to firefighter survival http://www.firehouse.com/article/10541890/managing-the-fireground-mayday]. Date accessed: March, 2012.
- IAFF [no date]. IAFF Fire Ground Survival Program. Washington, DC: International Association of Fire Fighters [http://www.iaff.org/HS/FGS/FGSIndex.htm]. Date accessed: March 2012.
- Grossman D, Christensen L [2008)]. On combat: the psychology and physiology of deadly conflict in war and peace, 3rd ed. Millstadt, IL: Warrior Science Publications.
- Clark BA [2005]. "Strategy and Tactics" - 500 Mayday called in rookie school http://www.firehouse.com/article/10498807/500-maydays-called-in-rookie-school.
- U.S. Fire Administration [2006]. Mayday CD Q133 Firefighter safety: calling the Mayday and H134 Calling the Mayday: hands on training. Emmitsburg, MD: U.S. Department of Homeland Security, U.S. Fire Administration, National Fire Academy.
- Clark BA [2008]. Leadership on the line: firefighter Mayday doctrine—where are we now? Radio@Firehouse.com http://www.firehouse.com/podcast/10459336/leadership-on-the-line-firefighter-mayday-doctrine-where-are-we-now. (Link updated 10/4/2012)
- IAFC Safety, Health, and Survival Section [2010]. Rules of engagement of structural firefighting [http://www.iafcsafety.org/image/ROE_Poster.pdf. Date Accessed: March 2012.
- Bachrach A, Egstrom G [1987]. Stress and performance in diving. San Pedro, CA: Best Publishing.
- NFPA [2008]. NFPA 1521 Standard for fire department safety officer. Quincy, MA: National Fire Protection Association.
- NFPA [2010]. NFPA 1710 Standard for the organization and deployment of fire suppression operations, emergency medical operations, and special operations to the public by career fire departments. Quincy, MA: National Fire Protection Association.
- NIST [2010]. Report on residential fireground field experiments. NIST Technical Note 1661, April http://www.nist.gov/el/fire_research/upload/Report-on-Residential-Fireground-Field-Experiments.pdf. Date accessed: November 2011.
- NFPA [2010]. NFPA 1407: Standard for training fire service rapid intervention crews. Quincy, MA: National Fire Protection Association.
- Klaene BJ, Sanders RE[2000]. Structural fire fighting. Quincy, MA: National Fire Protection Association.
- NIOSH [2009]. Workplace Solutions: Preventing deaths and injuries of fire fighters working above fire-damaged floors. Cincinnati, OH: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, DHHS (NIOSH) Publication No. 2009-114 http://www.cdc.gov/niosh/docs/wp-solutions/2009-114/default.html.
- Corbin DE [2000]. Seeing is believing. Occup Saf Health 69(8):60–67.
- Underwriters Laboratories [2009]. Structural stability of engineered lumber in fire conditions http://lms.ulknowledgeservices.com/catalog/display.resource.aspx?resourceid=187716. Date accessed: February 17, 2010. (Link Updated 5/13/2015)
- NFPA [2008]. NFPA 1852 Standard on selection, care and maintenance of open-circuit self-contained breathing apparatus for emergency services. Quincy, MA: National Fire Protection Association.
- IAFF [2010]. News Release, IAFF and DHS select MSA to build next-generation SCBA prototype http://www.iaff.org/Comm/PDFs/SCBA.pdf. Date accessed: November 30, 2011.
- International Code Council [2009]. International residential code for one and two-family dwellings. Washington, DC: International Code Council.
- NFPA [2010]. NFPA 101 Life safety code. Quincy, MA: National Fire Protection Association.
Investigator Information
This incident was investigated by Matt E. Bowyer, General Engineer, Stephen Miles, Safety and Occupational Health Specialist, and Murrey Loflin, Investigator, with the Fire Fighter Fatality Investigation and Prevention Program, Surveillance and Field Investigations Branch, Division of Safety Research, NIOSH located in Morgantown, WV. An expert technical review was provided by Robert D. Neamy, Deputy Chief (Retired), Los Angeles Department. A technical review was also provided by the National Fire Protection Association, Public Fire Protection Division.
Additional Information Sources
The Occupational Safety and Health Administration published a document in 2006 entitled: "Fire Service Features of Buildings and Fire Protection Systems", which contains chapters on standpipe systems and FDCs, among others. The link to the electronic version of manual is here: https://www.osha.gov/Publications/fire_features3256.pdf
NFPA 5000: Building Construction and Safety Code, 2012, defines a high-rise as buildings 75 feet or greater in height measured from the lowest level of fire department vehicle access to the floor of the highest occupiable story.
Disclaimer
Mention of any company or product does not constitute endorsement by the National Institute for Occupational Safety and Health (NIOSH). In addition, citations to Web sites external to NIOSH do not constitute NIOSH endorsement of the sponsoring organizations or their programs or products. Furthermore, NIOSH is not responsible for the content of these Web sites.
APPENDIX 1
Status Investigation Report of Two
Self-Contained Breathing Apparatus
Submitted By the
NIOSH Division of Safety Research (DSR) for the
North Carolina Fire Department
NIOSH Task Number 17985
Background
As part of the National Institute for Occupational Safety and Health (NIOSH) Fire Fighter Fatality Investigation and Prevention Program, the Technology Evaluation Branch agreed to examine and evaluate two SCBA units identified as Scott Health and Safety model AirPak 4.5, 4500 psig, 30-minute, self-contained breathing apparatus (SCBA).
This SCBA status investigation was assigned NIOSH Task Number 17985. The NIOSH Division of Safety Research (DSR) was advised that NIOSH/NPPTL/TEB would provide a written report of the inspections and any applicable test results.
The SCBA units, contained within corrugated cardboard boxes, were delivered to the NIOSH facility in Bruceton, Pennsylvania, on August 19, 2011. After their arrival, the packages were taken to building 20 and stored under lock until the time of the evaluations.
SCBA Inspection
The packages were opened in the General Respirator Inspection Area (building 20) on November 15 and November 17, 2011, and a complete visual inspection of the units was conducted by Tom Pouchot, General Engineer, NPPTL. These SCBA units were examined, component by component, in the condition received to determine the conformance of each unit to the NIOSH approved configuration. The visual inspection process was documented photographically.
The SCBA identified with the marking of RS3 fire fighter was labeled by NPPTL as SCBA Unit #1. The SCBA identified as the victim’s was labeled by NPPTL as SCBA Unit #2. The units were identified as the Scott Health and Safety Company model AirPak 4.5, 30-minute, 4500 psig unit, NIOSH approval number for Unit #1 TC-13F-0076CBRN and Unit #2 was TC-13F-0076. Once the visual inspections were completed, the SCBA units were repackaged and placed back in Building 20 under lock.
The complete SCBA inspections are summarized in Appendix I. The condition of each major component of the SCBA that were photographed with a digital camera is contained in Appendix III of full report. It was judged that both units could be safely pressurized and tested. Unit #2 was tested using a substitute cylinder and facepiece from Unit #1. The substitute cylinder and facepiece were used on Unit #2 for all the NIOSH and NFPA tests that were performed.
SCBA Testing
The purpose of the testing was to determine the conformance of each SCBA to the approval performance requirements of Title 42, Code of Federal Regulations, Part 84 (42 CFR 84). Further testing was conducted to provide an indication of the conformance of each SCBA to the National Fire Protection Association (NFPA) Air Flow Performance requirements of NFPA 1981, Standard on Open-Circuit Self-Contained Breathing Apparatus for the Fire Service, 1997 Edition.
NIOSH SCBA Certification Tests (in accordance with the performance requirements of 42 CFR 84):
- Positive Pressure Test [§ 84.70(a)(2)(ii)]
- Rated Service Time Test (duration) [§ 84.95]
- Static Pressure Test [§ 84.91(d)]
- Gas Flow Test [§ 84.93]
- Exhalation Resistance Test [§ 84.91(c)]
- Remaining Service Life Indicator Test (low-air alarm) [§ 84.83(f)] National Fire Protection Association (NFPA) Tests (in accordance with NFPA 1981, 1997 Edition)
- Air Flow Performance Test [Chapter 5, 5-1.1]
Units #1 and #2 were tested on December 1 and 15, 2011. Unit #2 utilized a substitute cylinder and facepiece from Unit #1.
Appendix II contains the complete NIOSH and NFPA test reports for each of the SCBA. Tables One and Two summarize the NIOSH and NFPA test results.
Summary and Conclusions
Two SCBA units from the North Carolina Fire Department were submitted to NIOSH NPPTL by the NIOSH Division of Safety Research for evaluation. The SCBA units were delivered to NIOSH on August 19, 2011, and inspected on November 15 and 17, 2011. The units were identified as Scott Health and Safety model AirPak 4.5, 4500 psig, 30-minute, SCBA units (NIOSH approval numbers TC-13F-0076CBRN and TC-13F-0076). The units suffered minimal damage; exhibited other signs of wear and tear; and the units were covered lightly with general dirt, grime, and foreign particulate material. The cylinder valves as received, Unit #1 was in the closed position and Unit #2 was in the closed position. The cylinder gauges read approximately 0 psig. The cylinder valve hand wheel could be turned on Unit #1 but could not be turned on Unit #2. The regulator and facepiece mating and sealing areas on the units were relatively clean and there was extensive debris on the inside of the Unit #2 facepiece. The rubber faceseals on the units were in good condition. The harness webbing on the units was in good condition with no fraying or tears, but the webbing was slightly dirty. The PASS device on the Unit #1 functioned, but the PASS device on Unit #2 did not function. New batteries were installed on Unit #2 and the PASS device did function. The NFPA approval labels on the units were present and readable. Visibility through the lens of the unit facepieces was fair to good as the lenses had some scratches and a slight amount of foreign material present.
The air cylinder on the Unit #1 had a manufactured date of 8/04. Under the applicable DOT-E-10915-4500 exemption, the air cylinder is required to be hydro tested every 5 years, starting on or before the last day of 8/09. Therefore, it appears that the cylinder on this SCBA unit was due for hydro testing before the end of August 2009. There was a re-test label on the cylinder assembly for Unit #1 with a date of 3/10. Therefore, it appears that this cylinder was within the hydro certification when last used. The Unit #1 cylinder also had some light scratches with the outer resin.
The air cylinder on the Unit #2 had a manufactured date of 10/98. Under the applicable DOT-E-10915-4500 exemption, the air cylinder is required to be hydro tested every 5 years, starting on or before the last day of 10/03. Therefore it appears that the cylinder on this SCBA unit was due for hydro testing before the end of October 2003 and repeat testing before the end of October 2008. The re-test label indicates that the last hydro test was performed 11/07. Therefore, it appears that this cylinder was within the hydro certification when last used. Unit #2 cylinder also had some light scratches and scuffs over the whole assembly with a wear spot near the cylinder valve. A replacement air cylinder for Unit #2 was used from Unit #1 along with the Unit #1 facepiece. No other maintenance or repair work was performed on the units at any time.
SCBA Unit #1 met the requirements of the NIOSH Positive Pressure Test, with a minimum pressure of 0.2 inches of water. Unit #1 did meet the requirements of all of the other NIOSH tests. This unit failed the NFPA test as the HUD was not functional. SCBA unit #2 met the requirements of the NIOSH Positive Pressure Test, with a minimum pressure of 0.2 inches of water. Unit #2 did meet all the requirements of all the other NIOSH tests. This unit failed the NFPA test as the HUD was not functional.
In light of the information obtained during this investigation, NIOSH has proposed no further action on its part at this time. Following inspection and testing, the SCBA units were returned to storage pending return to the North Carolina Fire Department. If the units are to be placed back in service, the SCBAs must be repaired, damaged components replaced, tested, and inspected by a qualified service technician, including such testing and other maintenance activities as prescribed by the schedule from the SCBA manufacturer. Typically a flow test is required on at least an annual basis.
The National Institute for Occupational Safety and Health (NIOSH), an institute within the Centers for Disease Control and Prevention (CDC), is the federal agency responsible for conducting research and making recommendations for the prevention of work-related injury and illness. In 1998, Congress appropriated funds to NIOSH to conduct a fire fighter initiative that resulted in the NIOSH "Fire Fighter Fatality Investigation and Prevention Program" which examines line-of-duty-deaths or on duty deaths of fire fighters to assist fire departments, fire fighters, the fire service and others to prevent similar fire fighter deaths in the future. The agency does not enforce compliance with State or Federal occupational safety and health standards and does not determine fault or assign blame. Participation of fire departments and individuals in NIOSH investigations is voluntary. Under its program, NIOSH investigators interview persons with knowledge of the incident who agree to be interviewed and review available records to develop a description of the conditions and circumstances leading to the death(s). Interviewees are not asked to sign sworn statements and interviews are not recorded. The agency's reports do not name the victim, the fire department or those interviewed. The NIOSH report's summary of the conditions and circumstances surrounding the fatality is intended to provide context to the agency's recommendations and is not intended to be definitive for purposes of determining any claim.
For further information, visit the program Web site at www.cdc.gov/niosh/fire
or call toll free 1-800-CDC-INFO (1-800-232-4636).
- Page last reviewed: November 18, 2015
- Page last updated: October 15, 2014
- Content source:
- National Institute for Occupational Safety and Health Division of Safety Research