


Supermarket Fire Claims the Life of One Career Fire Fighter and Critically Injures Another Career Fire Fighter - Arizona
 ShareCompartir
ShareCompartir
 Death in the Line of Duty...A summary of a NIOSH fire fighter fatality investigation
Death in the Line of Duty...A summary of a NIOSH fire fighter fatality investigation
F2001-13 Date Released: July 25, 2002
SUMMARY
On March 14, 2001, a 40-year-old male career fire fighter/paramedic died from carbon monoxide poisoning and thermal burns after running out of air and becoming disoriented while fighting a supermarket fire. Four other fire fighters were injured, one critically, while fighting the fire or performing search and rescue for the victim. The fire started near a dumpster on the exterior of the structure and extended through openings in the loading dock area into the storage area, and then into the main shopping area of the supermarket. The fire progressed to five alarms and involved more than 100 personnel. Fire fighters removed the victim from the structure and transported him to a local hospital where he was pronounced dead.
NIOSH investigators concluded that, to minimize the risk of similar occurrences, fire departments should
- ensure that the department's Standard Operating Procedures (SOPs) are followed and continuous refresher training is provided
- ensure that a proper size-up, using common terminology, is conducted by all fire fighters responsible for reporting interior/exterior conditions to the Incident Commander (IC)
- ensure that pre-incident plans are established and updated on mercantile occupancies in their district
- ensure that fire fighters manage their air supplies as warranted by the size of the structure involved
- instruct and train fire fighters on initiating emergency traffic (Mayday-Mayday) and on the importance of activating their personal alert safety system (PASS) device when they become lost, disoriented, or trapped
- ensure that multiple Rapid Intervention Crews (RIC) are in place when an interior attack is being performed in a large structure with multiple points of entry
- consider placing fire fighter identification emblems on the fire fighters' helmet and turnout gear
- consider placing a bright, narrow-beamed light at all entry portals to a structure to assist lost or disoriented fire fighters in emergency egress
Additionally,
- Building owners should consider upgrading or modifying structures to incorporate new codes and standards to improve occupancy and fire fighter safety.
- Fire departments should consider as a part of their pre-incident planning, educating the public they serve on the importance of building owners, building personnel, or civilians immediately reporting any fire conditions to the first-arriving fire company on the scene.
- Manufacturers and research organizations should conduct research into refining existing and developing new technology to track the movement of fire fighters inside structures.

Aerial view of the incident
INTRODUCTION
On March 15, 2001, the International Association of Fire Fighters (IAFF) and the United States Fire Administration notified the National Institute for Occupational Safety and Health (NIOSH) of the incident. The fire department involved also notified NIOSH of the incident, and the Chief of the department requested that NIOSH evaluate the self-contained breathing apparatuses (SCBAs) worn by the victim and the four injured fire fighters.
During March 25 to April 1, 2001, three occupational safety and health specialists from the NIOSH Fire Fighter Fatality Investigation and Prevention Program and the Chief of the Surveillance and Field Investigations Branch investigated this incident. NIOSH investigators met with the Chief and his staff, the department fire marshal, representatives from the IAFF, a city attorney, and special agents from the Bureau of Alcohol, Tobacco and Firearms. The investigators interviewed officers and fire fighters involved in the incident.
They reviewed the department's standard operating procedures (SOPs), the victim's and injured fire fighters' training records, dispatch tapes and transcripts, tactical and accountability worksheets, and the department's report of the incident. The investigators also reviewed photographs, drawings, and floor plans of the incident site. They conducted a site visit, and the site was photographed and videotaped.
On March 28, 2001, a physical scientist from the NIOSH Division of Respiratory Disease Studies conducted an evaluation of the department's SCBA maintenance program. As part of the investigation, NIOSH agreed to examine and evaluate five 3000 psi, 30-minute, self-contained breathing apparatus (SCBA). These SCBA were last used during interior fire-fighting operations at a structure fire on March 14, 2001. A summary of the report is attached as Appendix I.
A follow-up visit was conducted by the three occupational safety & health specialists during June 18 to 24, 2001, to interview the officers of the command team involved in this incident.
The fire department consists of 1,549 employees, of whom 1,258 are uniformed fire fighters. The department has 45 stations that serve a population of about 1.3 million in a geographical area of approximately 477 square miles.
Training and Experience. The department requires all fire fighters to complete a 12-week basic training program that meets the National Fire Protection Association (NFPA) Level I and Level II certification. The victim had 8 years of fire-fighting experience and NFPA Level I and Level II certification, and he was a certified paramedic. The critically injured fire fighter was a 35-year-old male fire fighter/paramedic with 4 years of experience. Three other fire fighters, who were not critically injured, had the following ages, ranks, and years of experience: a 40-year-old male fire fighter/paramedic, 12 years; a 42-year-old male captain, 15 years; and a 44-year-old male fire fighter, 15 years.
Equipment and Personnel.
1654 Hours—Initial Dispatch (Due to type of call [dumpster fire], only one engine on initial dispatch) Engine 24 (officer, engineer, two fire fighters); Hazmat 4 (engineer [self-dispatched and added to call]).
1658 Hours—Balance 2-1
Engine 21 (officer, engineer, two fire fighters); Engine 14 (officer, engineer, two fire fighters [fatal victim and one non-critically injured fire fighter; engine self-dispatched and added to call]); Ladder 24 (officer, two engineers, one fire fighter); Battalion Chief 3 (chief officer, one assistant); Rescue 21 (two fire fighters [self-dispatched and added to call]); Rescue 25 (two fire fighters). NOTE: This department refers to a rescue unit as an ambulance staffed with certified fire fighters and fire-fighting equipment.
1700 Hours—Balance (Rapid Intervention Crews [RICs] dispatched)
Engine 3 (officer, engineer, two fire fighters); Rescue 3 (two fire fighters [Injured Fire Fighter #1]); Utility Truck 1 (engineer).
1708 Hours—Balance First Alarm
Engine 34 (officer, engineer, two fire fighters); Engine 18 (officer, engineer, two fire fighters); Engine 25 (officer [non-critically injured], engineer, two fire fighters); Engine 15 (officer, engineer, two fire fighters); Engine 4 (officer, engineer, two fire fighters); Engine 725 (officer, engineer, two fire fighters); Engine 710 (officer, engineer, two fire fighters); Ladder 26 (officer, two engineers, one fire fighter); Ladder 9 (officer, two engineers, two fire fighters); Ladder 1 (officer, two engineers, two fire fighters); Battalion Chief 1 (chief officer, one assistant); Communications Van (engineer), Car 957 (safety officer); Car 94 (division chief/safety officer); Car 56 (fire marshal). NOTE: Additional chiefs and district safety officers also responded as a part of the first alarm.
1725 Hours'second-alarm Companies
Engine 30 (officer, engineer, two fire fighters [not critically injured]); Engine 1 (officer, engineer, three fire fighters); Engine 6 (officer, engineer, two fire fighters); Engine 9 (officer, engineer, two fire fighters); Ladder 11 (officer, two engineers, one fire fighter); Ladder 20 (officer, two engineers, one fire fighter); Battalion Chief 5 (chief officer, one assistant); Battalion Chief 2 (chief officer, one assistant); Battalion Chief 4 (chief officer, one assistant); Battalion Chief 6 (chief officer, one assistant).
Additional units were dispatched on subsequent alarms; however, only those units directly involved in the fatal event are discussed in the investigation section of this report.
Structure. The structure was a 27,905-square-foot, L-shaped supermarket that was part of a strip mall (Diagram 1). The structure had a slab concrete foundation and masonry block walls with steel beams and posts. The roof system consisted of open web steel trusses covered with wood, foam, and tar asphalt roofing. The ceiling height throughout the supermarket and lower-level storage area was approximately 20 feet. Second-floor platforms located above the coolers and the first-floor storage areas contained offices and storage areas. The main entrance to the supermarket was located on the east side. The only other doors were a standard 3-foot-wide steel exterior man-door and a 6-foot-wide steel roll-up door located on the south side. The layout of the supermarket is illustrated in Diagram 2. The supermarket was not equipped with a sprinkler system. NOTE: The supermarket originally was constructed outside the city limits. The building was later annexed into the city but was not required to have a sprinkler system installed.
INVESTIGATION
On March 14, 2001, at 1654 hours, Engine 24 responded to a reported exterior cardboard fire at a supermarket. The Hazmat 4 engineer (who was in the area while returning from another call) arrived on the scene at 1657 hours and during initial size-up discovered the cardboard fire with exposure to the building. The engineer also noted that an electrical service drop into the supermarket was directly above the fire (Diagram 1). Hazmat 4 requested that central dispatch balance the alarm to a 2-1, and at 1658 hours, central dispatch balanced the alarm with Engine 21, Ladder 24, Battalion Chief 3 (BC 3), and Rescue 25. Engine 14 and Rescue 21 self-dispatched and responded to the scene.
Engine 24 arrived at 1700 hours, and the captain assumed command (incident commander [IC]). The Hazmat 4 engineer evacuated civilians from the supermarket and surrounding stores in the strip mall. BC 3 arrived on the scene and assumed the IC position and reassigned the Engine 24 captain as the west sector officer. The Engine 24 crew stretched a handline to the south side of the structure to attack the cardboard fire (Photo 1). Because the service drop was arcing, the Engine 24 captain pulled his crew away from the building, and the IC requested central dispatch contact the power company to shut down the power grid.
NOTE: The IC and first-arriving units were unaware that the supermarket was L-shaped and could be accessed from the east and south sides of the building. The east side was the main entrance to the shopping area of the supermarket and the south side-directly behind the clothing and hardware stores-was the location of the man-door and roll-up door entrances to the main storage area of the supermarket (Photo 2).
A supermarket employee stated in a police report that because of the large amount of fire emitting through the man-door and into the structure, he had begun moving propane cylinders and other merchandise away from the door before fire fighters began arriving on the scene. While he was moving the merchandise, the employee became aware that the fire had quickly spread to the interior and into the roof members. According to statements, this information was not reported to the fire fighters upon their arrival.
At 1702 hours, Engine 21 and Engine 14 arrived on the scene, followed by Rescue 25 and Ladder 24 at 1703 hours. Ladder 24 was assigned the roof sector to search for fire extension and to ventilate. Crews from Engine 21 and Rescue 21 checked the clothing and hardware stores for fire extension and civilians. Fire fighters found no fire extension or civilians in either store; however, they found heavy smoke conditions in the rear of the hardware store. The Engine 14 crew, including the victim, were ordered into the east side (front) of the supermarket to check for fire extension and civilians.
At 1707 hours, Engine 3 arrived on the scene as the designated Rapid Intervention Crew (RIC). After the Engine 3 officer reported heavy smoke emitting from the west side of the supermarket, the IC reassigned them to advance a handline into the bakery on the west side to check for fire extension. Because the fire had extended into the structure, the IC requested that central dispatch balance the initial call to a first alarm.
The electrical power to the south side of the building was shutoff, allowing crews to gain access through the roll-up door. The officer from Engine 24 was reassigned as south sector officer after reporting to the IC that heavy smoke was emitting from the wall vents on the west and south sides.
While Engine 14 crew members were searching the supermarket in the main shopping area, they encountered a light haze of smoke banked down to approximately 4 feet below the ceiling. In the produce preparation area, which led into the storage area, they encountered a thick, black smoke accompanied by heat. At 1709 hours, the officer from Engine 14 reported the conditions to the IC and informed him that the Engine 14 crew was stretching a handline into the supermarket.
At 1711 hours, the crew from Engine 14, the officer and two fire fighters from Engine 3, and the crew from Rescue 3 advanced two handlines through the east-side (front) entrance. At 1712 hours, the IC assistant confirmed to the IC that they had a working interior fire. The south sector officer reported to the IC that crews from Rescue 25 and Engine 24 were advancing two handlines through the roll-up door into the storage area, where they encountered heavy smoke banked down to floor level. The IC radioed back a caution that Engine 14 was operating on the opposite side of the storage area and that they should be aware of opposing streams.
At 1714 hours, Engine 14, Engine 3, and Rescue 3 advanced a handline into the produce storage area, and Engine 3 advanced a second handline through the supermarket toward the meat preparation room, which was located along the west wall of the structure (Diagram 2). Conditions in the supermarket deteriorated as the structure began to fill with thick, black smoke. The crew from Engine 14, an officer and fire fighter from Engine 3, and a fire fighter from Rescue 3 were operating in the produce storage area (Photo 3). Another fire fighter from Rescue 3 (Injured Fire Fighter #1) and crew members from Engine 3 were on the second handline in the supermarket. NOTE: The crew from Ladder 24 cut a 6-foot by 6-foot ventilation hole in the roof over the storage area and then exited the roof because they were running low on air.
At approximately 1719 hours, central dispatch notified the IC that 25 minutes had elapsed. Additional crews were arriving on the scene, including the Command Van with support staff. The South Sector officer sent reports of heavy heat and smoke coming from the south-sector interior. At 1725 hours, the IC radioed central dispatch and requested the balance of a second alarm. The IC began assigning on-scene and arriving units to the west exposure and to the east side of the strip mall in preparation for the transition from an offensive to a defensive operation.
The crews from Engine 14, Engine 3, and Rescue 3 told NIOSH investigators that while they were operating in the main supermarket, the produce storage area, and the rear storage area, the heat was intensifying and the thick, black smoke was banked down to floor level. A fire fighter from Rescue 3 and a fire fighter from Engine 3, who were in the main supermarket area, noticed that the fire along the ceiling was intensifying. The crew members from Engine 14 and fire fighters from Engine 3 and Rescue 3, who were operating in the produce storage area, pulled ceiling and searched for fire extension. At this point, the victim told his officer that he was low on air. The officer from Engine 14 pulled his crew together and told them that they would follow the handline as a crew out of the building. Another Engine 14 crew member also reported to the officer that he was low on air.
The engineer who was originally on the nozzle led the exiting crew, followed by the victim, a fire fighter, and the officer. As they were following the handline out of the produce storage area, the victim and the fire fighter following him fell over some debris and became separated from the handline. The officer from Engine 14 - still in the storage area - fell backward over debris and became disoriented, and the officer from Engine 3 put him back on the handline and sent him in the direction of the exit. Meanwhile, the victim and fire fighter from Engine 14, both back on their feet, walked into a wall and fell again. NOTE: It is believed that the victim and the Engine 14 fire fighter had stumbled into the main supermarket shopping area and were moving toward the meat preparation room. As the victim began moving quickly about the shopping area, the fire fighter grabbed his coat to stay with him. Simultaneously, the Engine 14 officer's low-air alarm began to vibrate, and he ran out of air as he approached the east (front) door. As he exited, he encountered the engineer from his crew who had preceded the victim and the fire fighter from Engine 14 on the handline.
The victim and the fire fighter realized they were lost and decided to radio a Mayday. The fire fighter attempted to radio the Mayday, but his transmission was unsuccessful. The victim then successfully radioed the Mayday on his radio. The IC immediately radioed the Engine 18 and Ladder 9 crews and ordered them to assume the RIC duties. Hearing the radio call, the officer from Engine 14 told the officer from Engine 21 to follow the handline to the area where his crew had been operating.
The officer from Engine 14 sent the crew from Engine 21 into the supermarket through the east (front) door to search for the lost fire fighter. NOTE: The Engine 14 officer thought that only one member of his crew was unaccounted for. The fire fighter from Engine 14 became separated from the victim near the meat preparation room. The fire fighter reentered the meat preparation room just as he ran out of air. He heard the radios of other fire fighters (officer and fire fighter from Engine 34) and moved toward them in the main storage area. The fire fighter had become debilitated by the smoke and was assisted out the man-door on the south side of the building by the officer and a fire fighter from Engine 34. Fire fighters assumed that they had rescued the victim; however, once the fire fighter from Engine 14 was removed from the building, fire fighters soon realized that the victim was still inside. The fire fighter from Engine 14 was later transported to a local hospital where he was admitted for treatment of smoke inhalation.
At 1729 hours, the victim radioed a transmission to the crews asking them not to back out because he needed help. The IC radioed back asking for his location. The victim replied that he was in the rear behind something, out of air, and down on the ground sucking in smoke. The IC advised him to stay calm and told him that crews were on their way to assist him. At approximately 1730 hours, the officer from Engine 21 heard someone yelling in the vicinity of the produce storage area. As he followed the voice, he ran into the victim, who was standing near one of the initial attack lines in the main supermarket area. The officer grabbed the victim, asked him to identify himself, and attempted to place him on the handline. The victim, who had removed his regulator from his facepiece because he was out of air, was resistive and reportedly appeared disoriented. On a second attempt, the officer was able to get the victim on his knees and on the handline. Soon after, the victim stood up, turned, and quickly moved toward the rear of the supermarket as the Engine 21 officer attempted to grab him and keep him on the handline. It is believed that the victim headed back toward the meat preparation room. A fire fighter from Rescue 3 who was in the main storage area, upon hearing the victim's voice, headed toward the sound and ran into the victim just outside the swinging door that led from the main storage area into the meat preparation room. The victim told the Rescue 3 fire fighter that he was out of air, and the fire fighter told him to stay calm and follow him. The victim turned and headed away from the fire fighter toward the meat preparation room as the fire fighter grabbed the victim and told him that he was going the wrong way. As the victim turned, he knocked the Rescue 3 fire fighter down and the two became separated. Returning to his feet, the fire fighter tried to find the victim but ran out of air and was forced to leave the building.
NOTE: During this time, the IC made numerous attempts to contact the victim to tell him to activate his Personal Alert Safety System (PASS); however, the victim did not respond. Injured Fire Fighter #1, who was low on air, was about to exit when he heard the victim's voice coming from the direction of the meat preparation room. He followed the victim's voice until he met up with the victim in the meat preparation area. Injured Fire Fighter #1 radioed the IC at 1734 hours that he had found the victim, that they were by themselves, and that they were both out of air. Injured Fire Fighter #1 ran out of air, partially removed his facepiece, and pulled his hood over his face. NOTE: At this point, Injured Fire Fighter #1 was near the meat cooler while the victim was about 8 feet away in the meat preparation room (Diagram 3). The victim's PASS was not sounding at this time. At 1735 hours, the IC ordered fire fighters to break out (ventilate) the windows on the east (front) side.
At 1736 hours, the IC believed that the victim had been rescued and removed from the building. This "victim" was really the fire fighter from Engine 14 who had been with the victim. The IC ordered all fire fighters out of the building because he ordered fire-fighting operations to change from offensive to defensive. Note: After crews exited the building, flames engulfed the east side of the supermarket, preventing any further entry through the east (front) door. From this point forward, all rescue crews entered and exited through the two doors on the south side of the building. Safety officers posted at the man-door and roll-up door controlled access and assignments of rescue crews. The officer from Engine 25, now operating in the main storage area, followed a path to the meat cooler and found Injured Fire Fighter #1 (Diagram 3 and Photo 4). The officer radioed the IC that he had one fire fighter down and that he needed assistance. The officer made a second transmission that he and his crew had found the victim and that they were bringing him out. NOTE: When the Engine 25 officer referred to Injured Fire Fighter #1 as "one fire fighter down," his crew and IC believed that he was referring to the victim, not another downed fire fighter. The officer passed Injured Fire Fighter #1 to his crew in the main storage area, and they took him out of the building through one of the doors on the south side. Note: A fire fighter, who was among the fire fighters outside the building, recognized that Injured Fire Fighter #1 was not the victim. The officers and IC then realized that the victim was still inside. At 1739 hours, the IC ordered all fire fighters off the roof and out of the building because they were going defensive as soon as the victim was out. NOTE: Before the Engine 25 officer passed Injured Fire Fighter #1 to his crew, Injured Fire Fighter #1 told the officer that the victim was nearby. As the IC was ordering fire fighters out, the Engine 25 officer located the victim in the meat preparation room. The victim was unresponsive, and his PASS device was sounding. The Engine 25 officer, who was alone with the victim, made an emergency transmission that was not received by the IC. At 1740 hours, an officer from Engine 4 heard the transmission and radioed that a fire fighter was down in the southwest corner. The Engine 25 officer, unable to move the victim, ran out of air, removed his facepiece and regulator, and attempted to crawl out of the building. Simultaneously, crews from Engine 6 and Engine 710 entered the south side of the building and proceeded toward the produce storage area. As crew members from Engine 6 neared the produce storage area, they heard a PASS device sounding from their left (meat preparation room). The Engine 6 crew encountered the officer from Engine 25 (his PASS device was not sounding) and passed him to the Engine 710 crew, who assisted him out of the building. The Engine 25 officer, the third fire fighter to become injured, was transported to a local hospital and treated for smoke inhalation.
The Engine 6 crew continued toward the sounding PASS device and found the victim lying unconscious on his back with his facepiece partially removed. They checked the victim for a pulse and could not find one.
Numerous crews participated in the removal of the victim from the building. Fire fighters were hampered in their removal efforts by the victim's size (he was 6 feet, 4 inches tall, and he weighed about 289 pounds [in addition to the weight of his gear]) and the amount of debris blocking their path through the main storage area to the south-side roll-up door. Approximately 19 minutes elapsed from the point when fire fighters found the unconscious victim to the point when the victim was removed from the building. Fire fighters immediately began cardiopulmonary resuscitation (CPR) and advanced life support (ALS) on the victim at the scene.
Injured Fire Fighter #1 (the critically injured fire fighter from Rescue 3), was transported to a local hospital for treatment of smoke inhalation. At the hospital, his carboxyhemoglobin level was measured at 29 percent. Three other fire fighters who had suffered smoke inhalation-a fire fighter from Engine 14, an officer from Engine 25, and a fire fighter from Engine 30-were treated at a local hospital and released.
CAUSE OF DEATH
The medical examiner listed the victim's cause of death as thermal burns and smoke inhalation. The victim's carboxyhemoglobin level was listed at 61 percent at the time of death.
RECOMMENDATIONS/DISCUSSION
Recommendation #1: Fire departments should ensure that the department's Standard Operating Procedures (SOPs) are followed and continuous refresher training is provided. 1
Discussion: The purpose of the department's SOP is to account for all fire fighters on the fireground. This SOP provides the command staff a means to track and account for all fire fighters. The following guidelines within this SOP should be followed:
- All companies should follow orders, stay together, and report any changes to the Incident Commander. This will allow the Incident Commander to maintain an accurate tracking and awareness of where resources are committed at an incident and the accountability of all personnel.
- Sector officers are assigned as needed and the sector officers respond accordingly. Sector officers are responsible for maintaining an accurate tracking and awareness of crews assigned to them. This will require the sector officer to be in his/her assigned area and maintaining close supervision of assigned crews.
- Company officers shall maintain a current electronic roster of personnel responding on the apparatus.
- All crews will work for Command or Sectors - no free-lancing.
- Crews arriving on the scene should remain intact. Two or more members will be considered a minimum crew size. Each member must have a radio.
- All crews entering a hot zone must have a supervisor.
- All crews will go in together, stay together, and come out together. Reduced visibility and increased risk will require very tight togetherness.
- The IC is immediately notified of any fire fighters who are not accounted for.
- Fire conditions and strategies are continuously evaluated.
- Fire fighters make clear reports when a May Day is transmitted.
- Lost or trapped fire fighters manually activate their PASS device.
- Fire fighters always remain in contact with the hoseline or lifeline and use it as a guide to exit.
- Fire companies should complete pre-incident plans.
Refresher training should be provided to all fire fighters on a regular basis or as needed when changes are made to the department's SOPs.
Recommendation #2: Fire departments should ensure that a proper size-up, using common terminology, is conducted by all fire fighters responsible for reporting interior/exterior conditions to the Incident Commander (IC). 1, 2
Discussion: A size-up should be a systematic process to determine the critical fireground factors that lead to the strategy and development of attack. The size-up should consist of observing the fireground factors, a risk management plan, determining the proper strategy, developing an Incident Action Plan (IAP) and the deployment of personnel. A proper size-up can only be conducted by fire fighters that are trained to identify a common understanding of fire conditions (interior/exterior) and are able to communicate the findings using standardized terminology that is understood by all fire fighters. The size-up should not be delayed or be a time-consuming process but should continue throughout operations. The initial size-up will provide information to the IC that will be crucial for determining the appropriate action.
When dealing with large structures, such as a strip mall, all fire fighters should conduct their own size-up for their personal safety. When conducting a size- up, all fire fighters should be aware and report to the IC any condition or variable that could possibly affect the strategy. For example, when the roof crew gets on the roof and finds that the building incorporates a fire wall, the officer or fire fighters should immediately radio the IC and report where the fire wall is and where it goes. This will provide information to help the IC determine the layout of the interior sections of the large structure or in this case, strip mall.
Just as importantly, an interior size-up should be conducted by an officer or senior fire fighter and reported to the IC. Since the IC is staged at the command post (outside), the interior conditions should be communicated as soon as possible to the IC. Interior conditions could change the IC's strategy or tactics. For example, if heavy smoke is emitting from the exterior roof system, but fire fighters cannot find any fire in the interior, it is a good possibility that the fire is above them in the roof system. It is important for the Incident Commander to immediately obtain this type of information to help make the proper decisions.
A proper size-up begins from the moment the alarm is received, and it continues until the fire is under control. Several factors must be evaluated in conducting the size-up—e.g., type of structure, time of day, contents of the structure, potential hazards, etc. The size-up should also include risk versus gain during incident operations. The following factors are important considerations:
- Occupancy type involved and rescue possibilities. The type of occupancy can have a great effect on the aspects of the fire attack. The type of occupancy could assist in determining the structure's layout, hazardous materials, and the possibility of civilians (e.g., civilians will be present in a hospital around the clock).
- Smoke conditions. The smoke conditions can provide the Incident Commander with additional information about the fire. For example, if the fire is in the roof and burning roofing materials, the smoke would probably appear to be thick and black.
- Type of construction. The type of construction will be one of the most important areas to identify. The type of structure could provide the Incident Commander information such as how the building may hold up under fire conditions or if the building is generally subject to collapse under fire conditions.
- Type of roof system. The roof system should be one of the first things that is determined before fire fighters enter a burning structure. One type of roof system is the lightweight truss roof. The structural goal of the lightweight truss is to distribute loads over a large area.
- Age of structure. The Incident Commander should ascertain the age of the building when determining strategy or tactics. The age of the structure can provide the Incident Commander with information to help determine the building's integrity or other vital information such as construction methods or construction materials.
- Exposures. The Incident Commander should evaluate the whole picture. The protection of exposures near or connected to a burning building should be included in the strategic plan.
- Time considerations. Information such as time of incident, time fire was burning before arrival, time fire was burning after arrival, and type of attack, is some of the most important information the Incident Commander should have.
Recommendation #3: Fire Departments should ensure that pre-incident plans are established and updated on mercantile occupancies in their district. 3
Discussion: NFPA 1620 states that "Pre-incident planning in a mercantile occupancy involves not only the emergency responders, but administrators, section or department supervisors, and other staff members." The primary purpose of a pre-incident plan is to help responding personnel effectively manage emergencies with available resources. Pre-incident planning involves identifying the protection systems, building construction, contents, and operating procedures that can impact emergency operations. The construction of the building in terms of the size of the building (both vertical and horizontal), building features (fire walls, fire barriers, roofs, and floors), access points, areas where products of combustion could spread due to a lack of structural barriers (e.g., stock areas), and building services, should be determined. Strip shopping centers or rows of attached mercantile occupancies have common walls.
Most occupancies present an ever-changing environment making ongoing maintenance of the pre-incident plan as critical as the original development of the plan. Where conditions indicate that a change in a pre-incident plan is warranted, the plan should be updated and distributed to the appropriate persons and agencies.
A system to utilize the pre-incident plan should be designed to allow access to the plan, or a summary with key elements of the plan, while in route and during the incident. Some supplemental detailed information such as building plans can be kept in a lock box or other secured area.
Recommendation #4: Fire departments should ensure that fire fighters manage their air supplies as warranted by the size of the structure involved. 4
Discussion: Air consumption will vary with each individual's physical condition, the level of training, the task performed, and the environment. Depending on the individual's air consumption and the amount of time required to exit a hostile environment, the low air alarm may not provide adequate time to exit. Working in large structures (high rise buildings, warehouses, and supermarkets) require that fire fighters be cognizant of the distance traveled and the time required to reach the point of suppression activity from the point of entry. When conditions deteriorate and the visibility becomes limited, firefighters may find that it takes additional time to exit when compared to the time it took to enter the structure.
Recommendation #5: Fire Departments should instruct and train fire fighters on initiating emergency traffic (Mayday-Mayday) and on the importance of activating their personal alert safety system (PASS) device when they become lost, disoriented, or trapped. 5
Discussion: As soon as a fire fighter becomes lost or disoriented, trapped or unsuccessful at finding his/her way out of a hazardous situation (e.g., interior of structure fire), he/she must recognize that fact and initiate emergency traffic. He/she should manually activate his/her personal alert safety system (PASS) device and announce "Mayday-Mayday" over the radio. A "Mayday-Mayday" call will receive the highest communications priority from Dispatch, Incident Command, and all other units. The sooner Incident Command is notified and a RIC is activated, the greater the chance of the fire fighter being rescued. Fire fighters should initiate emergency traffic while they are still capable and not wait until they are too weak or low on air to call for help.
Recommendation #6: Fire departments should ensure that multiple Rapid Intervention Crews (RIC) are in place when an interior attack is being performed in a large structure with multiple points of entry. 6, 7
Discussion: Typically, a RIC is designated to stand by and monitor activity in case an emergency situation should occur. A RIC should consist of at least two fire fighters and should be available for rescue of a fire fighter or a team if the need arises. It would be ideal to have a full company or a minimum of four fire fighters make up the RIC; however, this may not be possible due to staffing issues. In large structures, multiple RICs should be established and possibly positioned in different sectors. When RICs enter large structures, they may use the majority of their air supply trying to locate an injured, down, or disoriented fire fighter. For this reason, backup RICs should be in place to replace the initial RIC when they exit. The RICs should be fully equipped with the appropriate protective clothing, protective equipment, SCBA, and any specialized rescue equipment that might be needed, given the specifics of the operation underway. Once a RIC is established, they should remain the RIC throughout the operation. They should constantly survey the fireground operations and be in communication at all times with the IC and companies on the fireground. As fireground operations continue, the RIC teams should observe the following:
- where fire fighters are entering and exiting
- how many fire fighters are inside
- where the fire fighters are operating
- what operations are taking place
- the layout of the structure
- the structure (i.e., trussed roof, metal roof, etc.) and hazards that could exist with the structure (i.e., possible collapse areas, etc.)
- hazards they might encounter (i.e., chemicals, tanks, etc.)
- the fire's condition (i.e., fire spread, fire in the roof, etc.)
- if an emergency occurs, what will be their best route to enter or exit
- what equipment they will need if an emergency occurs (i.e., airbags, hydraulic jacks, additional air bottles, etc.)
Each incident is different, and additional concerns should also be taken into consideration. Many functions are expected from the RIC members during an incident. If an emergency occurs, the RIC(s) should have full air bottles, a good understanding of the overall situation, and be able to respond in a safe manner to perform the search or rescue. If the RIC is used for an emergency operation, a second RIC should be put in place in case an additional emergency should occur. Note: Fire departments should ensure that they assess all risk factors when making the decision to send a RIC into a structure that has already been the scene of an emergency evacuation, search, or rescue.
- Fire fighters should consider using a hose line or a rope bag with luminescent lights to mark a victim's location if an injured or down fire fighter cannot be removed and fire fighters have to exit without the victim.
A part of the RIC's equipment should be a hose line or rope bag with luminescent lights. When an injured or down fire fighter is located by a RIC and they cannot remove the fire fighter, a hose line or rope bag with luminescent lights could be used to mark the victim's location for other RICs to follow. If the victim's PASS device has been turned off to protect communications, the RICs should ensure that the PASS is reactivated when rotating out.
- Fire departments should ensure that fire fighters receive continuous training for search-and-rescue operations.
RICs will be mostly responsible for search-and-rescue operations; however, it may be hard to predict who the RIC will be in some cases. For this reason all fire fighters should be familiar with the RIC operations and the different situations they may encounter. Fire fighters should be given training to save other fire fighters and/or themselves in emergency situations. When a fire fighter becomes injured, low on air, disoriented, or is exposed to high levels of carbon monoxide, it is hard to predict how the fire fighter may react. This should be covered in the training and a plan of action should be developed and implemented to deal with such rescues. Alternatively if staffing is available, fire departments should designate rescue companies whose main purpose on the fireground is to support fire operations and conduct search and rescue of fire fighters.
Recommendation #7: Fire departments should consider placing fire fighter identification emblems on the fire fighters' helmet and turnout gear. 8
Discussion: When fire fighters enter smoke-filled structures the visibility is usually very poor, thereby reducing the possibilities of easily identifying each other. Some fire departments color code their helmets so fire fighters, officers, or the chief can be easily identified on the fireground. Fire departments can also use name, number, or company emblems to identify each individual fire fighter on the fireground. This could assist fire fighters on the fireground to identify a lost or disoriented fire fighter.
The fire department involved in this incident provides station uniforms (T-shirts) that are labeled with each fire fighter's name. During this incident, rescue crews removed the T-shirts from the unconscious fire fighter (Injured Fire Fighter #1), making it difficult to determine who the rescued fire fighters were.
Recommendation #8: Fire departments should consider placing a bright, narrow-beamed light at all entry portals to a structure to assist lost or disoriented fire fighters in emergency egress. 9
Discussion: In a dark, smoky environment, fire fighters often become lost or disoriented, and all too often they are unable to escape. A bright, narrow-beamed light at the entry point could possibly assist fire fighters in emergency egress situations, i.e., when lost or disoriented. Past NIOSH investigations have revealed that a light placed at the entry portals assisted some fire fighters in emergency egress situations.
Additionally,
Recommendation #9: Building owners should consider upgrading or modifying structures to incorporate new codes and standards to improve occupancy and fire fighter safety. 10
Discussion: Building codes and standards have been developed which are used as guidelines for new building design and construction. Unfortunately, before municipalities adopted or enforced specific codes and standards, many buildings were designed and constructed without incorporating such standards. New or improved codes have been established which can improve the safety of existing structures. Sprinkler systems are one specific area of concern for large structures. It is proven that sprinkler systems reduce the loss of property and life. There is also a strong possibility that sprinklers could reduce fire fighter fatalities since they contain, and even extinguish, fires before the arrival of the fire department. Sprinklers are currently the most proactive fire safety approach in building construction. The structure involved in this incident did not have a sprinkler system.
Recommendation #10: Fire departments should consider as part of their pre-incident planning, educating the public they serve on the importance of building owners, building personnel, or civilians immediately reporting any fire conditions to the first-arriving fire company on the scene. 1, 3
Discussion: Fire growth or conditions is one of the most important pieces of information for the first- arriving fire company on the scene of any fire. If possible, the person who witnessed the fire should stand by in a safe location until the first arriving fire company arrives on the scene. NFPA 1620, 2-3.3, suggests that the pre-incident plan should provide for available facility personnel to advise responding personnel of current conditions upon arrival. The current conditions reported would include; the location of the fire, the approximate time the fire started, the fire's growth, the fire's condition, and if possible, the layout of the structure. This will help the fire fighters decide their tactics and strategy to attack the fire.
The standard operating procedures for this department recommend that fire companies should complete pre-incident plans.
In this incident, a supermarket employee had witnessed the fire and begun removing items from the rear storeroom as the fire department responded. The witness removed several items from the storeroom before seeing the fire go up the wall and into the ceiling. The witness then exited, and seeing that the fire department had arrived, did not report the conditions to any fire department personnel.
Recommendation #11: Manufacturers and research organizations should conduct research into refining existing and developing new technology to track the movement of fire fighters inside structures. 11
Discussion: Fire fighter fatalities often are the result of fire fighters becoming lost or disoriented on the fireground. The use of systems for locating lost or disoriented fire fighters could be instrumental in reducing the number of fire fighter deaths on the fireground. One such system, a wireless tracking system, requires locating three accurately placed spread-spectrum transmitters around a building to provide positioning information. Other systems may include a UHF Radio system or an Infrasound Low Frequency Detector. Research into refining existing systems and developing new technologies for tracking the movement of fire fighters on the fireground should continue.
REFERENCES
- Arizona Fire Department [2000]. Written standard operating procedures.
- Brunacini A [1985]. Fire command. Quincy, MA: National Fire Protection Association.
- NFPA [1998]. NFPA 1620: Recommended practice for pre-incident planning. Quincy, MA: National Fire Protection Association.
- Fire Fighter's Handbook [2000]. Essentials of fire fighting and emergency response. New York: Delmar Publishers.
- Hoffman, JJ [2002]. MAYDAY-MAYDAY-MAYDAY. Fire Department Safety Officers Association Health and Safety for Fire and Emergency Service Personnel 13(4):8.
- NFPA [1997]. NFPA 1500: Standard on fire department occupational safety and health program. Quincy, MA: National Fire Protection Association.
- Olson, JB [1998]. "Aware": A life saving plan for rescuing trapped firefighters. Fire Engineering 151(12):52-58.
- National Institute for Occupational Safety and Health [1999]. Two fire fighters die and two are injured in townhouse fire—District of Columbia. DHHS (NIOSH) Fire Fighter Fatality Report 99F-21.
- National Institute for Occupational Safety and Health [1998]. Commercial structure fire claims the life of one fire fighter—California. DHHS (NIOSH) Fire Fighter Fatality Report 98F-07.
- NFPA Fire Analysis Division [1987]. Automatic sprinkler systems do have an impact in industry. Fire Journal 81(1):39-40.
- National Institute for Occupational Safety and Health [2000]. Six career fire fighters killed in cold-storage and warehouse building fire—Massachusetts. DHHS (NIOSH) Fire Fighter Fatality Report 99F-47.
INVESTIGATOR INFORMATION
This investigation was conducted by Frank Washenitz, Tom Mezzonotte, and Mark McFall, Safety and Occupational Health Specialists; and Dawn Castillo, Chief, Surveillance and Field Investigations Branch, Division of Safety Research NIOSH.
Diagram 1. Strip Mall Layout
Diagram 2. Supermarket Layout
Diagram 3. Meat Preparation Room Section
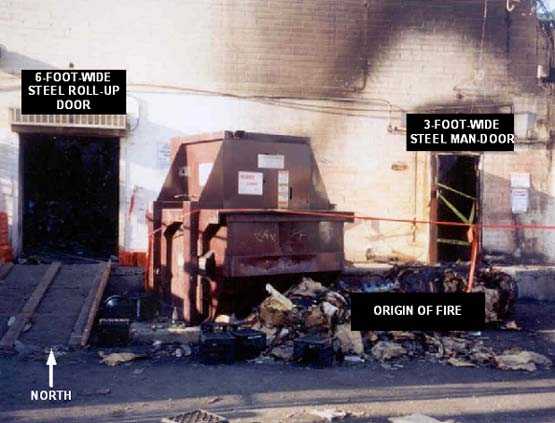
Photo 1. South Entrances of Supermarket

Photo 2. Main Storage Room
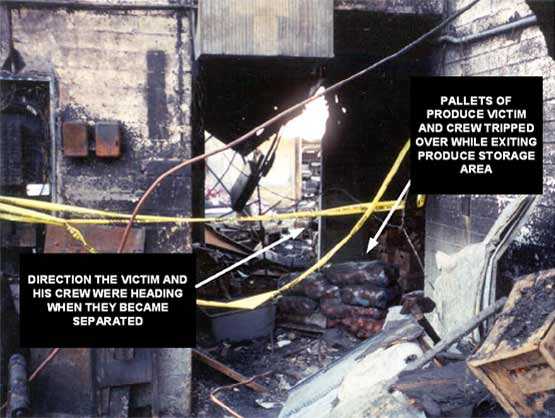
Photo 3. View of Produce Storage Area

Photo 4. Meat Preparation Room
APPENDIX I
The following appendix is a summary of NIOSH Task No. TN-11895. For a full report, including photos, tables, and diagrams, contact NIOSH, Division of Respiratory Disease Studies, Respirator Branch at (304) 285-5907.
Investigator Information
The SCBA inspections and performance tests were conducted by and this report was written by Thomas McDowell, General Engineer, Respirator Branch, National Personal Protective Technology Laboratory, National Institute for Occupational Safety and Health, located in Morgantown, West Virginia.
Background
As part of the National Institute for Occupational Safety and Health (NIOSH) Fire Fighter Fatality Investigation and Prevention Program, the Respirator Branch agreed to examine and evaluate five Scott Health & Safety (Scott) 3000 psi, 30-minute, self-contained breathing apparatus (SCBA). These SCBA were last used during interior firefighting operations at a structure fire on March 14, 2001.
This SCBA status investigation was assigned NIOSH Task Number TN-11895.
Two of the five SCBA, each secured in its own black carrying case, were delivered to the NIOSH Appalachian Laboratory for Occupational Safety and Health (ALOSH) by representatives of the fire department on March 21, 2001. The remaining three SCBA were shipped to NIOSH via Federal Express. The three SCBA, also in individual carrying cases, arrived at NIOSH on May 23, 2001. Upon arrival, all five SCBA were taken to the Firefighter SCBA Evaluation Lab (Room 1520) and were stored under lock until the time of the evaluations.
SCBA Inspections
The contents of each SCBA carrying case were inspected by Thomas McDowell, General Engineer, of the Respirator Branch, National Personal Protective Technology Laboratory (NPPTL), NIOSH. Each case contained one Scott Air-Pak® 3.0 SCBA. The SCBA were examined individually, component by component, in the condition as received to determine their conformance to the NIOSH-approved configuration. The entire inspection process was videotaped.
The first case from the fire department was opened on March 21, 2001, in Room 1520 of the ALOSH Building. The inspection of the first SCBA (referred to as Unit #1 [victim's unit]) was completed that day. The inspection of Unit #1 was witnessed by the representatives from the fire department. The second case was opened later that same day. The inspection of Unit #2 (Injured Fire Fighter #1) was initiated after the representatives from the fire department had left for the day. The inspection of Unit #2 was completed on April 27, 2001. The third unit was removed from its case and inspected on July 2, 2001. Unit #4 was removed from its case and inspected on July 3. The fifth unit was removed from its case and inspected on July 9.
SCBA Testing
Testing of Unit #1 was initiated on March 22, 2001. The representatives from the fire department witnessed the six performance tests that were completed that day. A seventh performance test (the Exhalation Breathing Resistance Test) was conducted on Unit #1 the following day after the representatives returned home. Performance testing of Unit #2 was initiated and completed on April 30, 2001. Unit #3 was tested on July 10 and 13, 2001. Unit #4 was tested on July 11 and 13. Unit #5 was tested on July 12 and 13.
The five SCBA were tested in the conditions as received from the City of Phoenix Fire Department with the following noted exceptions:
- Unit #2 was delivered to NIOSH with two regulators. The regulator identified as belonging to Unit #3 was attached to the regulator hose on Unit #2. The regulator identified as belonging to Unit #2 was attached to the Unit #2 facepiece. At the time of the inspection of Unit #2, the Unit #3 regulator was disconnected from the Unit #2 regulator hose and stored in Room 1520 until the time it was inspected along with the other components of Unit #3. The Unit #3 regulator was used during the testing of Unit #3.
- The compressed air cylinder on Unit #3 was found to be too damaged to safely pressurize. Therefore, the undamaged compressed air cylinder from Unit #4 was used during the performance testing of Unit #3.
- Unit #5 was shipped to NIOSH without a compressed air cylinder. The compressed air cylinder from Unit #4 was used during the performance testing of Unit #5.
The purpose of the testing was to determine each SCBA's conformance to the approval performance requirements of Title 42, Code of Federal Regulations, Part 84 (42 CFR 84). Further testing was conducted to provide an indication of each SCBA's conformance to the National Fire Protection Association (NFPA) Air Flow Performance requirements of NFPA 1981 - Standard on Open-Circuit Self-Contained Breathing Apparatus for the Fire Service, 1997 Edition.
The following performance tests were conducted on each of the five SCBA:
NIOSH SCBA Certification Tests (in accordance with the performance requirements of 42 CFR 84):
- Positive Pressure Test [42 CFR 84.70(a)(2)(ii)]
- Rated Service Time Test (duration) [42 CFR 84.95]
- Gas Flow Test [42 CFR 84.93]
- Exhalation Breathing Resistance Test [42 CFR 84.91(c)]
- Static Facepiece Pressure Test [42 CFR 84.91(d)]
- Remaining Service Life Indicator Test (low-air alarm) [42 CFR 84.83(f)]
National Fire Protection Association (NFPA) Tests (in accordance with NFPA 1981, 1997 Edition):
- Air Flow Performance Test [NFPA 1981, Chapter 6, 6-1]
SCBA Test Results
Each of the five SCBA met the requirements of all six selected NIOSH tests performed. Additionally, all five SCBA met the facepiece pressure requirements of the NFPA Air Flow Performance Test.
Personal Alert Safety System (PASS) Devices
Each of the five SCBA was equipped with an integrated Personal Alert Safety System (PASS) device. During the SCBA evaluations, the PASS devices were activated both manually and automatically. The PASS device on Unit #2 did not function. The PASS devices on Units #1, #3, #4, and #5 appeared to function properly in both modes. Because NIOSH does not test or certify PASS devices, no further testing or evaluations were conducted on the PASS units.
Summary and Conclusions
Five SCBA were submitted to NIOSH by the fire department involved in this incident for evaluation. Two of the SCBA were delivered to NIOSH on March 21, 2001. The other three units were shipped to NIOSH via Federal Express. The three units arrived at NIOSH on May 23, 2001. The SCBA inspections were initiated on March 21, 2001. The inspection of the last of the five SCBA was completed on July 9, 2001. All five units were identified as Scott Air-Pak 3.0, 30-minute, 3000 psi, SCBA (NIOSH approval number TC-13F-366). All five SCBA have the appearance of having seen considerable use. However, with the exception of the compressed air cylinder on Unit #3, all components on the five units were in good shape and functional. The SCBA were determined to be in a condition safe for testing.
The five units were each subjected to a series of seven performance tests. Testing began on March 22, 2001, and was completed on July 13, 2001. No maintenance or repair work was performed on the SCBA at any time. Because the compressed air cylinder on Units #3 was damaged, and because Unit #5 was shipped to NIOSH without a compressed air cylinder, the cylinder from Unit #4 was used during all performance tests on Units #3, #4, and #5. All five SCBA met the requirements of all six selected NIOSH tests performed. Additionally, all five SCBA met the facepiece pressure requirements of the NFPA Air Flow Performance Test.
In light of the information obtained during this investigation, the Institute has proposed no further action at this time. Following inspection and testing, the five SCBA were returned to their carrying cases, sealed, photographed, and then returned to the Arizona fire department via Federal Express. The SCBA were shipped from NIOSH on July 13, 2001.
This page was last updated on 8/06/02
- Page last reviewed: November 18, 2015
- Page last updated: October 15, 2014
- Content source:
- National Institute for Occupational Safety and Health Division of Safety Research