


A Career Lieutenant and a Career Fire Fighter Found Unresponsive at a Residential Structure Fire Connecticut
 ShareCompartir
ShareCompartir
 Death in the Line of Duty...A summary of a NIOSH fire fighter fatality investigation
Death in the Line of Duty...A summary of a NIOSH fire fighter fatality investigation
F2010-18 Date Released: June 1, 2011
Executive Summary
On July 24, 2010, a 40-year-old male career lieutenant (Victim #1) and a 49-year-old male career fire fighter (Victim #2) were found unresponsive at a residential structure fire. The victims and two additional crew members were tasked with conducting a primary search for civilians and fire extension on the 3rd floor of a multifamily residential structure. The fire had been extinguished on the 2nd floor upon their entry into the structure. While pulling walls and the ceiling on the 3rd floor, smoke and heat conditions changed rapidly. Victim #1 transmitted a Mayday (audibly under duress) that was not acknowledged or acted upon. Minutes later the incident commander ordered an evacuation of the 3rd floor. As a fire fighter exited the 3rd floor, Victim #1 was discovered unconscious and not breathing, sitting on the stairs to the 3rd floor. Approximately 7 minutes later, Victim #2 was discovered on the 3rd floor in thick, black smoke conditions. Both victims were removed by the rapid intervention team (RIT) and other fire fighters who assisted them. Both victims were pronounced dead at local hospitals.

|
Incident structure following extinguishment. |
Contributing Factors
- Failure to effectively monitor and respond to Mayday transmissions
- Less than effective Mayday procedures and training
- Inadequate air management
- Removal and/or dislodgement of self-contained breathing apparatus (SCBA) facepiece
- Incident safety officer (ISO) and rapid intervention team (RIT) not readily available on scene
- Possible underlying medical condition(s) (coronary artery disease)
- Command, control, and accountability.
Key Recommendations
- Ensure that radio transmissions are effectively monitored and quickly acted upon, especially when a Mayday is called
- Ensure that Mayday training program(s) and department procedures adequately prepare fire fighters to call a Mayday
- Train fire fighters in air management techniques to ensure they receive the maximum benefit from their SCBA
- Ensure that fire fighters use their SCBA during all stages of a fire and are trained in SCBA emergency procedures
- Ensure that a separate incident safety officer (ISO), independent from the incident commander, is appointed at each structure fire with the initial dispatch
- Ensure that a rapid intervention team (RIT) is readily available and prepared to respond to fire fighter emergencies
- Consider adopting a comprehensive wellness and fitness program, provide annual medical evaluations consistent with NFPA standards, and perform annual physical performance (physical ability) evaluations for all fire fighters.

|
Incident scene. |
Introduction
On Saturday, July 24, 2010, a 40-year-old male career lieutenant (Victim #1) and a 49-year-old male career fire fighter (Victim #2) were found unresponsive at a residential structure fire. Both were transported to local hospitals where they were pronounced dead. On July 26, 2010, the U.S. Fire Administration notified the National Institute for Occupational Safety and Health (NIOSH) of this incident. On July 30, two safety and occupational health specialists from the NIOSH Fire Fighter Fatality Investigation and Prevention Program (FFFIPP) traveled to Connecticut to investigate this incident. The NIOSH investigators met with the deputy fire chief and representatives from the local fire fighters' union; the fire department's training division; the State of Connecticut Department of Public Safety, Division of State Police, Office of State Fire Marshal; health department; the local civil service director; private ambulance service; and the State of Connecticut's Department of Labor, Division of Occupational Safety and Health (CONN-OSHA). Interviews were conducted with the deputy fire chief, training division staff, the health department physician, a member of the fire fighter's union safety and productivity committee, the incident commander (IC), the general manager of the private ambulance service, fire fighters who were on scene, and the director of public safety communications. NIOSH investigators met with the state police to inspect and photograph the victims' structural fire fighting gear and self-contained breathing apparatus (SCBA) involved in the incident, and to review witness statements, photographs, and other available information obtained during their investigation. The NIOSH investigators visited, documented, and photographed the fire scene and structure. The NIOSH investigators reviewed the victims' pre-employment medical evaluations, annual medical evaluations, annual respirator fit testing, and medical examiner reports. The NIOSH investigators also reviewed training records for the victims and the IC, dispatch radio transcripts, photos and videos taken by bystanders, department standard operating procedures (SOPs), and SCBA air quality testing results and maintenance records. On January 20, 2011, a NIOSH investigator and the NIOSH Fatality Investigations Team Chief returned to Connecticut to meet with the fire chief and with representatives with CONN-OSHA and the state police.
Fire Department
This career fire department has 8 stations with 292 uniformed members which serve a population of approximately 140,000 within an area of about 17 square miles. At the time of the incident the fire department had 9 engines, 4 aerial ladders, and a heavy rescue truck.
Fire Department Operations
Field personnel within the fire department are divided into four platoons to cover two shifts a day. Each platoon works three straight 10-hour day shifts, followed by three days off, then three straight 14-hour night shifts. This averages out to a 42-hour workweek. Fire fighters can work overtime, which allows them to work 24 or more hours in a row.
The fire department's training division works from 0900 to 1630, Monday through Friday. The training division is responsible for assigning a designated incident safety officer (ISO) to respond to incidents that require one (e.g., hazardous materials responses and confirmed working structure fires). Training staff within this division are assigned as the on-duty ISO during normal duty hours. After normal business hours and on weekends, an ISO is placed on an on-call status. The ISO is dispatched per dispatch protocols or upon request from the IC. The ISO will respond in a fire department vehicle from his/her home to the incident location with all required equipment to perform their duties.
The fire department has written operational procedure guidelines, standard operating procedures, and directives (OPG/SOP/D) that cover a wide range of administrative and operational topics.1 Those OPGs/SOPs/Ds specific to this incident include the following:
- Mayday Procedures (see summary of procedure in Appendix I)
- SCBA Operation and Maintenance Instructions
- Use of SCBA
- SCBA Emergency Escape
- Personal Alert Safety System (PASS) Devices
- Rapid Intervention Team (RIT)
- Emergency Evacuations
- Radio Operation Instructions
- Radio Usage Guidelines
- Radio Guidelines for Fire Ground Channels
- Initial Dispatch and Multiple Alarm Procedures
- Incident Command System
- Accountability System
- Engine and Truck Company Operations and Responsibilities
- Training Requirements
The fire department does not have a procedure or guideline for fire fighter rehab at emergency incidents.
A contracted private ambulance service provides emergency medical services (EMS) to the city and to the fire department. The fire department may first respond to medical emergencies dispatched within the city limits to assist the ambulance service. Emergencies requiring EMS are routed through the city's dispatch center and then transferred to the ambulance dispatch center, which then logs all information before dispatching the appropriate station for an ambulance to respond. No procedures or guidelines are established between the ambulance service and fire department stating that an ambulance will be automatically dispatched to standby at a fire-related incident to render medical care and rehab services to fire fighters or civilians on scene when needed.
9-1-1 Communications Center
In April 2010, the city’s fire and police 9-1-1 centers were consolidated into a new public safety communications department through a grant. Fire department lieutenants assigned to the original fire department 9-1-1 center did not transition into the new communications department, but were reassigned to the field. Civilian fire dispatchers from the fire department’s 9-1-1 center did transfer into the new communications center. Prior to the communications center’s opening, all fire dispatchers were trained on the new computer-aided dispatch and radio systems and had taken or were scheduled to take an advanced fire service dispatch class. Note: Dispatchers hired after 1990 were certified as telecommunicators through the State of Connecticut, Office of Statewide Emergency Telecommunications.
These civilian fire dispatchers had been trained on fire department policies and dispatch procedures by fire department personnel prior to transferring to the new communications center. Training included fire department procedures on handling a Mayday, and the fire department had also established a Mayday procedure test to check the viability of the Mayday SOP. According to the fire department's SOP, this test was conducted every first day shift (Monday morning) (see summary of procedures in Appendix I).
NIOSH investigators were able to meet with and interview the communications center director regarding the incident and history of the new communications center. However, NIOSH investigators did not have an opportunity to interview the actual dispatcher(s) who worked the 9-1-1 console or the supervisor(s) on duty the day of the incident. According to the communications center director, two fire dispatchers (1 originally from the fire department's 9-1-1 center) handled the fire incident. Together, they had 40 years of dispatching experience for fire and police. Two supervisors were also available in the communications center during the incident. According to training records received, the two dispatchers and two supervisors held a current State of Connecticut certification as a Public Safety Telecommunicator. The supervisors had also been certified as a Communications Center Supervisor by the Association of Public-Safety Communications Officials, or APCO.
Coincidentally, following the incident, the fire department worked with the new communications center on installing equipment that would boost radio signals in dead areas, based on problems in previous incidents. The fire department does not recall having any radio transmission problems during the incident.
State Regulations
The State of Connecticut operates an occupational safety and health program in accordance with Section 18(b) of the Occupational Safety and Health Act of 1970. CONN-OSHA has adopted all federal OSHA standards that apply to public sector employers. CONN-OSHA enforces fire department compliance with the following regulations:
- Fire Brigades2 29 CFR 1910.156(b)(1), 1910.156(c), 1910.156(c)(2), 1910.156(d)(1), 1910.156(e)(1-5)
- Respiratory Protection3 29 CFR 1910.134(c), 1910.134(e), 1910.134(f)(2), 1910.134(g)(1), 1910.134(g)(3), and 1910.134 (h)Note: This list only contains enforceable regulations related to fire incidents.
Following their investigation, CONN-OSHA determined that the fire department had violated regulations set forth by the Connecticut's Occupational Safety and Health Act. As of January 24, 2011, these citations included:
- The employer did not furnish employment and a place of employment which were free from recognized hazards that were causing or likely to cause death or serious physical harm to employees in that the employer did not follow their existing Standard Operating Procedures regarding “Maydays”.
- The employer did not follow existing Standard Operating Procedures regarding “Maydays” on July 24, 2010.
- 1910.101 (a): The employer did not determine that compressed gas cylinders under his control were in safe condition to the extent that can be determined by visual inspection. Visual and other inspections were not performed as prescribed in the Hazardous Materials Regulation of the Department of Transportation (49 CFR parts 171-179 and 14 CFR part 103). Where those regulations are not applicable, visual and other inspections shall be conducted in accordance with Compressed Gas Association Pamphlets C-6-1968 and C-8-1962, which incorporated by reference.
- Hydrostatic testing was not performed on all SCBA air cylinders that were worn by fire fighters who perform interior structure firefighting.
- 1910.134(e)(1): Medical evaluations were not provided to employees to determine the employee’s ability to use a respirator, before the employee is fit tested or required to use the respirator in the work place.
- Employer did not ensure that medical evaluations were performed on employees who wear self containing breathing apparatus (SCBA).
- 1910.134(f)(2): The employer shall ensure that an employee using a tight-fitting facepiece respirator is fit tested at least annually.
- Annual fit testing was not performed on fire fighters who wore self contained breathing apparatus while performing interior structure firefighting.
- 1910.134(g)(4)(iii): The employer did not ensure that each employee engaged in interior structural firefighting operations used SCBAs.
- The employer did not ensure that all fire fighters wore self contained breathing apparatus while performing all aspects of interior structure firefighting on July 24, 2010.
Health, Wellness, and Fit-for-duty Program
In 1999, this fire department suffered a medical line-of-duty death that was investigated by NIOSH.4 NIOSH recommendations following that incident included the following:
- Conduct annual medical evaluations of all fire fighters to determine their medical ability to perform duties without presenting a significant risk to the safety and health of themselves and others
- Reduce risk factors for cardiovascular disease and improve cardiovascular capacity by phasing in a mandatory wellness/fitness program for fire fighters
- Perform an autopsy on all on-duty fire fighters whose death may be cardiovascular related.
In early 2000, the fire department applied for a health and wellness grant that enabled them to purchase physical fitness equipment for all stations and nutritional services for approximately 2 years. At the time of the incident, fire fighters were allowed to work out at their own discretion, but no requirements or programs were established for physical fitness.
The city requires all fire fighter candidates to pass a pre-employment medical evaluation, a physical agility test, and a respirator fit test. The pre-employment medical evaluations are performed by a physician contracted by the city. The evaluation consists of a medical history, a physical examination, blood tests (complete blood count, chemistries, and lipids), urinalysis, spirometry, a resting electrocardiogram (EKG), an exercise stress test, a chest x-ray, a vision test, a hearing test, and a drug screen. Both victims successfully passed their pre-employment medical physicals.
In 2006, the fire department began offering annual medical evaluations conducted by the city's health department. The components of this evaluation are the same as the pre-employment evaluations, minus the exercise stress test, blood test, and urine drug screen. In 2007, some screening tests were added. The additional mandatory tests included pulse oximetry, color vision screening, and scoliosis screening. The additional optional tests included prostate examination; fecal blood test for colon cancer; and blood tests for diabetes, anemia, and hypercholesterolemia. In 2008, a clinician change in the health department resulted in most fire fighters not receiving their annual medical evaluation for that year, but the medical evaluations were quickly reinstated in 2009. Both victims passed their 2009 medical evaluations. In June 2010, the health department clinician made a recommendation that the fire department's annual physical evaluation meet requirements set forth in National Fire Protection Association (NFPA) 1582 Standard on Comprehensive Occupational Medical Program for Fire Departments.5
The city does not use the International Association of Fire Fighters/International Association of Fire Chiefs (IAFF/IAFC) Fire Service Joint Labor Management Candidate Physical Ability Test (CPAT) Program, which was developed as a fair and valid evaluation tool to assist in the selection of fire fighters and to ensure that all fire fighter candidates possess the physical ability to complete critical tasks effectively and safely.6 Note: The fire department has been working with city officials to bring such a test to their department. Currently, the State of Connecticut, Commission on Fire Prevention and Control offers the CPAT to interested fire fighter candidates.
In 2002, Victim #2 passed the city delivered pre-employment physical agility and strength test protocol, which consisted of: (a) torso bend and arm lift, (b) ground ladder climb, (c) stair climb, (d) sit-ups, (e) hose hoist, (f) dummy carry, and (g) dry hose pull, but he was not tested on the ground ladder climb or hose hoist. Hired in 2007, Victim #2 was not required to retake the pre-employment physical agility and strength test that he took in 2002, which made those test result 5 years old at the time of his hiring. Victim #1 was hired in 1994, and no pre-employment physical agility test records were available for Victim #1. At the time of the incident, the fire department did not require fire recruits or members of their department to pass an annual physical agility test.
The fire department annually fit tested (in house) fire department members who were required to wear a respirator or SCBA pursuant to the requirements of OSHA regulation 29 CFR 1910.134.3 Note: NIOSH investigators did not confirm if all members of the fire department had received an annual fit test. Both victims successfully completed fit testing in January 2009; they had not received their 2010 fit test by the time of the incident.
Training and Experience
The fire department's training division oversees the department's recruit training program. The length of the training program has changed over the years and, at the time of the incident, was being conducted over a 14 week period. Victim #1 and Victim #2 completed their recruit training programs in 1994 and May 2008, respectively. The current recruit training program includes the following components:
- Orientation
- Fire Fighter I and II Certification (meets State of Connecticut Fire Academy certification requirements and NFPA 1001 Standard for Fire Fighter Professional Qualifications7)
- Medical Response Technician
- Hazardous Materials First Responder (Awareness and Operational levels)
- Incident Command System (ICS) 100, 200, and 700
- Aircraft Rescue and Firefighting Course
- Confined Space Rescue (Awareness level)
- 2Q (prepares potential fire apparatus operators; designed by the State of Connecticut, Department of Motor Vehicles)
- Physical Fitness Training (begins the 2nd week of recruit training; includes daily basic stretching exercises, walking and an untimed 3 mile run. No documentation is maintained on the progression of the recruit fire fighter’s physical fitness level.)
Victim #1 had been with this department for approximately 16 years. Victim #1 was hired in July 1994 as a fire fighter after serving 5 years with another career fire department. He was promoted to the rank of lieutenant in February 2009. He held certifications in Fire Fighter I, Medical Response Technician, Hazardous Materials First Responder (Awareness and Operational levels), and Confined Space Awareness. He completed classes such as ICS 700, Fire Officer, Technical Rescue, and how to escape deadly situations inside burning buildings. He had also completed approximately 340 hours of documented yearly refresher training between 2004 and 2010; these hours included training on topics such as SCBA, safety, personal protective equipment (PPE), fire chemistry, and building construction.
Victim #2 had been with this department for approximately 2 years. Victim #2 was hired in December 2007 as a fire fighter with no prior firefighting experience. He held certifications in Fire Fighter I, Fire Fighter II, and Medical Response Technician. He completed classes such as ICS 100, 200, and 700a. He had also completed approximately 212 hours of documented yearly refresher training between 2009 and 2010; these hours included training on topics such as SCBA, safety, PPE, fire chemistry, and building construction.
The IC, at the time of the incident, had been with this department for approximately 33 years, holding the rank of a battalion chief for the past 5 years. Prior to becoming a battalion chief he held the rank of a captain (9 years), a lieutenant (6 years), pumper/engineer (2 months), and fire fighter (13 years). He held certifications in Fire Fighter I, Medical Response Technician, Hazardous Materials First Responder (Operational level), and Confined Space Awareness. He completed classes such as Engine and Aerial Company Operations, Marine Fire Fighting, RIT, and how to escape deadly situations inside burning buildings. He had also completed documented courses on ICS, strategies and tactics, and command officer training including ICS in 1994 (in house/National Fire Academy), ICS Training in 1997 (in house), Managing Company Tactical Operations Simulations in 2001 (state fire academy), Strategy and Tactics in 2004 (in house), IS-700 National Incident Management System in 2006 (Federal Emergency Management Agency (FEMA)/Emergency Management Institute), Chief Officers Training in 2006 (third party), ICS 300 in 2007 (FEMA), and ICS 400 in 2008 (state fire academy). Note: Hours associated with these courses were not included in the IC's training record. Also, this may not constitute a complete list of training completed on ICS, strategies and tactics, and command officer training for the IC. The IC had also completed approximately 136 hours of documented yearly refresher training between 2004 and 2010; these hours included training on topics such as SCBA, safety, hazardous materials, fire chemistry, and building construction.
Equipment and Personnel
1st Alarm Assignment:
- Engine 3 (E3) with an engineer, two fire fighters, and a captain
- Ladder 5 (L5) with an operator, two fire fighters, and a lieutenant (initial IC)
- Engine 4 (E4) with an engineer, two fire fighters, and a lieutenant
- Rescue 5 (R5) with a driver, three fire fighters (FF1, FF2, FF3), and a captain
- Ladder 11 (L11) with an operator, two fire fighters (FF4 and Victim #2) and a lieutenant (Victim #1)
- Engine 1 (E1) with an engineer, two fire fighters, and a captain
- Engine 7 (E7) as the initial RIT with an engineer, two fire fighters, and a lieutenant
- Battalion 1 (B1) with an aide (BA)
Note: See Diagram 1 for incident scene.
Additional units requested by the IC and/or dispatched to the scene:
- Deputy Chief (DC)
- Incident Safety Officer (ISO)
- Engine 12 (E12) to take over as RIT, with an engineer, two fire fighters, and a lieutenant
- Ambulance 7116 (A7116) with basic life support
- Ambulance 7110 (A7110) with basic life support
- Ambulance 7126 (A7126) with advanced life support
Personal Protective Equipment
It was reported to NIOSH investigators that both victims entered the structure wearing a full array of personal protective equipment (PPE) and clothing, consisting of turnout gear (coat and pants), helmet, Nomex® hood, gloves, boots, and a SCBA with an integrated personal alert safety system (PASS) device. According to fire fighters interviewed by NIOSH investigators and state police witness statements, Victim #1 was found to be cyanotic with his facepiece suctioned to his face. The fire fighter who discovered Victim #1 did not recall hearing his PASS device alarming. Victim #2 was discovered with his facepiece properly connected to his regulator, but not positioned on his face. Victim #2's PASS device was alarming when he was discovered in the house. Both sets of turnout gear had their heat-resistant outer shells, moisture barriers, and insulating thermal linings present during the incident and documented during the investigation.
Both victims were equipped with handheld radios. The state police investigator reported to NIOSH investigators, during his inspection, that Victim #1's radio was still operable, including the emergency button; however, the radio believed to be Victim #2's was found to be inoperable, even after the batteries were replaced. Note: NIOSH investigators cannot confirm if Victim #2's handheld radio was operable during the incident, but the radio that was designated for his position on the apparatus was keyed several times on the main dispatch channel while Victim #2 was being removed from the house.
The victims' SCBAs were secured and retained by the state police investigators. NIOSH investigators were able to photograph and document both SCBAs. Both SCBA cylinders were 30-minute, 4500-psi units. The SCBAs did not appear to be degraded from fire or heat but did shown signs of wear and tear. The SCBAs were manufactured in 2008 and found to be certified under the 2007 editions of NFPA 1981 Standard on Open-Circuit Self-Contained Breathing Apparatus (SCBA) for Emergency Services and NFPA 1982 Standard on Personal Alert Safety Systems.8,9 Victim #1's SCBA cylinder was manufactured in September 1998 and had a stamped hydrostatic test date on the cylinder of April 2003. Victim #2's SCBA cylinder was manufactured in January 2004 but did not visually appear to have a stamped hydrostatic test date on the cylinder. Therefore, due to applicable DOT standards, it appeared that both SCBA cylinders were due for repeat hydrostatic testing in 2008 and 2009 respectively (every 5 years). The victims' SCBAs were evaluated by the NIOSH National Personal Protective Technology Laboratory (NPPTL) to determine conformity to the NIOSH-approved configuration (see Appendix II). Information contained in the PASS device data logger was also downloaded with assistance from the SCBA manufacturer (see Appendix II). The victims' structural fire fighting gear and PPE were also examined by NPPTL to determine conformity to NFPA voluntary consensus standards. Note: This evaluation report will be added to this report as Appendix III, when completed. NIOSH investigators do not believe that the PPE had any direct contribution to the two fire fighter deaths.
The fire department maintains their SCBA equipment and compressed breathing air refill system. The SCBA maintenance shop has manufacturer-certified technicians who work on the SCBAs. In May 2010, the fire department's stationary and mobile air refill system was evaluated by a third party and found to be in compliance with NFPA 1989 Standard on Breathing Air Quality for Emergency Services Respiratory Protection, 2008 edition,10 and Compressed Gas Association G-7.1-2004 Grade E standards and regulations.
Structure
Built in the early 1900s, the two-and-half-story house (see Photo 1) was purchased approximately 4 years prior to the incident as a multifamily rental occupancy. One family lived in the 1st floor apartment (approx. 1,300 sq. ft.); a second family lived in the 2nd floor apartment (approx. 1,300 sq. ft.) (See Diagram 2), and the owner occupied the finished half-story or attic space (approx. 700 sq. ft.) (See Diagram 3). The house also contained an unfinished basement (approx. 1,300 sq. ft.). The common front entrance contained access to the 1st floor apartment and a private stairwell, located at the A/D corner of the house, which provided access to the 2nd floor apartment. The house also had a single rear-entry door that provided access to a stairwell that led up to the owner's apartment and had landings to access all the apartments from the rear. According to the owner of the house, smoke detectors were installed within the house about a year prior to the incident. These smoke detectors were installed in every bedroom, in each hallway, and in the stairwells. The house did not have an installed sprinkler system and had been inspected in accordance with Department of Housing and Urban Development Section 8a guidelines, according to the homeowner. The house was Type V wood frame construction, but, during the initial stages of the fire, was presumed by arriving fire fighters to be balloon-framed due to the era when it was constructed. State fire investigators were able to confirm Type V construction after closer inspection.

|
|
Photo 1. A-side of house during cleanup operations. |
The Office of the State Fire Marshal's building code compliance inspection showed that the house did not meet certain Connecticut Fire Safety Code requirements for this type of structure. NIOSH investigators do not believe that these non-compliance issues contributed to the deaths of the two fire fighters.
aFederal assistance provided by the United States Department of Housing and Urban Development. Under the program, the owner(s) of the property receive rent subsidies to assist qualified low-income tenants in paying their rent.
Weather Conditions
The weather on July 24, 2010, was abnormally warm for this area. Temperatures were in the 90s with a heat index above 100°F. Partly cloudy skies and approximate winds of 10 miles per hour from the southwest were observed. Research by the National Institute of Standards and Technology has shown wind speeds on the order of 10 to 20 mph (16 to 32 km/hr) are sufficient to create wind-driven fire conditions in a structure with an uncontrolled flow path.11 The weather caused heat exposure issues for fire fighters. The fire department does not have an emergency incident rehabilitation policy and several fire fighters received medical care on scene by EMS personnel, with some requiring transport to local hospitals for heat-related emergencies. Although water was provided to fire fighters during the incident, no rehab area was established.
Timeline
This timeline is provided to set out, to the extent possible, the sequence of events according to recorded and intelligible radio transmissions. Two channels were used during this incident: the main dispatch channel and channel 2 (fireground). Times are approximate and were obtained from review of the dispatch records, witness interviews, photographs of the scene, and other available information. Times have been rounded to the nearest minute. NIOSH investigators have attempted to include all intelligible radio transmissions, but some may be missing. This timeline is not intended, nor should it be used, as a formal record of events.
- 1544 Hours
E3 and L5 dispatched to a report of an elevator rescue. - 1546 Hours
While en route, E3 contacted the dispatcher on the main dispatch channel and advised them they needed to redirect all companies to a possible house fire. - 1547 Hours
L5 copied E3's transmission on the main dispatch channel and redirected to the possible house fire.
E3 advised the dispatcher, on the main dispatch channel, that they had a fire on the 2nd floor and that they did not have a hydrant. Note: It is unclear whether E3 established command, but L5 arrived just after E3 and established command. - 1548 Hours
E3, E4, E1, E7 as RIT, L11, L5, R5, and B1 were dispatched on the main dispatch channel to the house fire. - 1549 Hours
L5 arrived on scene and their officer stated over the main dispatch channel, "2½-story wood frame with heavy fire coming from the 2nd floor, Alpha/Bravo side, L5 is now command." - 1550 Hours
E7 en route. - 1551-1552 Hours
E4 arrived on scene and laid a supply line in from the hydrant.
Over the main dispatch channel, L5 officer (initial arriving IC) advised the dispatcher that the bulk of the fire was knocked down by E3 and the primary search was in progress.
Over the main dispatch channel, the dispatcher advised L11 and E7 which way they should approach the scene.
Over the main dispatch channel, L5 officer requested an ambulance for an injured fire fighter (ankle injury).
Over the main dispatch channel, B1 advised the dispatcher that he was on scene, and he confirmed the first report of heavy fire with the bulk of the fire knocked down. B1 then took command of the incident. - 1553 Hours
L11 arrived on scene.
E1 took an additional hydrant.
A7116 dispatched to the incident for an injured fire fighter. Note: Dispatch of A7116 was not part of the initial fire assignment. The 9-1-1 center contacted the EMS dispatch center via landline to request an ambulance for the injured fire fighter on scene after the request from the L5 officer. - 1554 Hours
Over the main dispatch channel, the BA advised the dispatcher that the command post would be in front of the fire building and tag collection would be at the command post. On channel 2, E4 officer asked E3 to charge the second hoseline. E7 (RIT) arrived on scene. - 1555 Hours
On channel 2, E4 officer asked E3 again to charge the second hoseline.
Over the main dispatch channel, the IC requested the dispatcher to have the safety officer respond to the incident.
IC checked on the status of the ambulance.
Fire dispatch advised the IC that the ambulance was en route. - 1556 Hours
E3 advised the IC (on the main dispatch channel) that he needed hooks on the 2nd floor in the room of origin; the IC acknowledged the request.
Over the main dispatch channel, IC advised all companies, “Channel 2 fireground, channel 2 fireground.” Note: Up to this point, companies on scene were operating on the main dispatch and channel 2. Fire dispatch assigned fireground operations to channel 2 for the incident. - 1557-1558 Hours
IC called L11 on channel 2.
IC (on the main dispatch channel) confirmed with the dispatcher who was RIT (which was E7) on scene and advised them that their equipment was available at the command post.
Victim#1 acknowledged the IC’s request for L11 on channel 2, but the IC did not respond.
E3 officer, who incorrectly identified himself as “E4,” called command on channel 2 and stated they had a slight extension into the A/B corner. Note: He was working overtime the day of the incident at the station that houses E3 and E4, which is also his normal duty station.
The IC copied the E3 officer’s transmission on channel 2 and asked him if he had enough hooks available; the E3 officer stated he did.
A7116 arrived on scene. - 1559 Hours
E3 officer on channel 2 advised the IC that they needed a hoseline to the 3rd floor because they could not reach it (fire extension) from the 2nd floor.
The IC acknowledged the E3 officer’s transmission on channel 2.
The IC, on channel 2, advised Victim #1 that E1 was bringing a hoseline to the 3rd floor.
Victim #1 acknowledged the IC’s transmission on channel 2 and advised, “A primary is in progress, which is negative; and, they are still checking for extension.”
The IC acknowledged Victim #1’s transmission. - 1600 Hours
Over the main dispatch channel, the ISO advised the dispatcher that he was responding (from home).
A7116 contacted EMS dispatch requesting a single ambulance to standby at the incident per the IC.
A7110 dispatched and en route to fire to standby.
On channel 2, the IC (at the command post) advised the E4 officer that he could see fire extending up the A/B corner. Note: NIOSH investigators were not sure if this transmission was meant for the E4 officer or the officer from E3 who identified himself as E4. At 1559 hours, the E3 officer advised the IC of the extension to the 3rd floor.
On channel 2, the E4 officer advised the IC that he was working on getting a line up to the 3rd floor. - 1601 Hours
Over the main dispatch channel, the dispatcher advised the IC that the ISO and DC were responding.
On channel 2, the L5 officer contacted “L5-Alpha” (believed to be L5’s aerial ladder) to assist in the bucket; L5-Alpha acknowledged the transmission. - 1602-1603 Hours
On channel 2, the IC contacted the L5 officer to verify whether he thought he could make the roof with L5.
On channel 2, the L5 officer stated that he was sending the driver down to talk to him.
R5 officer advised the IC on channel 2 that the primary was negative on the 2nd floor.
E4 attempted to contact L5 on channel 2, but was walked-on by R5-Alpha attempting to contact the R5 officer twice.
E3 officer advised L5 on channel 2 that they needed to overhaul the porch on the 2nd floor, but he did not think L5 could get to it.
L5 officer acknowledged E3 engineer’s transmission on channel 2. - 1604 Hours
DC en route to the incident.
Over channel 2, R5 called the IC three times (no response).
Over channel 2, the E4 officer called the E3 pump operator twice to shut the fog nozzle hoseline down; the E3 pump operator acknowledged.
Victim #1 called the IC twice on channel 2 (no response). - 1605 Hours
Over the main dispatch channel, the IC requested another RIT from the dispatcher.
On channel 2, R5-Alpha advised the R5 officer that the primary above the fire floor (2nd floor) was complete.
On channel 2, the R5 officer attempted to contact the IC (no response).
E4 officer advised the E3 pump operator to recharge the fog nozzle hoseline; the E3 pump operator acknowledged. - 1606-1607 Hours
A7110 arrived on scene.
E12 dispatched and responded as the RIT. Note: At 1604 hours, E12 was en route to the elevator rescue.
On channel 2, the IC advised Victim #1 that he was getting a second hoseline to the 3rd floor for him. The IC asked Victim #1, “What’s the situation up there?”
Victim #1 stated, “We got the line in place, it’s charged, we have extension into the attic space…”
The IC then asked for Victim #1 to verify “if” he already had a line in place, but there was no response.
A member of E4 advised the IC that they had, “…line in operation on the number three floor.”
A7116 en route to hospital with injured fire fighter. - 1608 Hours
R5 contacted the IC on channel 2 and advised him that they had one line in operation and he recommended that the roof be opened. Note: A Vibralert® could be heard alarming during his transmission.
IC advised R5 that they were preparing ground ladders to access the roof. - 1609 Hours
E12 (RIT) arrived on scene.
Over the main dispatch channel, IC advised E12 of where the command post and equipment were located.
Victim #1 called command on channel 2 (no response).
IC and E1 personnel had a conversation on channel 2 about supplying water to an additional unit on scene. Note: Victim #1 keyed his radio prior to and just after this conversation, but no transmissions occurred. - 1610-1612 Hours
L5 officer called R5 on the main dispatch channel (no response).
On the main dispatch channel, the BA advised L5 and all companies to switch to channel 2.
E3 personnel contacted the IC on channel 2 and advised him that they might be able to open it (the roof) from the 2nd floor if they had hooks.
The IC called Victim #1 on channel 2 and was acknowledged, but no further transmissions occurred.
E4 (officer) called the nozzle man down to the 3rd floor. Note: At this point, the nozzle man may be the driver of R5.
L5 officer contacted R5 on channel 2.
R5 officer advised the L5 officer that they were operating on the 3rd floor and could not open the roof from there.
The IC attempted to contact Victim #1 on channel 2 (no response).
DC arrived on scene.
ISO arrived on scene. - 1613 Hours (1st Mayday Call)
On channel 2, FF2 called R5 (no response). He then called L11 (no response).
L5 officer advised L5-Alpha/Bravo to “come on down.” Note: L5-Alpha/Bravo is believed to be on the roof.
On channel 2, Victim #1 stated, “Mayday-Mayday-Mayday, we’re trapped on the rear stairs.” Note: This transmission was very quick lasting only 3 seconds. A Vibralert, presumed to be Victim’s #1, can be heard alarming during his transmission. Victim #1’s Mayday call was not acknowledged over the radio.
FF2 advised L11 on channel 2, “…fire below you, B-side.”
E1 personnel had a brief conversation on channel 2 regarding water supply.
The IC called L11 on channel 2 (no response).
An unknown fire fighter’s transmission is heard stating, “Negative on that opening, negative on that roof opening.”
The IC called L11 on channel 2 again (no response). - 1614 Hours
The IC called E1 on channel 2 (no response).
The IC called the L11 officer (Victim #1) on channel 2 (no response). - 1615 Hours
On channel 2, the IC stated, "Command to all companies on the 3rd floor, vacate the 3rd floor; I repeat, command to L11 and E1, vacate the 3rd floor." - 1616-1619 Hours 2nd Mayday Call)
The IC attempted to contact L11 again on channel 2 (no response).
The IC, on channel 2, then stated, “Command to E1.”
(1616.50 hours) On channel 2, FF2 stated, “Mayday, Mayday…Rescue 5 Bravo command we have a downed fire fighter rear steps. Mayday-Mayday-Mayday fire fighter down rear steps, 2nd floor.”
IC called L11 again on channel 2 (no response).
FF4 on channel 2 stated, “Ladder 11 irons to Ladder 11” (no response). Note: An apparatus air horn is heard sounding in the background of this transmission.
FF2 on channel 2 stated, “Rescue 5 Bravo command, Rescue 5 Bravo command we need help 2nd floor, send the RIT, we need fresh bodies.” Note: No audio transmissions or emergency tones are heard on channel 2 or the main dispatch channel advising that the Mayday call had been acknowledged.
DC contacted the IC on channel 2 to have him send the RIT to the rear stairs; the IC acknowledged. Note: The RIT may have already been advancing up the rear stairs, but they ran into difficulty accessing the 2nd floor landing off the rear stairs because a charged hoseline was against the closed door.
Dispatch attempted to contact command on channel 2 (no response).
The IC called L11 again on channel 2 (no response).
The DC contacted the IC requesting the ambulance on scene to come to the rear of the house.
Victim #1 was extricated out the rear of the house. - 1620 Hours
A7110 began medical care for the downed fire fighter (Victim #1).
Over the main dispatch channel, the BA requested an advanced life support ambulance to the fire scene.
A7126 was dispatched to intercept A7110 at the fire scene to provide advanced life support.
(~1620.35 Hours) The following transmission is heard on channel 2, “…Ladder 11 ‘mayday’ (very quick transmission)…Ladder 11 (unintelligible word(s)).” Note: The dispatch caller ID for this radio is designated as “L-11 FF3,” which was assigned to the fire fighter (designated as FF4 for this report) who later finds Victim #2 (see below 1624 hours). FF4 had not found Victim #2 at the time of this transmission.
On channel 2, FF4 stated, “Ladder 11 irons to Ladder 11 can” (no response). Note: “Ladder 11 can” was Victim #2’s designation that shift. - 1621 Hours
A7126 en route to fire scene. - 1622 Hours
On channel 2, the ISO advised the IC that the fire fighter (Victim #1) was removed and they needed to do a roll call for everyone on scene.
On channel 2, the IC advised all company officers that the “incident is taking a PAR” (personnel accountability report).
Officers began calling in their respective PARs - 1624 Hours (3rd and 4th mayday Calls)
FF4 on channel 2 stated, "Mayday-Mayday, I have a fire fighter trapped on the 3rd floor, Mayday-Mayday-Mayday 3rd floor." Note: This Mayday is for Victim #2. A PASS device is heard alarming during FF4's transmission.
On channel 2, the IC stated, “This is command to all companies, vacate the building, I report, command to all companies, vacate the building.”
FF4 on channel 2 stated again, “Mayday-Mayday-Mayday, I’ve got another fire fighter down, another one, 3rd floor, hurry!” - 1625 Hours
Over channel 2, the dispatcher stated, "For a Mayday," and activated the emergency evacuation tones. Note: It is unknown why the evacuation tones were sounded instead of the Mayday tones. Their evacuation tone is an alternating, high-low sound, similar to a European siren. Their Mayday tone is a rapid, high to low pitch, chirping sound. This was dispatch's first acknowledgement of a Mayday over the radio. No further radio traffic regarding the Mayday was provided by the dispatcher following the tone activation on channel 2.
Over the main dispatch channel, the dispatcher stated, “For a Mayday,” and activated the emergency evacuation tones as well. No further radio traffic regarding the Mayday was provided by the dispatcher following the tone activation on the main dispatch channel. - 1626 Hours
The IC contacted the DC on channel 2. DC acknowledged with no further traffic from the IC.
The IC on channel 2 again advised all companies to vacate the building.
The dispatcher then activated the emergency tones on channel 2 and the main dispatch channel, and stated, “All companies per command vacate the building, all companies vacate the building.” - 1627 Hours
The ISO contacted the IC on channel 2 and stated, "We need to make contact with that Mayday, we need more information, we have not heard from them since the initial call."
On channel 2, the IC stated, “Command to company declaring a Mayday; I repeat, command to the company declaring a Mayday sound off, sound off.”
A fire fighter from the RIT advised the IC on channel 2 that they were moving the fire fighter off the 3rd floor.
On channel 2, the dispatcher advised the IC that the Mayday call was for the 3rd floor.
A7126 arrived at the fire scene. - 1628 Hours
RIT advised the IC that they have the fire fighter (Victim #2) on the 3rd floor and will be bringing him down the rear stairs from the 3rd floor. - 1630 Hours
A7110 en route to the hospital with Victim #1 without assistance from A7126. - 1632 Hours
ISO asked for a progress report from the RIT on the Mayday.
RIT replied, “Coming down…3rd floor.”
ISO asked RIT to repeat their traffic.
A radio was keyed, but there was no transmission. - 1634 Hours
RIT personnel advised the IC that they had the fire fighter (Victim #2) down to the 2nd floor landing. - 1640 Hours
A7110 arrived at local hospital with Victim #1. - 1643 Hours
A7126 began medical care on second downed fire fighter (Victim #2). Note: This time was taken from Victim #2's patient care report and may not be accurate. - 1703 Hours
A7126 arrived at local hospital with Victim #2.
Investigation
On Saturday, July 24, 2010, at 1544 hours, E3 and L5 were dispatched for a reported elevator rescue. While en route to this incident, personnel on E3 noticed smoke coming from a residential side street and immediately notified dispatch. E3 and L5 diverted to the residential side street. E3 arrived on scene first to find fire showing from the 2nd floor B-side window and smoke showing from the 2nd floor A-side windows (both windows located at the A/B corner). E3 was not able to lay a line into the scene because when they turned onto the residential side street they were unsure of which house was actually on fire. E3 pulled just past the house to allow room for L5 (see Diagram 1). The E3 officer exited E3 and quickly performed a size-up of the fire. The E3 officer felt that the fire could be quickly contained with the 500 gallons of water carried on E3 and the additional personnel arriving on L5. The E3 hydrant man and nozzle man exited the engine and pulled a dry 250-ft, 1¾-inch pre-connected attack line to the 2nd floor landing (see Diagram 4). The E3 officer assisted them in flaking the hose out before joining them on the 2nd floor landing. While this was taking place, L5 arrived on scene, gave a size-up over the radio, and established command for the incident. The E3 nozzle man opened the bail and had no pressure. The E3 officer exited the house and removed kinks in the hoseline with assistance from L5 personnel. The E3 officer returned to the house and noticed that his nozzle man was coming down the 2nd floor stairs in pain. The E3 officer stayed with his hydrant man (who was now on the nozzle) and quickly extinguished the room and contents fire on the 2nd floor. The L5 officer called for an ambulance and took care of the injured fire fighter who apparently had sustained an ankle injury while advancing the charged hoseline toward the fire room.
While E3 operated in the fire room, E4 arrived on scene and laid a 5-inch supply line into E3. R5, L11, L1, E7 (RIT), and BC had arrived or were also arriving on scene. Two L5 fire fighters followed shortly by two R5 fire fighters (driver and FF1) and R5's officer entered the house following E3's hoseline to the 2nd floor, and the L5 operator raised the ladder to the A/B corner of the house. The two L5 fire fighters performed a primary search of the 2nd floor and opened windows as they progressed to the rear stairwell. This stairwell provided them access to the 3rd floor so that they could continue their primary search and check for extension above the fire room. The two L5 fire fighters were met with light smoke conditions and hot temperatures when they reached the 3rd floor (prior to any windows being opened). These two L5 fire fighters recalled radio transmissions from the L5 officer regarding the fire being knocked down and the BC arriving on scene and taking command. As they were walking to pull the baseboards below the windows in the front room (the front room was at the A/B corner, directly above the fire room), personnel from R5 (FF2/FF3) and L11 (Victims #1 and #2 and FF4) entered the 3rd floor, and they assisted L5 with opening windows on the B- and D-sides of the 3rd floor. Note: Victim #1 received face-to-face orders from the IC to check on extension and ventilation on the 3rd floor. L11 personnel walked through the 1st floor apartment to the rear stairwell, not on air, and then walked up to the 3rd floor where they had to go on air. Victim #2 assisted with pulling the baseboards in the front room while FF2 and FF3 used a thermal imaging camera to check for hot spots and extension. Note: FF3 remembered speaking with Victim #1 in the kitchen area on the 3rd floor regarding the hot spots viewed on the thermal imaging camera and recalled hearing Victim #1 relaying the information to command. Opening the windows on the 3rd floor allowed cross ventilation, which quickly increased visibility on the 3rd floor, but the room was still extremely hot.
The E4 nozzle man and officer pulled the second hoseline from E3 to back-up E3 personnel working on the fire floor. This second hoseline was a 200-ft, 1¾-inch pre-connect with a fog nozzle. The R5 officer, who was paired up with FF1, left the driver of R5 to pull ceilings in the fire room. The R5 officer and FF1 went up to the 3rd floor to check on conditions. The R5 officer recalled bumping into Victims #1 and #2 and FF4 in the front room of the 3rd floor. FF1 then had to exit the 3rd floor because his Vibralert was alarming. Note: At this time, smoke conditions varied and personnel operating on the 3rd floor may not have been on air. The R5 officer and Victim #1 had a conversation about the thermal imaging camera (TIC) showing how hot the walls were and how they needed a hoseline. The R5 officer and Victim #1 advised all personnel on the 3rd floor not to open the walls or ceiling until they had a charged hoseline in place. Victim #1 had previously requested a hoseline. Note: At this point, E7/E1 may have been tasked by the IC with preparing an additional hoseline for the interior, thus removing E7 from the role of RIT. The IC then notified dispatch that he needed an additional engine company for RIT.
Once the E4 crew made it up to the 2nd floor it was determined that the hoseline was no longer needed in the fire room and the hoseline was redirected to the 3rd floor. This second hoseline only made it to the base of the stairwell that led to the 3rd floor. The E4 officer called for a "spare flake" and the E4 hydrant man and driver retrieved a 100-ft section of hose. This section of hose contained a smooth bore nozzle and a gated wye valve. When they returned with the extra section, the E4 officer ordered the E3 pump operator to shut down his hoseline. The E4 officer then left his crew at the base of the stairs to check conditions on the 3rd floor. The E4 nozzle man, hydrant man, and driver disconnected the fog nozzle from the second hoseline and connected the extra section with the smooth bore nozzle. The E4 officer recalled moderate smoke conditions, which were banked down to about chin level on the 3rd floor. He recalled moving furniture that was located above the fire room with personnel from R5 (FF2 and FF3). Note: The E4 officer does not recall the whereabouts of Victims #1 and #2. The two L5 fire fighters, who were operating on the 3rd floor, were ordered down (by the L5 officer) to begin roof ventilation operations. Note: The IC had observed smoke conditions on the B-side suggesting the roof needed to be vented. The E4 officer returned to the 2nd floor to assist the nozzle man and hydrant man in flaking and removing kinks from the hoseline before it was advanced to the 3rd floor. While they advanced the dry hoseline up to the 3rd floor, they were passed by R5 personnel (FF2 and FF3 and shortly after, possibly by the R5 officer), who were all exiting to get new air bottles. Note: While FF2 and FF3 were walking through the 2nd floor to leave, the officer of E3 asked them to assist with checking extension in the fire room. Both were out of air, but many fire fighters interviewed by NIOSH investigators stated that conditions on the 2nd floor did not require them to be on air. The E4 crew advanced the hoseline approximately 5-7 feet into the 3rd floor with assistance from FF4 and the E1 officer, and then the E4 officer called for the hoseline to be charged. The E4 officer recalled thick, black smoke banked down to just above floor level and the sound of fire around him (no visible fire) just prior to personnel opening the ceiling and walls. Personnel from R5 (driver) and possibly L11 continued opening the ceilings, dropping sheet rock around the hose crew. Note: The E4 hydrant man recalled fire fighters coming up the stairs as they were operating their hoseline. NIOSH investigators believe this may have been the R5 officer (returning with a fresh air bottle) and possibly personnel from E1 and/or E7.
The E4 nozzle man did not recall seeing any fire, but a lot of heat was released when the ceiling was opened. Thick black smoke was also released and pushed down to floor level. E4 continued to flow water on the 3rd floor when their nozzle man's Vibralert began to alarm. He handed the nozzle over to the R5 driver and followed the hoseline out. The E4 officer and hydrant man remained on the hoseline. The R5 officer remembered that when he returned to the 3rd floor, the hoseline stretched by E4 could not reach the A-side of the house, black smoke had completely obscured visibility, and the heat on the 3rd floor had intensified. The R5 officer recalled speaking to someone about getting more lines into the 3rd floor. Note: The R5 officer does not recall seeing Victims #1 or #2 on the 3rd floor at that time, and FF4 may have been in the process of exiting the 3rd floor to change his air bottle. Shortly following this, the Vibralert for both the E4 officer and hydrant man started alarming. The E4 officer spoke to two unknown fire fighters and advised them to take the hoseline and back up the fire fighter on the nozzle (driver of R5). The E4 officer and hydrant man exited the house to retrieve fresh air bottles. At some point, the R5 driver left the nozzle on the 3rd floor because his Vibralert was also alarming. He stated that he told 1 or 2 fire fighters that he was leaving the 3rd floor. Note: NIOSH investigators cannot confirm who he spoke to. The R5 officer exited the 3rd floor and saw a dry hoseline being flaked out on the 2nd floor, with assistance from FF1. Note: E7/E1 personnel were working on getting this hoseline into operation. The R5 officer exited the house and went to the command post to talk with the IC about how bad conditions were. It is unclear if the R5 officer walked to the A-side of the 3rd floor in the area of the front room prior to leaving the 3rd floor. NIOSH investigators cannot account for the exact location of Victims #1 or #2 on the 3rd floor. An E1 fire fighter stated that he operated a hoseline on the 3rd floor by himself (possibly after the R5 driver left) and heard a loud noise, immediately closed the nozzle, and yelled out to see if someone was there. He then left the 3rd floor.
NIOSH investigators believe that Victim #1 and Victim #2 were alone on the 3rd floor when Victim #1 transmitted, "Mayday-Mayday-Mayday, we're trapped on the rear stairs." His Mayday, lasting only 3 seconds, was never acknowledged over the radio by the 911 dispatcher(s), the IC, or other personnel on scene. While this was occurring, the dry, second hoseline was placed over the 3rd floor stairwell wall by an E1 fire fighter. FF2, still with FF3 in the fire room, radioed Victim #1 (directly following Victim #1's Mayday transmission) to let him know that the fire was below him, B-side, but he got no response, so he decided to walk back through the house to the rear stairwell. FF3 exited the house to retrieve a new air bottle. The IC was also attempting to call personnel who were last known to be on the 3rd floor, with no response, which ultimately led to the IC ordering an evacuation. The E12 officer (who took over RIT), the on-call DC, and the ISO who all had just arrived on scene moments before Victim #1's Mayday all stated they heard what they thought was a faint or muffled Mayday over the radio. The DC walked from his vehicle over to the command post and spoke to the IC and BA regarding the possible Mayday call; they were both unaware of the transmission. The E12 officer also approached the command post and spoke to the IC and DC regarding the Mayday. The IC was unaware of the Mayday transmission and the DC said he wasn't sure if he heard one. There was no acknowledgement for a Mayday over the radio from the 911 dispatcher(s). Note: There was no attempt to verify whether a Mayday was transmitted over the radio. The DC and E12 personnel (RIT) then proceeded to walk down the B-side of the house.
While this was occurring, FF1, who was still on the 2nd floor landing, followed the charged hoseline from E4 to the 3rd floor. He stopped short of the 3rd floor door because he saw the figure of a fire fighter coming toward him in a crouched position. This fire fighter, later identified as Victim #1, leapt from the 3rd floor onto the stairs going down to the 2nd floor, landing on a knee wall separating the ascending and descending sides of the stairwell. FF1 immediately grabbed Victim #1 by his SCBA harness and assisted him over the wall onto the descending stairs. FF1 reported that Victim #1 landed on his feet, facing the sub landing. Victim #1 then turned around and sat down on the stairs, facing the door leading out to the 2nd floor. FF1 looked at him for a few seconds and noticed that his facepiece was still on and no alarms were alarming. FF1 did not feel anything was out of the ordinary so he continued to the 3rd floor. FF1 continued to follow the charged hoseline to the 3rd floor, wondering why the roof had not yet been opened. Note: Once L5 personnel ascended the roof via a 28-ft ladder positioned on the B-side of the house, they were unable to operate the saw due to heavy smoke conditions emitting from the roof and eaves. FF1 stated that the smoke was extremely black and thick. He told NIOSH investigators that he came upon a fire fighter on the hoseline. FF1 did not have a conversation with this fire fighter; he thought maybe he was on the nozzle or backing the nozzle man up because he heard water spraying toward the A-side (water was being sprayed from the 2nd floor). Note: NIOSH investigators believe the fire fighter that FF1 came upon was Victim #2. NIOSH investigators cannot place any other fire fighters on the 3rd floor at this time. FF1 does not recall how this fire fighter was positioned. FF1 then heard the IC call over the radio for the building to be evacuated. FF1 immediately turned around and followed the hoseline out.
While descending the stairs, FF1 came upon Victim #1 still sitting in the same position he had left him, with his facepiece on and no alarms sounding. FF1 nudged Victim #1 and told him they had to evacuate the house. Victim #1 then slumped over. FF1 quickly grabbed him and began pulling him down the stairs to the 2nd floor. Personnel from E7 and E1, who were working on the 2nd floor just off the stairs, quickly assisted FF1. FF2 got to the rear of the 2nd floor and saw that Victim #1 was unconscious and being brought down the stairs by FF1 and personnel from E7 and E1. FF2 immediately called the Mayday for Victim #1. Note: Approximately, 3 minutes and 30 seconds passed from the time Victim #1 called his Mayday until FF2 called the Mayday for Victim #1. The RIT (E12) was heading into the backyard when they heard this Mayday transmitted. The DC, who also heard FF2's Mayday call, later alerted the IC to send the RIT to the backyard, but they were already heading up the rear stairs. The IC stated to NIOSH investigators that he did hear this Mayday transmission and he proceeded to the backyard. Dispatch did not acknowledge this Mayday call over the radio, nor were they advised of a Mayday occurring at the incident. The IC was still attempting to contact L11 (Victim #1) after FF2 transmitted the Mayday. FF4 returned to the 2nd floor via the A-side stairwell to see Victim #1 being cared for. FF4, realizing Victim #2 was not with Victim #1, attempted to contact Victim #2 with no response. The RIT immediately assisted with getting Victim #1 down the stairs to receive medical care. Note: The IC arrived at the backyard when Victim #1 was being carried from the house, so he ran back to the front of the house and alerted EMS personnel on scene. Once Victim #1 was outside the house, CPR was immediately initiated and an automated external defibrillator was attached. Only basic life support measures were initiated by EMS personnel on scene due to their level of training. FF4 exited out the rear stairwell and began looking for Victim #2 asking several fire fighters if they had seen Victim #2, but no one was sure where he was. It is believed at this point that FF4 made the decision to re-enter the house and search for Victim #2. The ISO advised the IC that they needed a PAR and the IC advised personnel over the radio. At this time, the ISO was requesting a PAR and the IC was notifying personnel that they needed to evacuate the house.
FF4 entered the rear stairwell and went to the 3rd floor (it is unclear if any personnel followed him into the house). He followed a hoseline into the 3rd floor and found Victim #2 apparently lodged between a wall and a piece of furniture (see Diagram 5). Victim #2's PASS device and indicator lights were alarming; he did not have his facepiece on. FF4 stated that he called a Mayday for Victim #2 and then heard evacuation tones over the radio and then air horns from an apparatus. He transmitted a second Mayday because the first one was not acknowledged by dispatch or the IC. Dispatch acknowledged the second Mayday for Victim #2 and set off the evacuation tones (not the Mayday tones), but no further radio traffic from dispatch or the IC confirmed the specifics of the Mayday. The ISO radioed the IC and advised him that they needed additional information on the Mayday that was just called. The RIT and other fire fighters located in the backyard were working on getting to Victim #2 and getting him off the 3rd floor and down the stairs. Many fire fighters at this point had gone through one or even two bottles and were exhausted. The RIT provided the IC with updates on their progress. The RIT recalled Victim #2 being caught between a sofa and a wall on his back with his arms out from his body when they found him (see Diagram 5). Victim #2 may have also been entangled in a hoseline. The RIT removed Victim #2 from the house, CPR was initiated and an automated external defibrillator was attached. Both victims were taken to local hospitals where they were pronounced dead.
NIOSH investigators can only speculate on what occurred on the 3rd floor that led Victim #1 to transmit a Mayday. FF1 stated to NIOSH investigators that he never heard the Mayday transmitted by Victim #1 and believed there were no causes for alarm when he saw Victim #1 exit the 3rd floor. FF1 does not recall hearing Victim #1's PASS device when he exited the 3rd floor or after he slumped over on the stairs. The victims' air packs were designed to go into pre-alarm within 20 seconds (can shake to reset) and then full alarm at 30 seconds (reset button must be used). Victim #1's facepiece was suctioned to his face when he was found. The question still remains why Victim #1 never removed his regulator or facepiece when he sat down on the stairs. It is unknown why Victim #2's facepiece was not positioned on his face. Both SCBA cylinders were empty upon inspection by state police investigators.
Fire Behavior
The room and contents fire was determined to have originated in a bedroom on the 2nd floor, A/B corner; it was quickly knocked down by E3 (see Photo 2). It is believed that the fire got into the eves when it was lapping out the A/B corner windows, and then spread within the large void spaces in the ceiling and walls of the 3rd floor. The fire was situated toward the A/B corner of the 3rd floor, but the open void areas allowed smoke to accumulate within the ceilings and walls before they were opened.

|
|
Photo 2. Remnants of a mattress and box springs within the room of origin on the 2nd floor. |
Operating on the 3rd floor at varying times were members from L5, R5, L11, E4, and E7. Initially, light-to-moderate smoke conditions were observed on the 3rd floor, depending on how close fire fighters were to the A-side of the 3rd floor. Fire fighters recalled the 3rd floor being very hot. TICs used by different individuals on the 3rd floor showed the room to be hot on the A-side and ceiling. Windows on the A-, B-, and D-sides were opened, allowing most of the smoke to self ventilate. Light smoke remained within the 3rd floor, with good visibility. Extension was checked around A- and B-side baseboards. Some fire fighters recall Victim #1 telling them the fire was in the ceiling and possibly the walls, and to not open those areas until a hoseline was in place. Even after providing horizontal ventilation on the 3rd floor, smoke conditions worsened, banking down to fire fighters' chin levels and becoming denser. While waiting for the hoseline, L5 members were reassigned by the IC to ventilate the roof to provide additional relief to the 3rd floor. The IC reported to NIOSH investigators that he ordered the roof vented because he saw smoke pushing out the B-side windows. Personnel from E4 advanced the charged hoseline to the 3rd floor, allowing the ceilings and walls to be opened. A mixture of thick, brown/black smoke quickly filled the room, reducing visibility. Photos 3-10 show conditions at the scene leading up to the first Mayday and then during the second Mayday.

|
Photo 3. Initial conditions observed when the BC arrived on scene at approximately 1551 hours. Note: Fire was under control on the 2nd floor and fire fighters were checking for extension. White-to-gray smoke can be seen flowing in the direction of right to left from the gables. The A-side window on the 3rd floor had been opened for ventilation (unsure at what stage of the fire or by whom). |
 |
Photo 4. Conditions observed at 1608 hours by an off-duty fire fighter. Note: Smoke had changed to gray and brown in color and was emitting from the eaves and A- and D-side windows which were manually opened by personnel working on the 3rd floor. A hoseline was being stretched to the 3rd floor. |

|
Photo 5.Conditions at approximately 1609 hours. Note: L5 personnel were preparing to ascend the ladder placed on the B-side of the house. The IC (white helmet) is observing the scene. Smoke seen coming from the 3rd floor B-side double window and pushing from the eaves. At this time, ceiling and walls were likely being opened on the 3rd floor, and water would have been available. |
 |
Photo 6. Conditions at approximately 1611 hours. Note: L5 personnel were ascending the roof from the ground ladder on the B-side. Smoke color was still gray to brown in color and was becoming denser. Personnel were still working on the 3rd floor. Wind direction was right to left. |
 |
Photo 7. Conditions at approximately 1613 hours. Note: L5 personnel were on the peak of the roof and having difficulty starting the roof saw. Smoke was denser than before and pushing from the roof and eaves. The fire fighters were unable to vent the roof. NIOSH investigators believe that Victim #1 transmitted his Mayday about this time. |

|
Photo 8. Conditions at approximately 1616 hours. Note: View from the A/D corner, scene conditions very close to when FF2 discovered FF1 pulling Victim #1 off the 3rd floor stairs. White and gray smoke can be seen flowing from the A-side window and eaves while brown smoke flowed from the D-side window. |
 |
Photo 9. Mayday for Victim #1, called by FF2. Note: RIT personnel from E12 are seen heading to the rear of the house. L5 personnel were descending the roof via the B-side ground ladder. Fire is seen burning along the roof line above the A/B corner. Gray, dense smoke was flowing from the 3rd floor B-side double window and A-side window. |
 |
Photo 10. Fire vented through the roof. Note: NIOSH investigators believe this photo shows conditions very close to the time that the Mayday was called for Victim #2 by FF4. Wind was pushing the smoke plume from right to left. |
Contributing Factors
Occupational injuries and fatalities are often the result of one or more contributing factors or key events in a larger sequence of events that ultimately result in the injury or fatality. NIOSH investigators identified the following items as key contributing factors in this incident that ultimately led to the fatalities:
- Failure to effectively monitor and respond to Mayday transmissions
- Less than effective Mayday procedures and training
- Inadequate air management
- Removal and/or dislodgement of self-contained breathing apparatus (SCBA) facepiece
- Incident safety officer (ISO) and rapid intervention team (RIT) not readily available on scene
- Possible underlying medical condition(s) (coronary artery disease)
- Command, control, and accountability.
Cause of Death and Injuries
Autopsies were conducted by the state medical examiner on both victims. Significant findings for Victim #1 included a focally severe occlusive coronary atherosclerosis (≥ 95% blockage) of his right coronary artery, 4 centimeters distal from its origin, and a carboxyhemoglobin (COHb) level of 4%, suggesting only minimal carbon monoxide exposure. His cause of death was listed as "asphyxia associated with smoke inhalation and exposure to fire." Significant autopsy findings for Victim #2 include patchy severe atherosclerosis, producing approximately 80% occlusion of the left anterior descending coronary artery and up to 60% occlusion of the mid-portion of the right coronary artery, and a COHb level of 44% (a level consistent with fatal carbon monoxide poisoning). His cause of death was listed as "smoke inhalation with other significant condition(s) of coronary atherosclerosis."
In addition to the deaths of the two fire fighters, the fire fighter from E3 suffered a broken ankle while advancing the hoseline, and numerous fire fighters suffered heat-related illnesses with 5 or 6 requiring transport to local hospitals.
Recommendations
Recommendation #1: Fire departments and dispatch centers should ensure that radio transmissions are effectively monitored and quickly acted upon, especially when a Mayday is called.
Discussion: Fireground communications can become very hectic and confusing when a fire fighter is in distress, becomes lost, or is trapped. Fire departments and dispatch centers need to be able to effectively monitor radio transmissions (e.g., Maydays) while on the fireground and within a dispatch center. A Mayday procedure can outline the fireground response plan and duties of fire fighters, officers, the dispatch center, and the IC. This will help reduce any confusion during the Mayday.
The term "Mayday" is the international distress signal. Fire fighters must act promptly when they become lost, disoriented, injured, low on air, or trapped.12-17 They should announce "Mayday-Mayday-Mayday" over the radio and manually activate their PASS device. A transmission of the Mayday situation should be followed by the last known location of the fire fighter, and if able, the individual's identifier, such as "E3 pump." A crew member who suspects a fire fighter(s) is in trouble or missing should quickly try to communicate with the fire fighter(s) via radio and, if unsuccessful, initiate a Mayday providing relevant information.
An emergency radio transmission reporting a "Mayday" is the highest priority transmission that may occur at any incident and should receive precedence from dispatch, the IC, and other units operating at the incident. When this emergency traffic is initiated, all other radio traffic should stop to clear the channel and allow the message to be heard. Mayday transmissions must always be acknowledged and immediate action taken. The IC must either personally handle the situation or designate another officer to do so. Part of "handling" a Mayday is to communicate with the fire fighter(s) in distress and with any other fire fighters or officers involved. The sooner the IC is notified and a RIT is activated, the greater the chance of the fire fighter being rescued. If there is any question that a Mayday may have been transmitted and heard by someone (not all), it should also receive priority in verifying if it were a Mayday transmission. The IC should be made aware of this immediately, so that he can attempt to contact the potential individual who transmitted the Mayday or contact dispatch to verify the transmission. A possible Mayday transmission should never be overlooked.
During this incident, the IC had to monitor two different radio channels by using two different handheld radios. His BA also assisted in monitoring the two radio channels. At times, radio transmissions on one channel were missed or unanswered because the IC was transmitting on the opposite channel. The DC and officer of E12 all thought they heard what sounded like a Mayday (transmitted from Victim #1), and a face to face discussion occurred among them and the IC, but this possible Mayday transmission was not confirmed with dispatch, nor, at the time, the unknown fire fighter that transmitted it.
This fire department had established a Mayday procedure within the department that was practiced routinely with the communications center, but this routine radio check did not test fire fighter or dispatcher competencies in the Mayday procedure, or the ability of an IC to manage a Mayday incident. Weekly, dispatch would select a company and radio channel to practice the Mayday procedure. The dispatchers followed a procedure at a scheduled day and time, instead of having an unannounced Mayday called. The challenge for fire departments is providing realistic, safe training that accurately simulates fire conditions, but it is absolutely necessary that the Mayday training place fire fighters in positions that closely simulate an actual fire to realistically exercise one's Mayday skills.17 In this incident, Mayday transmissions were missed and not acknowledged. It is not known why the dispatch center did not hear or acknowledge the Maydays or why the Mayday tone was not used appropriately.
Fire departments should be aware of the recently released 2010 International Association of Fire Chiefs' (IAFC) Rules of Engagement (ROE) of Structural Firefighting.18 These guidelines recommend that fire fighters constantly monitor fireground communications for critical radio reports and declare a Mayday as soon as they are in danger. Although not addressed by the IAFC ROE, ICs and dispatch centers should also be constantly monitoring fireground communications for critical radio reports.
Also, the IAFF Fire Ground Survival program was developed to ensure that training for Mayday prevention and Mayday operations are consistent between all fire fighters, company officers, and chief officers. 17
Recommendation #2: Fire departments should ensure that Mayday training program(s) and department procedures adequately prepare fire fighters to call a Mayday.
Discussion: The first and foremost priority for fire fighter safety is not getting oneself into a situation that could potentially cause injury or death. The fire fighter needs to maintain situational awareness at all times while operating on the fireground. Knowledge and skill training on how to prevent a Mayday situation or how to call a Mayday should begin and be mastered before a fire fighter engages in fireground activities or other immediately dangerous to life and health (IDLH) environments. Beginner fire fighter training programs should include training on such topics as: air management; familiarity with an SCBA, a radio, or PPE; crew integrity; reading smoke, fire dynamics and behavior; entanglement hazards; building construction, and signs of pending structural collapse. If a fire fighter does find themself in a questionable position (dangerous or not), they must be able to recognize this and be trained on procedures for when and how a Mayday should be called. A fire fighter's knowledge, skill, and ability to declare a Mayday must be at the mastery level of performance. This performance level should be maintained throughout their career through training offered more frequently then annually.17
In this incident, the fire department's Mayday SOP stated, "Whenever any member is in a situation that they believe to be life-threatening and unable to escape from, they will transmit a Mayday." Fire departments need to understand that each fire fighter may have a different interpretation of what is life-threatening. The ability of a fire fighter to call a Mayday is a complicated behavior that includes the affective, cognitive, and psychomotor domains of learning and performance.19 Any delay in calling a Mayday reduces the chance of survival and increases the risk to other fire fighters trying to rescue the downed fire fighter. This incident illustrates the need for fire fighters to be given specific Mayday procedures for when a Mayday must be called.
There are no rules on when a fire fighter must call a Mayday, and Mayday training is not included in NFPA fire fighter 1 or 2 standards.7 It is up to each authority having jurisdiction to develop rules and performance standards for a fire fighter to call a Mayday. The National Fire Academy Mayday courses present specific Mayday parameters or rules for when a fire fighter must call a Mayday. The courses may help fire departments in developing and teaching Mayday procedures for fire fighters.
The National Fire Academy has two courses addressing the fire fighter Mayday Doctrine, Q133 Firefighter Safety: Calling the Mayday, which is a 2-hour program covering the cognitive and affective learning domain of the fire fighter Mayday Doctrine; and, H134 Calling the Mayday: Hands-on Training which is an 8-hour course that covers the psychomotor learning domain of the fire fighter Mayday Doctrine. These courses are based on the military methodology used to develop and teach fighter pilots ejection doctrine. A training CD is available to fire departments free of charge from the U.S. Fire Administration Publications office. 19-20
Also, the IAFF Fire Ground Survival program is another resource fire departments can use and was developed to ensure that training for Mayday prevention and Mayday operations are consistent between all fire fighters, company officers, and chief officers.17
Recommendation #3: Fire departments should train fire fighters in air management techniques to ensure they receive the maximum benefit from their SCBA.
Discussion: It is dangerous for fire fighters to attempt to conserve air by intermittently removing their facepieces and taking a quick breath of ambient air. SCBA air cylinders contain a finite volume of air, regardless of the size. Air consumption will vary with each individual's physical condition, their level of training, the task(s) being performed, and the environment. Working within structures requires that fire fighters be cognizant of the distance and the time required to reach the point of suppression activity from the point of entry/egress. When conditions deteriorate and visibility becomes limited, fire fighters may find that it takes additional time to exit when compared to the time it took to enter the structure.13, 20 Depending on the individual's air consumption and the amount of time required to exit an IDLH environment, the low-air alarm may not provide adequate time to exit.
Air management techniques should be a regular part of fire fighters' training. NFPA 1404 Standard for Fire Service Respiratory Protection Training,21 Paragraph 5.1.4(2), requires fire departments to train fire fighters on air management techniques so that the individual fire fighter will develop the ability to manage air consumption while wearing a SCBA. NFPA 1404 A.5.1.4(2) specifies that the individual air management program should include the following directives: (1) fire fighters should exit an IDLH atmosphere before consumption of reserve air supply begins, (2) the low-air alarm is notification that the individual is consuming the reserve air supply, and (3) the fire fighter and his/her crew should take immediate action when a crew member's reserve air alarm is activated.
Fire departments should regularly conduct training exercises in which fire fighters perform various exercises and work tasks at different work rates until their SCBA cylinder air is exhausted. With this type of training, fire fighters will understand the length of time they can expect to work before the low-air alarm sounds and how long they have to exit once the alarm sounds. In order to comply with NFPA 1404, fire departments and fire fighters should follow the rule of air management which states, "Know how much air you have in your SCBA and manage that air so that you leave the hazardous environment before your low-air alarm activates."22, 23 By being aware of these time parameters, fire fighters can make educated decisions on the time they can safely spend in IDLH atmospheres.
Prior to the Mayday issued by Victim #1, many fire fighters working on the 3rd floor had exited to change their air bottles, including members of the victims' crew. Both victims' SCBA cylinders were found to be depleted when they were found.
Fire departments should be aware of the recently released 2010 International Association of Fire Chiefs' (IAFC) Rules of Engagement (ROE) of Structural Firefighting.18 These guidelines recommend that fire fighters maintain awareness of their air supply, situation, location and fire conditions.
Recommendation #4: Fire departments should ensure that fire fighters use their SCBA during all stages of a fire and are trained in SCBA emergency procedures.
Discussion: Fire departments should adopt a zero tolerance response to all department members who only use an SCBA during interior firefighting. Non-visible fire does not mean "no hazard for fire fighters." Fire fighters are often tasked to operate within environments which pose inhalation hazards (e.g., toxic smoke and oxygen deficiency),24 defined by the Occupational Safety and Health Administration (OSHA) as IDLH. OSHA 29 CFR 1910.134 (g)(4)(iii) states, "The employer shall ensure that all employees engaged in interior structural firefighting use SCBAs."3 NFPA 1500 Standard on Fire Department Occupational Safety and Health Program states, "When engaged in any operation where they could encounter atmospheres that are immediately dangerous to life or health (IDLH) or potentially IDLH, or where the atmosphere is unknown, the fire department shall provide and require all members to use SCBA that has been certified as being compliant with NFPA 1981 Standard on Open-Circuit Self-Contained Breathing Apparatus for Fire and Emergency Services." 8, 25 NFPA 1500 Section 7.9.8 restricts fire fighters from removing their facepieces anytime while operating in an IDLH or potentially IDLH atmosphere.
Fire fighters must understand that as temperatures increase in the initial stages of a fire, plastics begin to give off large quantities of various gases. This is called quantitative decomposition, and it happens long before materials reach their ignition temperatures.26 The two principal toxins in smoke—carbon monoxide and hydrogen cyanide—act to deprive the brain of oxygen, and their effects would be enhanced due to the lower levels of oxygen in the air.27 Hydrogen cyanide is a colorless, odorless gas that is released from plastics, natural and synthetic building components, and household items like carpet fibers and polyurethane foam cushions—all of which were present in the structure. Symptoms of hydrogen cyanide exposure include confusion, involuntary muscle movement, vertigo, shortness of breath, or coma.28 Also, carbon monoxide, a by-product of incomplete combustion, can be present before fire fighters visualize fire, and its exposure will present in the same manner as hydrogen cyanide. Even if nothing but carbon dioxide, water vapor, and nitrogen were present in the fire products, and these were to mix with the air being breathed by a fire fighter, then the oxygen percentage would be reduced below the normal 21%. At 15% oxygen, fire fighters can experience lethargy, poor coordination, and confused thinking. During this incident, there were multiple instances where fire fighters inside the structure and on the roof operated without donning an SCBA and/or their facepiece in moderate to heavy smoke conditions.
Emergencies created by, or associated with, the use of an SCBA can be overcome in several ways. Fire departments should develop and implement a comprehensive respiratory protection program21 that includes fire fighter fitness, training, and competency and skill assessments in SCBA and emergency procedures. Fire fighters should remember the first rule in any emergency situation—do not panic. Panic causes an increased breathing rate, which causes an increase in air consumption and an inability to focus on emergency procedures. Removing one's facepiece in an IDLH atmosphere can immediately expose the respiratory system to a potentially fatal environment, thus incapacitating an individual. Choosing to leave one's SCBA facepiece on may be the best chance in providing additional time for a fire fighter to be rescued. Fire fighters should follow their department's SOPs regarding emergency SCBA procedures and emergency communications. Fire departments who do not have written procedures on SCBA use should develop and enforce them. Proper training along with an implemented and enforced policy or procedure will assist fire fighters with proper maintenance, use, and removal of an SCBA.
Recommendation #5: Fire departments should ensure that a separate incident safety officer (ISO), independent from the incident commander, is appointed at each structure fire with the initial dispatch.
Discussion: According to NFPA 1561 Standard on Emergency Services Incident Management System,29 "The incident commander shall have overall authority for management of the incident and the incident commander shall ensure that adequate safety measures are in place." This shall include overall responsibility for the safety and health of all personnel and for other persons operating within the incident management system. While the incident commander is in overall command at the scene, certain functions must be delegated to ensure adequate scene management is accomplished.29 According to NFPA 1500 Standard on Fire Department Occupational Safety and Health Program,25 "as incidents escalate in size and complexity, the incident commander shall divide the incident into tactical-level management units and assign an incident safety officer (ISO) to assess the incident scene for hazards or potential hazards." These standards indicate that the incident commander is in overall command at the scene but acknowledge that oversight of all operations is difficult. Although, the presence of a safety officer does not diminish the responsibility of individual fire fighters and fire officers for their own safety and the safety of others, on-scene fire fighter health and safety is best preserved by delegating the function of safety and health oversight to the ISO.
NFPA 1521 Standard for Fire Department Safety Officer defines the role of the ISO at an incident scene and identifies duties such as recon of the fireground and reporting pertinent information back to the incident commander; ensuring the department's accountability system is in place and operational; monitoring radio transmissions and identifying barriers to effective communications; and ensuring established safety zones, collapse zones, hot zones, and other designated hazard areas are communicated to all members on scene.30 The ISO adds a higher level of attention and particular expertise in analyzing safety hazards, building construction, fire conditions and in the particular uses and/or limitations of protective equipment, which will help fire fighters and fire officers. 31 Larger fire departments may assign one or more full-time staff officers as safety officers who respond to working fires. In smaller departments, every officer should be prepared to function as the ISO when assigned by the incident commander. When the designated ISO is not immediately dispatched or available at the scene, the IC should appoint an ISO. Line officers should receive sufficient training to act as an ISO where needed, until the designated ISO arrives on scene. This will ensure the presence of an ISO on the fireground at all times. The ISO should also be added to the first alarm of a reported fire and for additional incidents that the fire department sees necessary.
Additionally, the incident commander relies upon fire fighters and the ISO to relay feedback on fireground conditions in order to make timely, informed decisions regarding risk versus gain and offensive-versus-defensive operations. The safety of all personnel on the fireground is directly impacted by clear, concise, and timely communications among mutual aid fire departments, sector command, the ISO, and the incident commander.
During this incident, the ISO was not part of the initial dispatch, arriving more than 20 minutes after the initial dispatch, because the incident occurred after hours, which required the on-call ISO to be requested for his assistance.
Recommendation #6: Fire departments should ensure that a rapid intervention team (RIT) is readily available and prepared to respond to fire fighter emergencies.
Discussion: A RIT should be designated and available to respond before interior attack operations begin and throughout the duration of the incident. The team should report to the IC and be available within the incident's staging area. When standing by, the RIT should monitor radio traffic and size up the incident, but not assist in regular fire fighting activities. NFPA 1500, section 8.8.7 states, "At least one dedicated RIT shall be standing by with equipment to provide for the rescue of members that are performing special operations or for members that are in positions that present an immediate danger of injury in the event of equipment failure or collapse.25 The RIT should have all tools necessary to complete the job, e.g., search and rescue ropes, Halligan bar and flat-head axe combo, first-aid kit, and resuscitation equipment.32 These teams can intervene quickly to rescue a fire fighter who is running out of breathing air, disoriented, lost in smoke-filled environments, trapped by fire, or involved in structural collapse.25
During this incident, E7 who was originally assigned as the RIT, was placed in an operational role prior to E12 being available and staged at the command post to take over RIT duties. Conditions at an incident scene can change at any time and not having an available RIT to assist in monitoring radio traffic and respond to those potential emergencies could be detrimental.
Fire departments should be aware of the recently released 2010 International Association of Fire Chiefs' (IAFC) Rules of Engagement (ROE) of Structural Firefighting. These guidelines recommend that ICs always have a rapid intervention team in place at all working fires.18
Recommendation #7: Fire departments should consider adopting a comprehensive wellness and fitness program, provide annual medical evaluations consistent with NFPA standards, and perform annual physical performance (physical ability) evaluations for all fire fighters.
Discussion: The degree to which the victims' medical conditions contributed to their deaths is not certain. However, NIOSH investigators believe that the adoption of a comprehensive wellness and fitness program, annual medical evaluations, and annual physical ability evaluations have merit and should be considered by all fire departments. Such programs have the potential to provide early detection and/or reduction of risk factors associated with cardiovascular disease. Worksite health promotion programs have been shown to increase productivity, reduce absenteeism, and reduce the number of work-related injuries and lost work days.33-34 Fire service health promotion programs have been shown to reduce coronary artery disease risk factors and improve fitness levels, with mandatory programs showing the most benefit.35-37 The cost effectiveness of these health promotion programs was reported in a study conducted by the Oregon Health and Science University, which reported a savings of more than $1 million for each of four large fire departments implementing the IAFF/IAFC wellness/fitness program compared to four large fire departments not implementing a program. These savings were primarily due to a reduction of occupational injury/illness claims with additional savings expected from reduced future nonoccupational healthcare costs.38
Guidance for fire department wellness/fitness programs to reduce risk factors for cardiovascular disease and improve cardiovascular capacity is found in NFPA 1583 Standard on Health-Related Fitness Programs for Fire Fighters, the IAFF/IAFC Fire Service Joint Labor Management Wellness/Fitness Initiative, the National Volunteer Fire Council's Health and Wellness Guide, and in Firefighter Fitness: A Health and Wellness Guide.39-42
Guidance regarding the content and frequency of annual medical evaluations can be found in NFPA 1582 Standard on Comprehensive Occupational Medical Program for Fire Departments and in the IAFF/IAFC Fire Service Joint Labor Management Wellness/Fitness Initiative .5, 40 These guidelines help to determine fire fighters' medical ability to perform duties without presenting a significant risk to the safety and health of themselves or others.
NFPA 1500 recommends that fire department members who engage in emergency operations be annually evaluated and certified by the fire department as having met the physical performance requirements identified in paragraph 10.2.3 of the standard.25 This is recommended to ensure fire fighters are physically capable of performing the essential job tasks of structural fire fighting. The physical ability test could be performed as part of the fire department's annual training program.
Recommendation #8: Fire departments should ensure that accountability is maintained and that fire fighters maintain crew integrity when operating on the fireground, especially when performing interior fire suppression activities.
Discussion: The use of an accountability system is recommended by NFPA 1500 Standard on Fire Department Occupational Safety and Health Program and NFPA 1561 Standard on Emergency Services Incident Management System.25, 29 A functional personnel accountability system requires the following:
- Development of a departmental SOP
- Training all personnel
- Strict enforcement during emergency incidents
As the incident escalates, additional staffing and resources may be needed, adding to the burden of tracking personnel. At this point, an accountability system should be in place which includes an incident command board that is established and maintained by an assigned accountability officer or aide. A properly maintained incident command board allows the IC to readily identify the location and time of all fire fighters on the fireground. As a fire escalates and additional fire companies respond, a chief's aide or accountability officer assists the IC with accounting for all fire fighting companies at the fire, at the staging area, and at the rehabilitation area. A properly initiated and enforced accountability system on every response, which is consistently integrated into fireground command and control, enhances fire fighter safety and survival by helping to ensure a more timely and successful identification and rescue of a disoriented or downed fire fighter.
Fire fighters should always work and remain in teams whenever they are operating in a hazardous environment.32 Team integrity depends on team members knowing who is on their team and who is the team leader; staying within visual contact at all times (if visibility is low, teams must stay within touch or voice distance of each other); communicating needs and observations to the team leader; and rotating together for team rehab, team staging, and watching out for each other (e.g., practicing a strong buddy system). Following these basic rules helps prevent serious injury or even death by providing personnel with the added safety net of fellow team members. Teams that enter a hazardous environment together should leave together to ensure that team continuity is maintained.43
Fire departments should be aware of the recently released 2010 International Association of Fire Chiefs' (IAFC) Rules of Engagement (ROE) of Structural Firefighting.18 The 2010 IAFC ROE of Structural Firefighting states, "Go in together, stay together, come out together."18These guidelines also recommend that the IC ensure accurate accountability of every fire fighter's location and status.
Recommendation #9: Fire departments should formulate and institute a heat stress program and a rehabilitation (rehab) program in accordance with NFPA 1584 Standard on the Rehabilitation Process for Members during Emergency Operations and Training Exercises.
Discussion: Emergency medical care and transportation for injured or ill fire fighters should be immediately available on the scene of working structure fires. In order for this to occur, EMS should be included on the first alarm of fire incidents and additional incidents that a fire department feels necessary. Several fire fighters experienced and were treated for heat-related illnesses at this incident. Heat stress is the exposure to heat loads. Sources of heat include the metabolic cost of work, environmental factors (i.e., air temperature, humidity, air movement, and radiant heat exchange), and clothing.32 Heat strain is the overall physiological response resulting from heat stress.44 Sudden and severe fatigue, nausea, dizziness, or lightheadedness are symptoms of heat strain and should trigger removal from heat sources. Some common heat-related disorders include heat syncope, dehydration and loss of electrolytes, heat exhaustion, and heat stroke. Heat-related disorders vary in degree of severity, although all but heat stroke resolve with no lasting complications.44
The prime objective of heat stress management is the prevention of heat stroke which is life-threatening and the most serious of the heat-related disorders.44 The key to managing heat stress is to be familiar with controls used to prevent it and minimize its effect. As recommended by the U.S. Fire Administration's document Emergency Incident Rehabilitation, controls for heat stress include (1) fluid intake, (2) work rotation, (3) active cooling, and (4) rest.44 Most heat stress illnesses are due, in major part, to a failure to maintain adequate hydration. When dehydrated, the body's ability to thermoregulate is impaired.45 Sweating and excreting fluids faster than the body can absorb new fluids is physiologically possible. The likelihood and severity of heat strain experienced by an individual for a given level of heat stress depends on the physiological capacity of that individual to respond to stress.44 Over time, humans have the ability to adapt and become more proficient in handling extreme environmental conditions (acclimatization). Personal risk factors such as age, obesity, state of hydration, use of medications and drugs, gender, and state of acclimatization may reduce an individual's tolerance for heat stress.44
An IC should consider the circumstances of each incident in determining the need for rehabilitation.25 A rehab area should be located sufficiently away from the operation so that members can safely remove their PPE and SCBA, be staffed to include at least basic life support (for medical monitoring of heart rate, blood pressure, temperature, and perceived exertion) and have fluid and food available.46 An SOP/SOG should be written that outlines a systematic approach for rehab at incidents and include rehab operations that consider hot weather conditions (i.e., temperature, relative humidity, and direct sunlight) and who will be assigned rehab duties for the incident.
Fire departments should be aware of the recently released 2010 International Association of Fire Chiefs' (IAFC) Rules of Engagement (ROE) of Structural Firefighting.18 These guidelines recommend that ICS always have fire fighter rehab services in place at all working fires.
Recommendation #10: Fire departments should ensure that policies and procedures for proper inspection, use, and maintenance of SCBA are followed to ensure they function properly when needed.
NFPA 1981 Standard on Open-Circuit Self-Contained Breathing Apparatus for Emergency Services and NFPA 1852 Standard on Selection, Care, and Maintenance of Open-Circuit Self-Contained Breathing Apparatus speak directly to the maintenance and use of self-contained breathing apparatus.8, 47 The fire department has established a preventative maintenance program for their SCBAs. Annual maintenance, testing, and repairs require an individual to receive specialized training from factory-certified technicians and to perform required tasks as outlined by the manufacturer. This requires special tools, equipment, and knowledge to take apart the components of a SCBA, which are normally not available to a fire department. Daily, weekly, and or monthly inspections of a SCBA needs to be documented to include items like air cylinder and remote pressure gauge readings, general state of SCBA components and face piece, PASS device actuation, and regulator flow test and hydrostatic tests. A documented inspection can catch minor issues before they result in a SCBA malfunction or failure.
During this incident, it was discovered that both victims' SCBA cylinders did not have a current hydrostatic test date. Victim #1's SCBA end of service alarm did not actuate when it was supposed to (1,035 to 1,215 psig or 23% to 27% of full pressure). Additional information on the SCBA evaluations can be found within Appendix II.
References
- Fire department [1992-2010]. Operational procedure guidelines, standard operating procedures, and directives.
- Occupation Safety and Health Administration (OSHA). 29 CFR 1910.156 Fire brigades. [https://www.osha.gov/pls/oshaweb/owadisp.show_document?p_id=9810&p_table=STANDARDS]. Date accessed: February 2011.
- Occupational Safety and Health Administration (OSHA). 29 CFR 1910. 134 Respiratory protection. [https://www.osha.gov/pls/oshaweb/owadisp.show_document?p_table=STANDARDS&p_id=12716]. Date accessed: February 2011.
- NIOSH [1999]. Fire fighter dies at the scene of a small fire in an apartment building—Connecticut. Morgantown, WV: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, Fatality Assessment and Con42ecti Evaluation (FACE) Report No. 199918. [http://www.cdc.gov/niosh/fire/reports/face9918.html]. Date accessed: February 2011.
- NFPA [2007]. NFPA 1582 standard on comprehensive occupational medical program for fire departments. 2007 ed. Quincy, MA: National Fire Protection Association.
- IAFC. The IAFF/IAFC fire service joint labor management candidate physical ability test program summary. International Association of Fire Chiefs. [http://www.iafc.org/Operations/content.cfm?ItemNumber=1174]. Date accessed: February 2011. (Link updated 9/19/2011)
- NFPA [2008]. NFPA 1001 standard for firefighter professional qualifications. 2008 ed. Quincy, MA: National Fire Protection Association.
- NFPA [2007]. NFPA 1981 standard on open-circuit self-contained breathing apparatus for fire and emergency services. 2007 ed. Quincy, MA: National Fire Protection Association.
- NFPA [2007]. NFPA 1982 standard on personal alert safety systems (PASS). 2007 ed. Quincy, MA: National Fire Protection Association.
- . NFPA [2008]. NFPA 1989 standard on breathing air quality for emergency services respiratory protection. 2008 ed. Quincy, MA: National Fire Protection Association.
- Kerber S, Madrzykowski D [2009]. Fire fighting tactics under wind driven conditions: 7 story building experiments. Gaithersburg, MD: National Institute of Standards and Technology, April 2009, NIST TN 1629.
- Angulo RA, Clark BA, Auch S [2004]. You called mayday! Now what? Fire Engineering, September.
- Clark BA [2004]. Calling a mayday: the drill. [http://www.firehouse.com/article/10515446/calling-a-mayday-the-drill]. Date accessed: February 2011. (Link Updated 1/28/2013)
- DiBernardo JP [2003]. A missing firefighter: give the mayday. Firehouse, November.
- Sendelbach TE [2004]. Managing the fireground mayday: the critical link to firefighter survival. [http://www.firehouse.com/topic/firefighter-safety/managing-fireground-mayday]. Date accessed: February 2011. (Link no longer available 12/6/2012)
- Miles J, Tobin J [2004]. Training notebook: mayday and urgent messages. Fire Engineering, April.
- IAFF. IAFF Fire Ground Survival Program. International Association of Fire Fighters. [http://www.iaff.org/HS/FGS/FGSIndex.htm]. Date accessed: April 2011.
- IAFC Safety, Health, and Survival Section [2010]. Rules of engagement of structural firefighting (poster). International Association of Fire Chiefs, Safety, Health and Survival Section [http://websites.firecompanies.com/iafcsafety/files/2013/10/ROE_Poster_FINAL1.pdf]. Date accessed: February 2011. (Link Updated 1/14/2014)
- Clark, BA [2005]. 500 Maydays called in rookie school. [http://www.firehouse.com/article/10498807/500-maydays-called-in-rookie-school]. Date accessed: February 2011. (Link Updated 1/28/2013)
- Clark BA [2008]. Leadership on the line: firefighter mayday doctrine where are we now? Radio@Firehouse.com [http://www.firehouse.com/podcast/10459336/leadership-on-the-line-firefighter-mayday-doctrine-where-are-we-now]. Date accessed: February 2011. (Link Updated 1/28/2013)
- NFPA [2006]. NFPA 1404 standard for fire service respiratory protection training. 2006 ed. Quincy, MA: National Fire Protection Association.
- NIOSH [2001]. Supermarket fire claims the life of one career fire fighter and critically injures another career fire fighter—Arizona. Morgantown, WV: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, Fatality Assessment and Control Evaluation (FACE) Report F2001-13. [http://www.cdc.gov/niosh/fire/reports/face200113.html]. Date accessed: February 2011.
- Bernocco S, Gagliano M, Phippips C, Jose P [2008]. Is your department complying with the NFPA 1404 air management policy? Fire Engineering 161(2):103108.
- Klinoff R [2003]. Introduction to fire protection. 2nd ed. Clifton Park, NY: Thomas Delmar Learning.
- NFPA [2007]. NFPA 1500 standard on fire department occupational safety and health program. 2007 ed. Quincy, MA: National Fire Protection Association.
- Wallace D [1990]. In the mouth of the dragon: toxic fire in the age of plastics. New York, NY: Avery Publishing Group.
- Friedman R [1998]. Principles of fire protection chemistry and physics. Quincy, MA: National Fire Protection Association.
- Gagliano M, Phillips C, Jose P, Bernocco S [2008]. Air management for the fire service. Tulsa, OK: Penn Well Corporation.
- NFPA [2008]. NFPA 1561 standard on emergency services incident management system. 2008 ed. Quincy, MA: National Fire Protection Association.
- NFPA [2008]. NFPA 1521 standard for fire department safety officer. 2008 ed. Quincy, MA: National Fire Protection Association.
- Dodson D [2007]. Fire department incident safety officer. 2nd ed. Clifton Park, NY: Thomson Delmar Learning.
- IFSTA [2008]. Essentials of fire fighting. 5th ed. Stillwater, OK: Fire Protection Publications, International Fire Service Training Association.
- Stein AD, Shakour SK, Zuidema RA [2000]. Financial incentives, participation in employer sponsored health promotion, and changes in employee health and pro¬ductivity: HealthPlus health quotient program. J Occup Environ Med 42(12):11481155.
- Aldana SG [2001]. Financial impact of health promotion programs: a comprehensive review of the literature. Am J Health Promot 15(5):296320.
- Dempsey WL, Stevens SR, Snell CR [2002]. Changes in physical performance and medical measures following a mandatory firefighter wellness program. Med Sci Sports Exerc 34(5):S258.
- Womack JW, Humbarger CD, Green JS, Crouse SF [2005]. Coronary artery disease risk factors in firefighters: effectiveness of a one-year voluntary health and wellness program. Med Sci Sports Exerc 37(5):S385.
- Blevins JS, Bounds R, Armstrong E, Coast JR [2006]. Health and fitness programming for fire fighters: does it produce results? Med Sci Sports Exerc 38(5):S454.
- Kuehl K [2007]. Economic impact of the wellness fitness initiative. Presentation at the 2007 John P. Redmond Symposium, Chicago, IL, October 2007.
- NFPA [2008]. NFPA 1583 standard on health-related fitness programs for fire department members. 2008 ed. Quincy, MA: National Fire Protection Association.
- IAFF, IAFC [2008]. The fire service joint labor management wellness/fitness initiative. 3rd ed. Washington, DC: International Association of Fire Fighters, International Association of Fire Chiefs.
- NVFC [2008]. Health and wellness guide for the volunteer fire and emergency services. Green Belt, MD: National Volunteer Fire Council. [http://www.nvfc.org/files/documents/HealthWellness_guide.pdf]. Date accessed: February 2011.
- Schneider EL [2010]. Firefighter fitness: a health and wellness guide. New York, NY: Nova Science Publishers.
- Dunn V [1992]. Safety and survival on the fireground. Saddle Brook NJ: Fire Engineering Books and Videos.
- USFA [2008]. Emergency incident rehabilitation. Emmitsburg, MD: U.S. Department of Homeland Security, Federal Emergency Management Agency, U.S. Fire Administration, National Fire Academy.
- ACGIH [2001]. Heat stress and strain. Washington, DC: American Conference on Governmental Industrial Hygienists.
- NFPA [2008]. NFPA 1584 standard on the rehabilitation process for members during emergency operations and training exercises. 2008 ed. Quincy, MA: National Fire Protection Association.
- NFPA [2008]. NFPA 1852 standard on selection, care, and maintenance of open-circuit self-contained breathing apparatus (SCBA). 2008 ed. Quincy, MA: National Fire Protection Association.
Investigator Information
This incident was investigated by Stacy C. Wertman and Virginia Lutz, safety and occupational health specialists, with the Fire Fighter Fatality Investigation and Prevention Program, Surveillance and Field Investigations Branch, Division of Safety Research, NIOSH located in Morgantown, WV. This report was authored by Stacy C. Wertman, MS, ISO. Tom Pouchot, NIOSH General Engineer, National Personal Protective Technology Laboratory, conducted an evaluation of the victim's SCBA. An expert technical review was provided by Deputy Fire Chief William Goldfeder of the Loveland-Symmes (OH) Fire Department and editor of FireFighterCloseCalls.com and Dr. Burton A. Clark, EFO, CFO, Chair, Management Science Program, National Fire Academy, U.S. Fire Administration. A technical review was also provided by the National Fire Protection Association, Public Fire Protection Division.
Additional Information
State of Connecticut, Commission on Fire Prevention and Control, Candidate Physical Ability Test [http://www.ct.gov/cfpc/cwp/view.asp?a=826&Q=246722].
IAFF Fire Ground Survival Program
The purpose of the International Association of Fire Fighters (IAFF) Fire Ground Survival Program is to ensure that training for Mayday prevention and Mayday operations are consistent between all fire fighters, company officers and chief officers. Fire fighters must be trained to perform potentially life-saving actions if they become lost, disoriented, injured, low on air or trapped. Funded by the IAFF and assisted by a grant from the U.S. Department of Homeland Security through the Assistance to Firefighters (FIRE Act) grant program, this comprehensive Fire Ground Survival training program applies the lessons learned from fire fighter fatality investigations conducted by the National Institute for Occupational Safety and Health (NIOSH) and has been developed by a committee of subject matter experts from the IAFF, the International Association of Fire Chiefs (IAFC) and NIOSH. http://www.iaff.org/HS/FGS/FGSIndex.htm
Disclaimer
Mention of any company or product does not constitute endorsement by the National Institute for Occupational Safety and Health (NIOSH). In addition, citations to Web sites external to NIOSH do not constitute NIOSH endorsement of the sponsoring organizations or their programs or products. Furthermore, NIOSH is not responsible for the content of these Web sites.
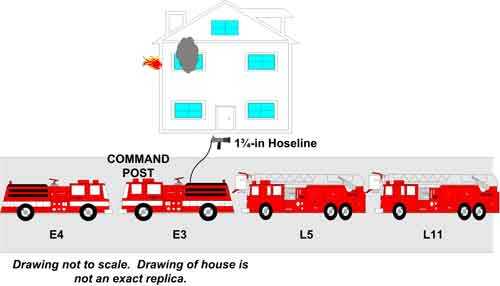 |
Diagram 1. Initial conditions and fire apparatus on scene. Note: E4 and L11 arrived on scene after the initial room and contents fire was brought under control. |
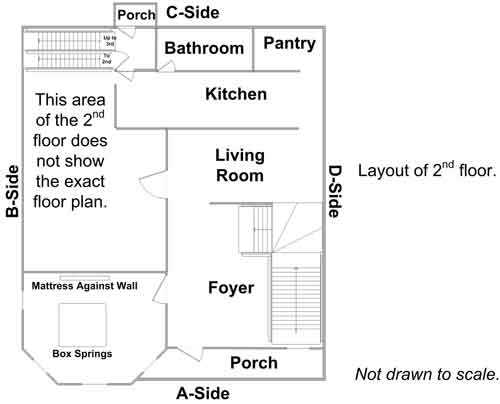 |
Diagram 2. Second floor. |
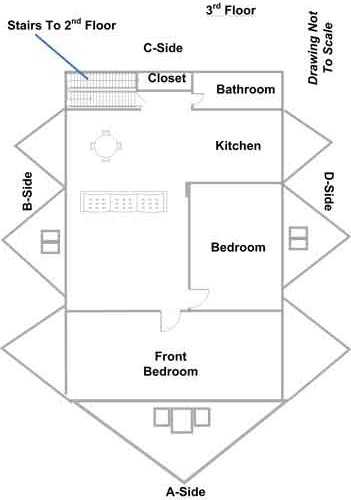
|
Diagram 3. Third floor. |
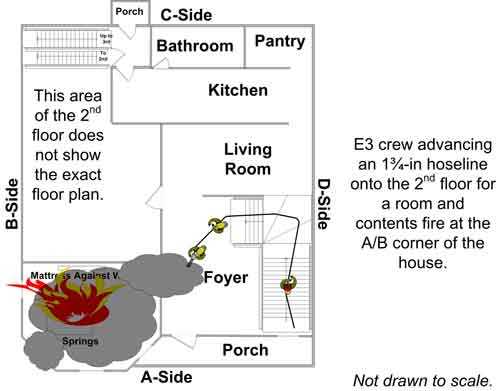 |
Diagram 4. E3 personnel discovered a room and |
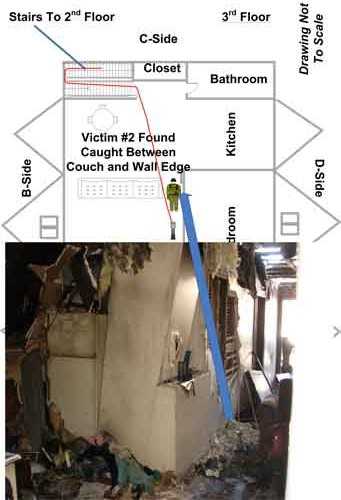
|
Diagram 5. Shows location of where Victim #2 was found by FF4. |
APPENDIX I
Summary of Fire Department Mayday SOP
- Whenever any member is in a situation that they believe to be life-threatening and unable to escape from, they will transmit a Mayday.
- Whenever any member sees another fire fighter or fire fighters in a life-threatening situation they will transmit a Mayday.
- Fire dispatch will broadcast a Mayday tone over both channel (main dispatch) and the assigned fire ground channel. The tone is a rapid, high to low pitch, chirping sound.
- The individual calling the Mayday will repeat the word Mayday three times. Whenever possible, the officer or fire fighter transmitting the Mayday message shall give fire dispatch their last known location, the nature of the emergency, unit designation, and assignment. If calling a Mayday for someone else, give fire dispatch the location of the fire fighter or company in distress and particulars concerning the emergency. The use of the “orange distress button” on the radio should only be used if the member is unable to communicate.
- When fire dispatch hears a Mayday message, they will establish “emergency traffic” by sounding the Mayday tone for 5 full seconds. Fire dispatch will then call the company or individual that transmitted the Mayday, seeking the company or individual location and problem. Fire dispatch will then assign a dedicated rescue channel to units assigned to assist in the removal of the member in distress.
- Upon confirmation of a Mayday and activation of the RIT team, fire dispatch will automatically dispatch 1 engine company, 1 ladder company, and an additional battalion chief to assist with RIT duties on the fire ground. It will be the responsibility of fire dispatch to automatically dispatch these additional units.
- Additional EMS units will be dispatched to the scene if the RIT is activated.
- Members must be prevented from rushing frantically around a building looking for a missing member, while not knowing who is missing, how many are missing, or where they may be. Everyone must understand that the life-threatening emergency, to which we were dispatched, still exists. We cannot abandon it and put more people at the scene, at risk. Companies must keep doing the job they were assigned to, and wait for the incident commander to coordinate the search.
- Whenever a Mayday message is transmitted, a roll call of companies operating at the scene shall be conducted as soon as feasible. However, the roll call shall not be conducted in such a way as to interfere with the rescue of the trapped or missing fire fighter(s). The roll call will not cause excessive radio traffic. The term PAR (personnel accountability report) will be used when answering a roll call. A “PAR” is an announcement from the officer in charge of a crew given only when all of the members assigned to that officer have been located and accounted for.
- Fire dispatch will advise all stations and fire cars that until an all clear has been received from the incident commander regarding the Mayday, all call will be dispatched over the voice alarm and a channel other than the Mayday channel.
- Whenever the term Mayday is transmitted all other communications on the frequency are to cease. Fire dispatch will immediately establish, “emergency traffic” sounding the Mayday tone and call the company initiating the Mayday getting their location and problem.
- Whenever a member becomes trapped or lost they shall transmit a Mayday and if physically able place their PASS alarm in the emergency mode. If the member is unable to communicate with fire dispatch, the “orange distress button” on the radio should also be activated.
- Members should not wait until the last moment to call Mayday
- At the point in the incident that the rescue operation is complete or the incident commander feels that the situation has been stabilized, the incident commander shall transmit an “all clear” to fire dispatch in order to bring Mayday operations to a close.
- Whenever a fire fighter is reported as trapped or lost, the incident commander will deploy the RIT. In addition, the incident commander should consider appointing a rescue group officer to coordinate the search and rescue effort. The rescue group officer should be a chief officer, but in the absence of an additional chief officer on the scene, an experienced company officer may be used.
- Reference to Emergency Evacuation for Rescue Procedure
- Reference to Rapid Intervention Team
- Mayday procedure testing:
- Every first day shift (Monday), a Mayday radio test will be conducted.
- The procedure will be tested in the following manner.
- Immediately following the completion of the radio test and evacuation tone test, fire dispatch will contact the company scheduled to do the test that day, via the red phone. Fire dispatch will inform the company that it is standing by for the Mayday test.
- A member from the company will then use a department radio to call fire dispatch using the channel designated by fire dispatch.
Note: A practice Mayday call is then transmitted over the radio following the established Mayday procedure.
APPENDIX II
Status Investigation Report of Two
Self-Contained Breathing Apparatus
Submitted By the
Connecticut State Police for the
Fire Department
NIOSH Task Number 17565
(Note: Full report is available upon request)
Background
As part of the National Institute for Occupational Safety and Health (NIOSH) Fire Fighter Fatality Investigation and Prevention Program, the Technology Evaluation Branch agreed to examine and evaluate two SCBA identified as Scott Health and Safety model AirPak AP75, 4500 psi, 30-minute, self-contained breathing apparatus (SCBA).
This SCBA status investigation was assigned NIOSH Task Number 17565. The Connecticut State Police Department was advised that NIOSH would provide a written report of the inspections and any applicable test results.
The SCBA units, contained within corrugated cardboard boxes, were delivered to the NIOSH facility in Bruceton, Pennsylvania on January 13, 2011. After their arrival, the packages were taken to building 20 and stored under lock until the time of the evaluations.
SCBA Inspection
The packages were opened initially in the Respirator Fit Test Lab (building 40) on January 20, 2011 and an initial visual inspection was conducted by Tom Pouchot, General Engineer NPPTL. The SCBA identified as Connecticut State Police exhibit 20 was labeled by NPPTL as SCBA Unit #1. The SCBA identified as Connecticut State Police exhibit 26 was labeled by NPPTL as SCBA Unit #2. Also at that time, Scott Health and Safety conducted a downloading of the data loggers for each SCBA. The units were identified as the Scott Health and Safety Company model AirPak AP75, 30 minute, 4500 psi unit, NIOSH approval number TC-13F-0076CBRN. Once initial visual inspection and data logger downloading were completed, the SCBA units were repackaged and placed back in building 20 under lock.
The complete visual inspection of the units was conducted on February 9, 2011. These SCBA units were examined, component by component, in the condition received to determine the conformance of the unit to the NIOSH-approved configuration. The visual inspection process was documented photographically.
The complete SCBA inspections are summarized in Appendix I of the full evaluation report. The condition of each major component of the SCBA that were photographed with a digital camera is contained in Appendix III of the full evaluation report.
It was judged that the unit could be safely pressurized and tested using a substitute cylinder provided by Scott Health and Safety. The substitute cylinder was also used for the NIOSH tests that were performed.
After testing, at the request of the Connecticut State Police, representatives of Scott Health and Safety traveled to the NIOSH facility to perform maintenance on Unit #2 SCBA to attempt to adjust the End of Service Alarm/Vibra Alert to within the NIOSH requirements. This maintenance was performed on March 10, 2011.
SCBA Testing
The purpose of the testing was to determine the conformance of each SCBA to the approval performance requirements of Title 42, Code of Federal Regulations, Part 84 (42 CFR 84). Further testing was conducted to provide an indication of the conformance of each SCBA to the National Fire Protection Association (NFPA) Air Flow Performance requirements of NFPA 1981, Standard on Open-Circuit Self-Contained Breathing Apparatus for the Fire Service, 1997 Edition.
NIOSH SCBA Certification Tests (in accordance with the performance requirements of 42 CFR 84):
1. Positive Pressure Test [§ 84.70(a)(2)(ii)]
2. Rated Service Time Test (duration) [§ 84.95]
3. Static Pressure Test [§ 84.91(d)]
4. Gas Flow Test [§ 84.93]
5. Exhalation Resistance Test [§ 84.91(c)]
6. Remaining Service Life Indicator Test (low-air alarm) [§ 84.83(f)]
National Fire Protection Association (NFPA) Tests (in accordance with NFPA 1981, 1997 Edition):
7. Air Flow Performance Test [Chapter 5, 5-1.1]
Units #1 and #2 were tested on February 10 and 11, 2011 using substitute cylinders.
Appendix II of the full evaluation report contains the complete NIOSH and NFPA test reports for each of the SCBA. Tables One and Two of the full evaluation report summarize the NIOSH and NFPA test results.
In addition, after Unit #2 was tested and found to be out of NIOSH compliance for the end of service alarm, Scott Health and Safety was contacted at the request of the Connecticut State Police to evaluate the out of compliance performance. On March 10, 2011, Scott Health and Safety representatives traveled to the NIOSH facility and inspected, cleaned and adjusted the SCBA unit with NIOSH personnel witnessing the actions. The Scott representatives were unable to bring the SCBA end of service alarm up to a NIOSH compliant level. Scott stated that a more invasive inspection and adjustment would be required at the Scott production facility in Monroe, North Carolina and that adjustment would bring this unit back into compliance. After consulting the Connecticut State Police, the decision was made that this additional adjustment would not be performed on Unit #2.
Summary and Conclusions
Two SCBA units were submitted to NIOSH by the Connecticut State Police Department for the Fire Department for evaluation. The SCBA units were delivered to NIOSH on January 13, 2011 and initially inspected on January 20, 2011. The units were identified as a Scott Health and Safety model AirPak AP75, 4500 psi, 30-minute, SCBA (NIOSH approval number TC-13F-0076CBRN). At that time Scott Health and Safety performed a downloading of the unit data loggers. The complete inspection of the SCBA units was conducted on February 9, 2011. The units suffered minimal heat damage, exhibited other signs of wear and tear and the units were covered lightly with general dirt, grime, foreign particulate material and soot. The cylinder valves as received, Unit #1 was in the open position and Unit #2 was in the closed position. The cylinder gauges read approximately 0 psig. The cylinder valve hand-wheels could be turned. The regulator and facepiece mating and sealing areas on the units were relatively clean and there was no debris on the inside of the facepieces. The rubber face seal on Unit #1 was warped and distorted somewhat. The harness webbing on the units were in good condition with no fraying or tears but the webbing was dirty. The PASS device on the units functioned. The NFPA approval labels on the units were present and readable. Visibility through the lens of the unit facepieces was fair as the lenses had some scratches and other foreign material present.
The air cylinder on Unit #1 had a manufactured date of 1/04. Under the applicable DOT-E-10945-4500 exemption, the air cylinder is required to be hydro tested every 5 years, starting on or before the last day of 1/09. Therefore it appears that the cylinder on this SCBA unit was due for hydro testing before the end of January 2009. There was no re-test label or indication on the cylinder assembly for Unit #1 and therefore it appears that this cylinder was not within the hydro certification when last used. The Unit #1 cylinder also had some light gouges with the outer resin peeling away from the inner composite material in some areas.
The air cylinder on Unit #2 had a manufactured date of 9/98. Under the applicable DOT-E-10945-4500 exemption, the air cylinder is required to be hydro tested every 5 years, starting on or before the last day of 9/03. Therefore it appears that the cylinder on this SCBA unit was due for hydro testing before the end of September 2003 and repeat testing before the end of September 2008. The re-test label indicates that the last hydro test was performed 4/03. There was no re-test label or indication on the cylinder for re-testing during 2008 and therefore it appears that this cylinder was not within the hydro certification when last used. Unit #2 cylinder also had some light scratches and scuffs over the whole assembly.
Replacement air cylinders with a current hydrostatic re-test qualification were obtained from Scott Health and Safety and were substituted for all tests. No other maintenance or repair work was performed on the units at any time.
SCBA Unit #1 met the requirements of the NIOSH Positive Pressure Test, with a minimum pressure of 0.1 inches of water. Unit #1 met the requirements of all of the other NIOSH tests.
SCBA Unit #2 met the requirements of the NIOSH Positive Pressure Test, with a minimum pressure of 0.00 inches of water. Unit #2 did not meet all the requirements of all the other tests. This unit failed the End of Service Life Indicator/Alarm test.
Scott Health and Safety personnel traveled to NIOSH on March 10, 2011 and inspected, cleaned and adjusted Unit #2 in an attempt to bring the SCBA back into NIOSH compliance. The Scott representatives were unable to bring the SCBA end of service alarm up to a NIOSH compliant level. Scott stated that a more invasive inspection and adjustment would be required at the Scott production facility in Monroe, North Carolina and that adjustment would bring this unit back into compliance. After consultation with the Connecticut State Police, the decision was made that no further maintenance would be performed on Unit #2.
In light of the information obtained during this investigation, NIOSH has proposed no further action on its part at this time. Following inspection and testing, the SCBA was returned to storage pending return to the Connecticut State Police.
If the units are to be placed back in service, the SCBA’s must be repaired, tested, and inspected by a qualified service technician, including such testing and other maintenance activities as prescribed by the schedule from the SCBA manufacturer. Typically a flow test is required on at least an annual basis.
PASS Device Data
Table 1 and Table 2 contain information from the PASS devices used by the victims. According to the recorded data, both PASS devices appeared to be functioning appropriately during the incident. Benchmark times, noted with an “X,” show the PASS devices being turned off/on, sensing, going into pre-alarm/alarm, and even being reset at different times. The lapse of times between benchmarks may have included the unit being powered off or there was ample movement not allowing the PASS device to sense no movement.
According to the timeline documented by NIOSH investigators, through the use of written and audible radio transcripts/transmissions, the PASS devices’ internal clock appeared to behind by 1 hour. NIOSH investigators cannot account for what was happening within the structure when Victim #1 transmitted a Mayday, or what happened with Victim #2 after Victim #1 was discovered unconscious in the stairs off the 3rd floor.
Table 1. Victim #1 PASS data log recorder.
|
Time
|
Date | Off To Sensing |
Sensing |
Pre Alarmg |
Manual |
Alarm |
Low |
Sensing To |
|---|---|---|---|---|---|---|---|---|
15:52:06 |
7/24/2010 |
- |
X |
- |
- |
- |
- |
- |
15:38:16 |
7/24/2010 |
- |
- |
- |
- |
X |
- |
- |
15:36:10 |
7/24/2010 |
- |
- |
- |
X |
- |
- |
- |
15:36:02 |
7/24/2010 |
- |
X |
- |
- |
- |
- |
- |
15:35:44 |
7/24/2010 |
- |
- |
X |
- |
- |
- |
- |
15:35:32 |
7/24/2010 |
- |
- |
- |
- |
- |
- |
X |
15:34:46 |
7/24/2010 |
- |
- |
- |
- |
X |
- |
- |
15:28:18 |
7/24/2010 |
- |
- |
X |
- |
- |
- |
- |
15:28:06 |
7/24/2010 |
- |
- |
- |
- |
- |
- |
X |
15:22:04 |
7/24/2010 |
- |
- |
- |
- |
- |
- |
X |
15:17:20 |
7/24/2010 |
- |
- |
- |
- |
- |
- |
X |
15:12:28 |
7/24/2010 |
- |
- |
- |
- |
- |
- |
X |
15:08:58 |
7/24/2010 |
X |
- |
- |
- |
- |
- |
- |
15:01:34 |
7/24/2010 |
- |
X |
- |
- |
- |
- |
- |
15:01:34 |
7/24/2010 |
- |
- |
- |
- |
X |
- |
- |
15:01:30 |
7/24/2010 |
- |
- |
- |
X |
- |
- |
- |
14:47:04 |
7/24/2010 |
- |
X |
- |
- |
- |
- |
- |
14:46:34 |
7/24/2010 |
X |
- |
- |
- |
- |
- |
- |
Table 2. Victim #2 PASS data log recorder.
|
Time
|
Date | Off To Sensing |
Sensing |
Pre Alarmg |
Manual |
Alarm |
Low |
Sensing To |
|---|---|---|---|---|---|---|---|---|
15:51:48 |
7/24/2010 |
- |
X |
- |
- |
- |
- |
- |
15:51:46 |
7/24/2010 |
- |
- |
- |
- |
X |
- |
- |
15:49:58 |
7/24/2010 |
- |
- |
X |
- |
- |
- |
- |
15:49:46 |
7/24/2010 |
- |
- |
- |
- |
- |
- |
X |
15:49:12 |
7/24/2010 |
- |
- |
- |
- |
X |
- |
- |
15:49:12 |
7/24/2010 |
- |
- |
X |
- |
- |
- |
- |
15:49:00 |
7/24/2010 |
- |
- |
- |
- |
- |
- |
X |
15:48:22 |
7/24/2010 |
- |
- |
- |
- |
X |
- |
- |
15:27:30 |
7/24/2010 |
- |
- |
X |
- |
- |
- |
- |
15:27:18 |
7/24/2010 |
- |
- |
- |
- |
- |
- |
X |
15:18:22 |
7/24/2010 |
- |
- |
- |
- |
- |
- |
X |
15:17:50 |
7/24/2010 |
- |
- |
- |
- |
- |
- |
X |
15:17:28 |
7/24/2010 |
- |
- |
- |
- |
- |
- |
X |
15:16:28 |
7/24/2010 |
- |
- |
- |
- |
- |
- |
X |
15:03:28 |
7/24/2010 |
X |
- |
- |
- |
- |
- |
- |
14:49:16 |
7/24/2010 |
- |
X |
- |
- |
- |
- |
- |
14:48:50 |
7/24/2010 |
- |
- |
- |
- |
- |
- |
X |
14:48:30 |
7/24/2010 |
- |
X |
- |
- |
- |
- |
- |
|
The National Institute for Occupational Safety and Health (NIOSH), an institute within the Centers for Disease Control and Prevention (CDC), is the federal agency responsible for conducting research and making recommendations for the prevention of work-related injury and illness. In 1998, Congress appropriated funds to NIOSH to conduct a fire fighter initiative that resulted in the NIOSH Fire Fighter Fatality Investigation and Prevention Program which examines line-of-duty-deaths or on duty deaths of fire fighters to assist fire departments, fire fighters, the fire service and others to prevent similar fire fighter deaths in the future. The agency does not enforce compliance with State or Federal occupational safety and health standards and does not determine fault or assign blame. Participation of fire departments and individuals in NIOSH investigations is voluntary. Under its program, NIOSH investigators interview persons with knowledge of the incident who agree to be interviewed and review available records to develop a description of the conditions and circumstances leading to the death(s). Interviewees are not asked to sign sworn statements and interviews are not recorded. The agency's reports do not name the victim, the fire department or those interviewed. The NIOSH report's summary of the conditions and circumstances surrounding the fatality is intended to provide context to the agency's recommendations and is not intended to be definitive for purposes of determining any claim or benefit.
|
For further information, visit the program Web site at www.cdc.gov/niosh/fire or call toll free 1-800-CDC-INFO (1-800-232-4636).
This page was last updated on 05/25/2011.
- Page last reviewed: November 18, 2015
- Page last updated: October 15, 2014
- Content source:
- National Institute for Occupational Safety and Health Division of Safety Research