


Six Career Fire Fighters Killed in Cold-Storage and Warehouse Building Fire - Massachusetts
 ShareCompartir
ShareCompartir
 Death in the Line of Duty...A summary of a NIOSH fire fighter fatality investigation
Death in the Line of Duty...A summary of a NIOSH fire fighter fatality investigation
F99-47 Date Released: September 27, 2000
SUMMARY
On December 3, 1999, six career fire fighters died after they became lost in a six-floor, maze-like, cold-storage and warehouse building while searching for two homeless people and fire extension. It is presumed that the homeless people had accidentally started the fire on the second floor sometime between 1630 and 1745 hours and then left the building. An off-duty police officer who was driving by called Central Dispatch and reported that smoke was coming from the top of the building. When the first alarm was struck at 1815 hours, the fire had been in progress for about 30 to 90 minutes. Beginning with the first alarm, a total of five alarms were struck over a span of 1 hour and 13 minutes, with the fifth called in at 1928 hours. Responding were 16 apparatus, including 11 engines, 3 ladders, 1 rescue, and 1 aerial scope, and a total of 73 fire fighters. Two incident commanders (IC#1 and IC#2) in two separate cars also responded.
Fire fighters from the apparatus responding on the first alarm were ordered to search the building for homeless people and fire extension. During the search efforts, two fire fighters (Victims 1 and 2) became lost, and at 1847 hours, one of them sounded an emergency message. A head count ordered by Interior Command confirmed which fire fighters were missing.
Fire fighters who had responded on the first and third alarms were then ordered to conduct search-and-rescue operations for Victims 1 and 2 and the homeless people. During these efforts, four more fire fighters became lost. Two fire fighters (Victims 3 and 4) became disoriented and could not locate their way out of the building. At 1910 hours, one of the fire fighters radioed Command that they needed help finding their way out and that they were running out of air. Four minutes later he radioed again for help. Two other fire fighters (Visctims 5 and 6) did not make initial contact with command nor anyone at the scene, and were not seen entering the building. However, according to the Central Dispatch transcripts, they may have joined Victims 3 and 4 on the fifth floor. At 1924 hours, IC#2 called for a head count and determined that six fire fighters were now missing. At 1949 hours, the crew from Engine 8 radioed that they were on the fourth floor and that the structural integrity of the building had been compromised. At 1952 hours, a member from the Fire Investigations Unit reported to the Chief that heavy fire had just vented through the roof on the C side. At 2000 hours, Interior Command ordered all companies out of the building, and a series of short horn blasts were sounded to signal the evacuation. Fire fighting operations changed from an offensive attack, including search and rescue, to a defensive attack with the use of heavy-stream appliances. After the fire had been knocked down, search-and-recovery operations commenced until recall of the box alarm 8 days later on December 11, 1999, at 2227 hours, when all six fire fighters' bodies had been recovered. NIOSH investigators concluded that, to minimize the risk of similar occurrences, fire departments should
ensure that inspections of vacant buildings and pre-fire planning are conducted which cover all potential hazards, structural building materials (type and age), and renovations that may be encountered during a fire, so that the Incident Commander will have the necessary structural information to make informed decisions and implement an appropriate plan of attack
ensure that the incident command system is fully implemented at the fire scene
ensure that a separate Incident Safety Officer, independent from the Incident Commander, is appointed when activities, size of fire, or need occurs, such as during multiple alarm fires, or responds automatically to pre-designated fires
ensure that standard operating procedures (SOPs) and equipment are adequate and sufficient to support the volume of radio traffic at multiple-alarm fires
ensure that Incident Command always maintains close accountability for all personnel at the fire scene
use guide ropes/tag lines securely attached to permanent objects at entry portals and place high-intensity floodlights at entry portals to assist lost or disoriented fire fighters in emergency escape
ensure that a Rapid Intervention Team is established and in position upon their arrival at the fire scene
implement an overall health and safety program such as the one recommended in NFPA 1500, Standard on Fire Department Occupational Safety and Health Program
consider using a marking system when conducting searches
identify dangerous vacant buildings by affixing warning placards to entrance doorways or other openings where fire fighters may enter
ensure that officers enforce and fire fighters follow the mandatory mask rule per administrative guidelines established by the department
explore the use of thermal imaging cameras to locate lost or downed fire fighters and civilians in fire environments
In addition,
manufacturers and research organizations should conduct research into refining existing and developing new technology to track the movement of fire fighters on the fireground.
INTRODUCTION
On December 3, 1999, six male career fire fighters, ages 34, 38, 38, 41, 42, and 51 (the victims) died after becoming lost in a cold-storage and warehouse building fire. On December 4, 1999, the liaison from the fire department involved in this incident and the International Association of Fire Fighters (IAFF) notified the National Institute for Occupational Safety and Health (NIOSH) of the incident. On December 5, 1999, a Safety and Occupational Health Specialist, the Senior Fire Fighter Investigator, and the Team Leader from the NIOSH Fire Fighter Fatality Investigation and Prevention Program traveled to the incident site to conduct an investigation. A second investigation team consisting of the Team Leader and three Safety and Occupational Health Specialists conducted a second investigation during the week of January 3-7, 2000. During the week of April 17, a third trip was completed by the Team Leader to finalize details of the prior two investigations, and an engineer and physical scientist from the NIOSH Respirator Branch conducted a Self-Contained Breathing Apparatus maintenance evaluation at the request of the Fire Chief (see Attachment). The incident was reviewed with the Chief, the Safety Officer, the Division Chief, the Deputy Chief and fire fighters from the Fire Department involved. The incident was also reviewed with a representative of the IAFF, a representative of the Professional Fire Fighters of Massachusetts, the State Fire Marshal, the Coroner, the District Attorney's representative, and the State Police. The incident site was visited on three separate occasions, photographs of the incident site were obtained, and the medical examiner's report was requested. Dispatch transcription records, standard operating procedures, building drawings, and the victim's training records were also obtained from the Fire Department. NIOSH investigators also completed a walk-through tour of a cold-storage warehouse similar to the one involved in the incident.
The Fire Department involved in the incident serves a population of 170,000 in a geographic area of 39.4 square miles and is comprised of 479 uniformed personnel and 12 fire stations. The Fire Department requires 480 hours of training, which includes 80 hours of hazardous materials training and a written test to become certified as Fire Fighter I and II. The training is designed to cover personal safety, forcible entry, ventilation, fire apparatus, ladders, self-contained breathing apparatus, hose loads, streams, hazardous materials, structure fire, pumps, repelling, search and rescue, terrorism, vehicle extraction, cardiopulmonary resuscitation, first aid, aerial operations, water and ice rescue, scuba diving, and electrical emergencies. The victims had 12 years, 5 months; 2 years, 1 month; 8 years, 9 months; 16 years, 5 months; 20 years, 3 months; and 27 years of fire fighting experience respectively.
Although 21 pieces of fire apparatus and over 73 personnel were involved in this incident, only those directly involved up to the time of the fatal incident are mentioned in this report. Table 2 provides a summary of the time line, apparatus, and personnel dispatched for each of the fire alarms for this fire.
WEATHER INFORMATION
Weather conditions during the major events of this incident (from 1600 to 2100 hours) were as follows: Wind was from the southwest at 7.5 mph and surface visibility was unlimited. The sky, overcast with broken clouds, was clear by 2100 hours. The temperature was 45 degrees Fahrenheit, and the relative humidity was 37 percent.
BUILDING INFORMATION
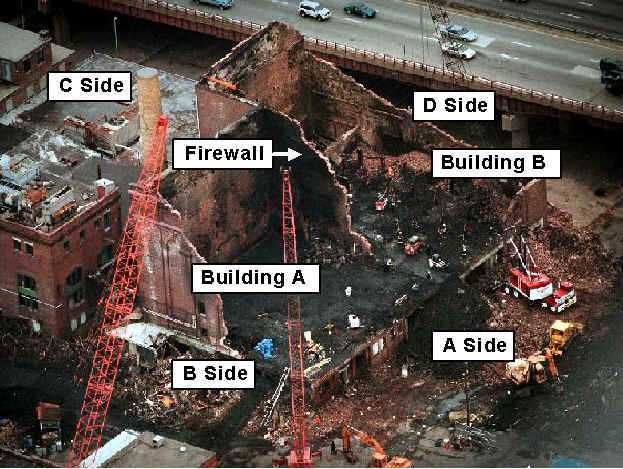
The structure was a cold-storage and warehouse building that had been vacant since 1991. The original building was constructed in 1905, and 7 years later (1912) another building was constructed on the western (D) side. The building constructed in 1905 was designated Building A, and the side constructed in 1912 was referred to as Building B. The entire building contained six floors above ground, for a total of 94,176 square feet, and a full basement (see Figure 1). The exterior walls, constructed of brick, measured 18 inches thick. The interior walls were covered with 6 to 18 inches of asphalt-impregnated cork (depending on the floor level), 4 inches of polystyrene and/or foam glass, and a thin layer of glassboard (see Photo 1). The flooring was wooden except for the flooring in the basement and first and second floors, which were concrete. The joists consisted of heavy timbers. Two stairwells were present; one was located on the B side and extended from the basement to the flat roof, and the other was located on the C side and extended to the third floor only (see Figure 2). Two sets of freight elevators were present, one on the B side and the other on the C side, and both were adjacent to stairwells. Two loading dock areas existed; one was located on the B side while the other was located on the C side (see Photo 2). Six windows were present on the second-floor level, three on the A side and three on the D side of Building B, but they had been covered with plywood. Window openings which were present in the stairwell on the B side were also covered with plywood. Although the building entrances and exits had been secured by plywood since 1991, homeless people had gained access to the building and established living quarters.
INVESTIGATION
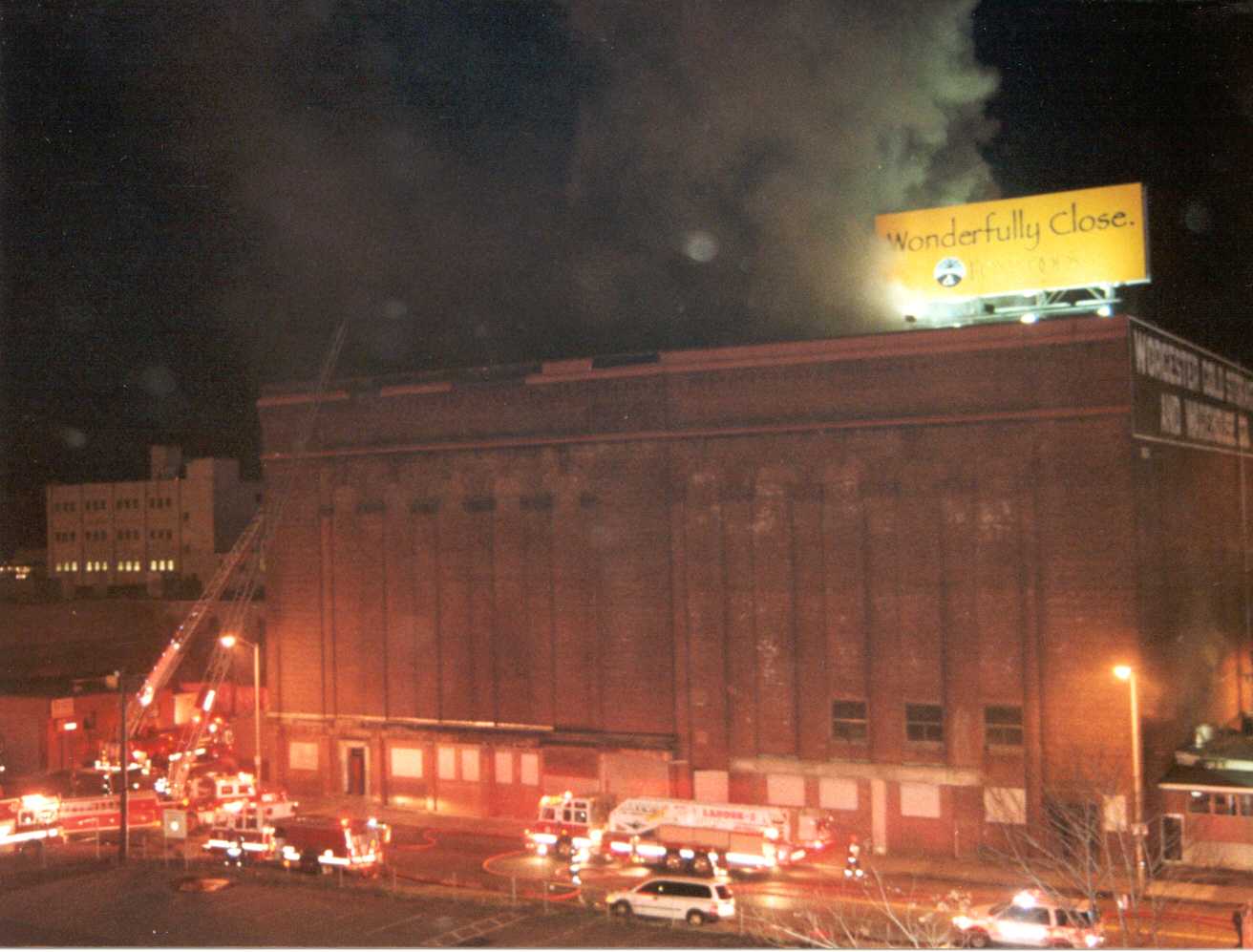
On December 3, 1999, at 1813 hours, an off-duty police officer reported smoke coming from the top of a building at 236 Franklin Street. Note: It has been determined that the fire was presumably started by two homeless people. The fire was started sometime between 1630 and 1745 hours in building B on the second floor (see Figure 2 and Photo 3). Therefore, the fire had been in progress for about 30 to 90 minutes before the box alarm was struck. At 1815 hours Central Dispatch advised "all companies strike and box 1438 Franklin and Arctic Streets for 236 Franklin Street." Engines 1, 6, 12, and 13 responded, along with Ladders 1 and 5, Rescue 1, and Car 3, which included the Incident Commander (IC#1) and his Aide. Engine 1 was first to arrive on the scene at 1816 hours and reported heavy smoke showing. At 1817 hours, Central Dispatch advised all companies that the correct address was 266 Franklin Street (cold-storage warehouse, see Photo 4). IC#1 arrived on the scene at 1819 hours and requested Central Dispatch to "strike a second alarm for Box 1438 Franklin and Arctic Street for 266 Franklin Street" due to the size of the building. Second-alarm companies consisted of Engines 2 and 16, Aerial Scope 2, and Car 2, which later became Incident Commander Two (IC#2). As the second-alarm companies arrived on the scene, they were directed by IC#1 to stage under a nearby interstate overpass. At 1820 hours, IC#1 radioed Central Dispatch and requested any available building information, but no information was ever found or received. Note: Due to the lack of pre-fire planning and inspection, and lack of building plans/drawings, confusion existed among the fire fighters as to the configuration and number of floors contained within the building. IC#1 then entered the building through a doorway from the first floor ground level on the A side and proceeded up the stairs to the second floor, where he conducted interior building operations. Simultaneously, his Aide circled the building to conduct a scene survey, and crews from Engine 13 and Ladder 1 also entered the building. The Aide reported that he was on the C/D corner of the building and that he saw heavy fire burning in and up the elevator shafts.
At 1822 hours, Engine 13 also reported fire in the elevator shaft on the second and third floors on the C/D corner. Ladder 1, in a freezer room on the second floor, reported they had a room full of fire, and they requested a line be brought in (see Photo 5). IC#1 ordered a 2 ½-inch line from Engine 1 and a 2 ½-inch line from Engine 16 be laid to the elevator shaft on the second floor at the C/D corner. A 1 3/4-inch line from Engine 1, a 2 ½-inch line from Engine 12, and a 2 ½-inch line from Engine 6 had been laid to the second and third floors through the stairwell on the B side (see Figure 3). All the lines were charged except the 2 ½-inch line from Engine 6, and active fire fighting began. (The line from Engine 6 had been laid to the third floor in Building A, but since no fire was found there, the line was not charged.) At 1826 hours, IC#1 was advised that two homeless people might be in the building. Car 2 (the second Incident Commander [IC#2] and his Aide) arrived on the scene at 1831 hours. IC#2 assumed command and was positioned on the outside of the A/B corner of the building. He requested a status report from IC#1, who was now the Interior Commander conducting interior operations, and he was told that heavy fire was burning on the second and third floors in Building B and that two homeless people might be in the building.
When Engine 1, Ladder 1, and Rescue 1 arrived on the scene on the first alarm, they all split up into crews. Engine 1's crew was comprised of a Captain and one fire fighter who entered the building looking for fire extension while the other two fire fighters from Engine 1 remained at the apparatus to set it up. Ladder 1's company split into two crews; one crew proceeded to the roof while the other crew checked for fire extension. Rescue 1, which was comprised of a Lieutenant and four fire fighters, including Victims 1 and 2, split into two, two-man crews while the driver remained with the apparatus. IC#2 instructed the crews from all three companies to search the building for homeless people and fire extension.
The crew from Engine 1 (Captain and fire fighter) entered the building from the B-side loading dock and joined one of the crews from Rescue 1 who had entered the building from the A-side first floor ground level stairway. The two crews, which included Victims 1 and 2 from Rescue 1, met at the stairwell on the first floor. They all proceeded up the stairwell and observed the other crew from Rescue 1 enter the third floor. Engine 1's crew and the two victims from Rescue 1 continued to the roof via the stairwell. Once on the roof, they proceeded to the C/D corner where they joined a crew from Ladder 1. The victims from Rescue 1 reported to Interior Command that they were on the roof and had heavy smoke and embers showing. The crews cleaned out a skylight measuring 15 square feet which was located over the elevator shaft, and Ladder 1 reported that the skylight was completely vented and that hot embers were coming through. The three crews (Engine 1, Rescue 1, and Ladder 1) left the roof, returned to the stairwell, and descended the stairs. Engine 1's crew were in the lead down the stairs, and they returned to the first floor. Ladder 1's crew descended the stairs after the Engine 1 crew and entered the second floor from the stairwell on the B side. Victims 1 and 2 from Rescue 1 entered the sixth floor and began a top-down, search-and-rescue sweep and fire extension check. After conducting the search-and-rescue sweep and fire extension check, they exited the sixth floor and entered the fifth floor. Simultaneously, the other crew from Rescue 1 (Lieutenant and one fire fighter) left the third floor and went to the fourth floor while Ladder 1's crew worked the second floor. The search-and-rescue crews were not using search ropes due to the light-to-moderate smoke conditions. Heavy, black, acrid smoke suddenly filled the second floor, causing all crews on the second floor to become disoriented and lose sight of one another. Ladder 1's crew conducted a right-hand search and eventually found the doorway that opened into the stairwell. They descended the stairwell until they found Interior Command who was now located between the second and third floors in the stairwell. Interior Command relocated to the bottom of the second-floor stairwell and ordered a head count. It was determined that two fire fighters from Rescue 1 were missing. The Aide for Interior Command, without wearing a self-contained breathing apparatus (SCBA), went to the fourth floor and stayed in the stairwell yelling, to no avail, for the missing fire fighters. At 1834 hours, IC#2 radioed the Lieutenant from Rescue 1, requesting his location and inquiring whether the primary and secondary searches for any civilians were completed. The Lieutenant responded that they had checked the third floor and were advancing up the stairwell to another floor. He reported no fire but heavy smoke. The Lieutenant and fire fighter from Rescue 1 proceeded to the fourth floor and were checking a room when visibility dropped to nearly zero. They were running low on air so they left the room, descended the stairs, and returned to an apparatus to change air bottles. While they were changing air bottles, the driver told them that two fire fighters from Rescue 1 were lost. The Lieutenant and fire fighter re-entered the building, and believing they were going to the fourth floor, instead went to the third floor because they thought the building had only five floors. Using search ropes, they searched the area on the third floor all the way back to a door opening through the firewall which separated the two buildings (see Figure 2 and Photo 6), but did not encounter the victims. At 1841 hours, Interior Command radioed Central Dispatch to make the following broadcast: "All companies working inside the structure use extreme caution. There may be holes in the floor, and the building may be extremely unsafe." At 1842 hours IC#2 requested a third alarm due to heavy fire conditions (see Photo 7). Central Dispatch struck a third alarm and requested that Engines 3 and 7 and Ladder 2 respond. At 1847 and 1848 hours respectively, one of the victims from Rescue 1 made the following two radio transmissions: "Rescue to Command, I need help on the floor below the top floor of the building. We are lost. Rescue to Command, we need help on the fourth floor." At 1849 hours, IC#2 had Central Dispatch clear the radio channel for emergency traffic, and another radio transmission was heard from one of the victims: "We have an emergency, Command. We are two floors down from the roof. This is the rescue company. Come now, two floors down from the roof. Guys, not the top floor, one floor down." A short time later, radio contact was made with the victims to determine their status. One of the victims replied, "We need air, we need air. I'm sharing a tank off me right now. We are lost. You got to send a rescue team up here for us. Second floor down from the roof, two floors down. We were on the roof, and then we checked the next floor down. Now we are on the next one. Hurry." At 1853 hours, Engine 13 reported that conditions inside the building were deteriorating very quickly. IC#2 requested a fourth alarm and that the Chief of the Department be notified. At 1854 hours, IC#2 radioed Interior Command that a fourth alarm had been struck and asked for verification of the floor the two fire fighters were trapped on. Interior Command responded, "They are on the second floor from the top. Two floors down from the roof, and I have Ladder 2, Engine 3, and Ladder 1 all going looking for them." At 1855 and 1856 hours, Interior Command made the following two requests: "Rescue 1, activate your PASS system so we can hear you. Activate your emergency alarm. Activate your PASS emergency alarm." At 1857 hours, one of the victims radioed back, "They are activated."
When Engines 3 and 7 and Ladder 2 arrived on the scene for the third alarm, the Engines were staged on the A/D corner, and Ladder 2 was staged on the A side of the building. The companies were instructed to proceed to Command at the front (A/B) corner of the building. Ladder 2's company consisted of a Lieutenant and three fire fighters. The driver stayed at the truck while the Lieutenant and two fire fighters proceeded to the command post. At the command post they received orders to conduct search-and-rescue operations on the fifth floor. They proceeded to the dock doors on the B side and entered the building. The Lieutenant and one fire fighter from Ladder 2 (Victims 3 and 4) were the first up the stairwell while the third fire fighter followed. At the third-floor level the trailing fire fighter joined a fire fighter from Engine 3 who had become separated from his crew. The two fire fighters began knocking out the plywood covering the window on the third floor. After knocking out the plywood, they went to the fourth floor and knocked out the plywood in that window. They ascended the stairwell to the fifth floor where they thought they would meet up with the Lieutenant and fire fighter from Ladder 2, but about 10 minutes had passed without seeing them, and they assumed that the Lieutenant and fire fighter had entered the room. The low-air alarm sounded on the SCBA worn by the fire fighter from Ladder 2, so he and the fire fighter from Engine 3 returned to the first floor. While on the first floor, at 1906 hours, the fire fighter from Ladder 2 radioed the Lieutenant from Ladder 2 and requested his location. The Lieutenant replied, "We came up the stairwell. We are on the fifth floor." He asked the Lieutenant, "What is your location on the fifth floor?" and the Lieutenant replied, "Good question." He asked the Lieutenant to repeat the message, and the Lieutenant replied, "We are doing a sweep. I believe we are in the front part of the building." At 1910 hours, the Lieutenant from Ladder 2 radioed Command: "Chief, get a company up the stairwell to the fifth floor. We can't locate the stairwell, or give us some sign as to which way to go. We are running low on air and we want to get out of here." At 1914 hours, the victims from Ladder 2 radioed again, requesting the following: "Send someone up to the stairwell to the fifth floor and stand in the doorway and start yelling. We can't find the door." The crew from Engine 3 (no victims) responded, "We have the message and are going to the fifth floor." Although the crew from Engine 3 located the doorway on the fifth floor at 1919 hours, they did not make contact with the victims from Ladder 2.
Engine 3's company consisted of a Lieutenant and four fire fighters, including Victims 5 and 6. Before leaving the Engine, the Lieutenant told the company that they were going to be used for search-and-rescue operations and that they would be entering the building. According to a pre-determined plan, the company split into two crews, one consisting of the Lieutenant and two fire fighters, and the other consisting of the senior fire fighter and a junior fire fighter (Victims 5 and 6). When both crews exited the truck, one crew ran to the command post while the second (Victims 5 and 6) finished putting on their gear. When the Engine 3 crew arrived at Command, two other crews were already there: three members from Ladder 2 and three members from Engine 7. Working in crews of three or four, they were instructed to use ropes while looking for the four missing fire fighters. The Lieutenant from Engine 3 received instructions to take air bottles up the stairwell and to try to locate Victims 1 and 2 who were supposedly on the fourth floor. The Lieutenant and two fire fighters each grabbed an air bottle and proceeded up the B stairwell to what they thought was the fourth floor. The third fire fighter became separated from the crew while going up the stairwell. Once at the third floor, the Lieutenant and one fire fighter entered the room and began their search. Visibility was about 1 ½ feet vertically off the floor and about 5 feet horizontally along the floor. While they were searching two rooms which were thought to be freezers about 35 square feet in size, visibility worsened, and they used a right-hand search to locate the door into the stairwell. They went down the stairwell and out onto the loading dock on the B side where they changed air bottles. Once again they went up the B stairwell, this time to the fifth floor, and without making contact with Victims 1 and 2, came back down to the loading dock. One of the Engine 3 fire fighters accompanied the Aide from IC#2 up the stairwell to the third and fourth floors. They held their breath to stop the flow of air into the face pieces of their SCBAs so that they could hear better and listened for PASS devices, but they never heard anything. They returned to the loading dock, and the fire fighter walked along the outside of the building's A side. He joined up with a fire fighter from Ladder 2 (the setup man) and another fire fighter. The three fire fighters used a 1 3/4-inch line off an Engine in the area to hit the fire through one of the windows on the second floor of the A side. Note: Two other fire fighters (Victims 5 and 6) did not make initial contact with command nor anyone at the scene, and were not seen entering the building. However, according to the Central Dispatch transcripts, they may have joined Victims 3 and 4 on the fifth floor.
At 1924 hours, IC#2 called for a head count of all the fire fighters, and it was then determined that six fire fighters were missing. At 1929 hours, the Chief of the Department called for a fifth alarm, and Engines 5 and 10 responded. At 1928 and 1929 hours, the victims from Engine 3 and Ladder 2 were radioed, but no response was ever received from either crew. Note: Between the hours of 1859 and 1932, Central Dispatch made eight dispatches regarding problems with radio emergency buttons (e.g., "Engine 6, your emergency button is going off." "Car 200, your alarm button is going off." "Car 200, disable your portable." "Engine 12, you have an open cam." "Engine 12, your emergency alarm keeps going off and will not allow transmission." "Engine 1, radio portable 2 alarm keeps going into alarm, and we can't transmit."). At 1931 and 1936 hours, the victims from Engine 3 and Ladder 2 were radioed a second time, and again no response was received. At 1948 hours, Interior Command radioed the victims from Ladder 2 and Engine 3 a third time but never received a response.
At 1949 hours, the crew from Engine 8, who had responded on the fourth alarm, radioed that they were on the fourth floor and that the structural integrity of the building had been compromised. A thermal imaging unit was brought to the scene by a neighboring fire department and put into service at 1952 hours, but it stopped working at 1955 hours due to the intense heat. At 1952 hours, a member from the Fire Investigations Unit reported to the Chief of the Department that heavy fire (flames of approximately 30 to 40 feet) had just vented through the roof on the C side. At 2000 hours Interior Command ordered everyone out of the building, and a series of short horn blasts were sounded to signal the evacuation. The operations changed from an offensive attack, including search and rescue, to a defensive attack with the use of heavy-stream appliances (see Photo 8). After the fire had been knocked down, search-and-recovery operations commenced until recall of the box alarm at 2227 hours on December 11, 1999.
CAUSE OF DEATH
The causes of death as released by the Office of the District Attorney are as follows: Victims 1 and 5 died as a result of severe thermal injuries and exposure to heat and noxious gases. Victims 2, 3, 4, and 6 died of inhalation of smoke, soot, and hot gases.
RECOMMENDATIONS AND DISCUSSION
Recommendation #1: Fire departments should ensure that inspections of vacant buildings and pre-fire planning are conducted which cover all potential hazards, structural building materials (type and age), and renovations that may be encountered during a fire, so that the Incident Commander will have the necessary structural information to make informed decisions and implement an appropriate plan of attack.1
Discussion: Inspections of vacant buildings allow fire fighters to become familiar with the interior of the buildings and any hazardous contents left behind. During a fire when the building is filled with smoke, knowledge of the layout of rooms, stairs, fire escapes, windows, elevators, and hazards inside the structure will be important life-saving information. During a vacant building inspection, the structural stability and hazards in hallways, stairways, and fire escapes can be identified and evaluated, and an informed plan of attack can be developed. In this incident, the exterior walls were constructed of brick materials 18 inches thick. The interior walls were covered with 6 to 18 inches of asphalt-impregnated cork (depending on the floor level), 4 inches of polystyrene and/or foam glass, and a thin layer of glassboard, all of which added greatly to the fire load and gave off toxic fumes when burned. Two stairwells existed, but only one stairwell (B side) extended from the basement to the roof. The other stairwell on the C side extended only to the third floor, a condition which created limited access throughout Building B. Two sets of freight elevators were present, but both were inoperable, and they created a chimney effect for the fire to reach other areas of the building. The interior rooms were maze-like in construction and contained freezers of varying sizes. Only two passageways per floor connected Building A to Building B. Six windows were present on the second floor and one window was present on each floor of the stairwell on the B side, and the windows were securely covered with plywood. Buildings with few openings are commonly known as "windowless buildings" and may present the following fire fighting problems: (1) locating a fire is difficult because the exact number of floor levels cannot be defined by counting windows from the outside at the command post; (2) horizontal or "cross venting" of burning floors inside buildings by opening windows is limited or not possible; (3) smoke buildup is rapid, and descends down from the top floors to street level due to reduced ventilation; (4) access to upper floor windows by aerial ladder master streams or for aerial ladders for rescue or search is limited or not possible; (5) flame and smoke spread throughout the entire building is concealed and undetermined; and (6) heat buildup inside the windowless building can be monumental. Buildings of this nature present numerous and varied hazards as evidenced by the above description, and it is paramount that fire officers and fire fighters be aware of the hazards present before they enter into a building of this nature. Detailed pre-fire planning of large, vacant, commercial buildings can assist fire fighters in preparing for a possible fire in the building. Multiple-company on-site training sessions, supervised by a battalion chief, should be held to practice large-scale fire fighting operations at the locations of these identified high-hazard vacant occupancies. When a pre-fire plan is drawn up for a large, vacant building, the following information on fire fighting strategy should be considered: (1) potential hazards inside, (2) water supply, (3) defensive strategy, (4) exposure protection strategy, (5) mutual-aid considerations, (6) collapse dangers, (7) apparatus positioning, and (8) venting strategies. Additionally, fire departments should have the capability of transmitting the pre-fire plans to the Incident Commander on the fireground via a mobile data terminal (an onboard computer) in the event they are not readily available as hard copy.
Recommendation #2: Fire Departments should ensure that the incident command system is fully implemented at the fire scene.2
Discussion: The Incident Command System (ICS) defines the roles and responsibilities to be assumed by personnel and the operating procedures to be used in the management and direction of emergency incidents and other functions. The Incident Commander (IC) is the individual with overall responsibility to implement and oversee the system. The functions of the IC include, but are not limited to (a) assumption, confirmation, and position of command, (b) situation evaluation, (c) initiating, maintaining, and controlling communications, (d) deployment, (e) strategy/incident action planning, and (f) organization.
a. Assumption, confirmation, and position of command. After the IC arrives on the fireground and assumes command, a stationary command post on the exterior of the fire building should be established. Command positioning becomes a critical factor in the overall effectiveness of the incident. National experience reflects that a strategic level of command can only be produced if the IC is in a stationary command post position. The command post should be situated in a conspicuous location which affords the IC a good view of the fire building and surrounding area. Ideally, it would offer a view of two sides of the fire building. Advantages of a command post are (1) stationary position, (2) a relatively quiet place in which to think and make decisions, and (3) a vantage point to oversee the operation. A stationary command post also offers the potential for improved lighting, protection from weather, space for additional staff, and access to more powerful mobile radios, reference and pre-planning materials, and portable computers (in some instances).
b. Situation evaluation. The IC is the only person who has the exterior, stationary, command-post-position advantage that allows current and forecasted information to be received, processed, evaluated, and then translated into a series of decisions that control the position and function of the fire fighters working in and around the hazard zone. This information management function becomes a major reason why the IC should stay at the command post. It is difficult for an IC to receive, decipher, and then react effectively to reports from all over the incident site if he/she is moving around, in proximity to operational noise, distracted by direct face-to-face communications with fire fighters, and limited to a portable radio as opposed to a more powerful mobile radio.
c. Initiate, maintain, and control communications. It is the IC's responsibility to initiate, maintain, and control effective incident communications. This communications function is critical to safe and effective incident operations because it is the means by which the IC and all the other incident participants stay connected. Being able to effectively communicate becomes the major tool the IC uses to exchange information and to create effective action. The IC should use the stationary command post advantage to maintain continuous and clear communications.
d. Deployment. The deployment function requires the IC to provide and manage a steady, adequate, and timely stream of appropriate resources. Typically, the IC logs the arriving units into the inventory and tracking system on a tactical worksheet in the stationary command post. The IC also enters the units into a standard accountability system that tracks where companies/crews are located in the hazard zone.
e. Strategy/incident action planning. A critical responsibility of the IC is to identify and manage the overall incident strategy (offensive or defensive). The IC must continually evaluate the relationship between the level of hazards present and the basic capability of the safety system to protect fire fighters from those hazards. The hazards present at structural fires involve structural collapse, thermal and toxic insult, becoming trapped and running out of air, and becoming disoriented, lost, and running out of air. Given the conditions present at this incident—large, vacant building with multiple levels, very few openings to the outside, maze-like interior, numerous freezer rooms of varying size with doors—combined with an active fire, created an environment with numerous hazards.
f. Organization. The ICS creates three standard levels of operation: the strategic level managed by the IC, the tactical level commanded by the sector officers, and the task level where fire companies conduct fire fighting activities. The organizational design provides a system where the strategic and tactical levels provide direction and support to the fire fighters who conduct fire fighting activities. In small incidents (single family dwellings and small commercials buildings) the situation is generally manageable enough for the IC to operate on both the strategic and tactical levels, and to directly manage fire companies performing standard functions. This incident occurred in a complicated six-floor building with a basement—essentially a high-rise building. A high-rise type of incident organization could have been implemented to manage the operations. A standard high-rise organization would involve, but not be limited to, a lobby control sector to log resources into the building, sector assignments on each floor, a vertical water supply function, stairway support, and a safety officer.
Recommendation #3: Fire departments should ensure that a separate Incident Safety Officer, independent from the Incident Commander, is appointed when activities, size of fire, or need occurs such as during multiple-alarm fires, or responds automatically to pre-designated fires.3-5
Discussion: According to NFPA 1561, paragraph 4-1.1, "The Incident Commander shall be responsible for the overall coordination and direction of all activities at an incident. This shall include overall responsibility for the safety and health of all personnel and for other persons operating within the incident management system." Although the Incident Commander (IC) is in overall command at the scene, certain functions should be delegated to ensure that adequate scene management is accomplished. According to NFPA 1500, paragraph 6-1.3, "As incidents escalate in size and complexity, the Incident Commander shall divide the incident into tactical-level management units and assign an Incident Safety Officer to assess the incident scene for hazards or potential hazards." The Incident Safety Officer (ISO), by definition, is "an individual appointed to respond to or assigned at an incident scene by the Incident Commander to perform the duties and responsibilities specified in this standard. This individual can be the health and safety officer or it can be a separate function." According to NFPA 1521, paragraph 2-1.4.1, "an Incident Safety Officer shall be appointed when activities, size, or need occurs." Each of these guidelines compliments the others and indicates that the Incident Commander is in overall command at the scene; however, oversight of all operations is difficult. An ISO can assist the Incident Commander by providing oversight for on scene fire fighter health and safety.
Recommendation #4: Fire departments should ensure that Standard Operating Procedures (SOPs) and equipment are adequate and sufficient to support the volume of radio traffic at multiple-alarm fires.3
Discussion: At times, fireground communications become ineffective because of congested radio traffic and inadequate radio equipment on the fireground. Although IC#2 had Central Dispatch clear the radio channel for emergency traffic, most radio operators continued to use the same channel. Also, during the half-hour period immediately following the first victims' emergency message, Central Dispatch made eight dispatches regarding problems with radio emergency buttons. Standard operating procedures (SOPs) should be written and implemented, and communications equipment should be of sufficient quantity and quality to support the volume of communications encountered at the fire scene. In the event of Maydays or emergencies on the fireground, fire fighters should switch radio operations to a new frequency or other channels. This would open the main channel for communication in case of an emergency or lost fire fighters.
Recommendation #5: Fire departments should ensure that Incident Command always maintains close accountability for all personnel at the fire scene.3,4,6,7
Discussion: Accountability on the fireground is of paramount importance. It is the responsibility of all officers to account for every fire fighter assigned to their company and relay this information to Incident Command. Accountability on the fireground can be maintained by several methods. One system uses individual tags for every fire fighter and officer responding to an incident, and another uses a company officer's riding list which states the names, assigned tools, and duties of each member responding with every fire company. One copy of the list should be posted in the fire apparatus and one copy carried by the company officer. The list posted in the apparatus is used if the company officer or the entire company is reported missing. Additionally, fire fighters should not work beyond the sight or sound of the supervising officer unless equipped with a portable radio. These fire fighters should communicate with the supervising officer by portable radio to ensure accountability and indicate completion of assigned duties. SOPs should address accountability, including the location and the duties of the responding fire companies. Just as company officers should know the location of all fire fighters assigned to the company, the Incident Commander should know the operating locations of officers and companies assigned on the first-alarm assignment. As a fire increases and additional fire companies respond to the fire, a communication assistant with a command board should assist the Incident Commander with accounting for all fire companies at the scene, at the staging area, and at the rehabilitation area. One of the most important aids for accountability at a fire scene is an incident management system, and it should be established by the Incident Commander. An Incident Commander bears the overall responsibility for safety at a fire, but safety is a team effort and should be ensured by the Incident Commander and sector and company officers. In this incident, sector officers could have been assigned to the four sides (A, B, C, and D) of the building thereby improving the accountability system.
Recommendation #6: Fire departments should use guide ropes/tag lines securely attached to permanent objects at entry portals and place high-intensity floodlights at entry portals to assist lost or disoriented fire fighters in emergency escape.8
Discussion: In a dark, smoky environment, large open areas, or maze-like construction, fire fighters often become lost or disoriented, and too often they are unable to escape. The use of guide ropes/tag lines securely attached to permanent objects at entry portals and held by fire fighters as they enter smoke-filled environments can become lifelines for emergency escape. Also, the use of high-intensity floodlights at entry portals could assist fire fighters in situations requiring emergency escape. In this incident a Lieutenant from Ladder 2 radioed Command: "Chief, get a company up the stairwell to the fifth floor. We can't locate the stairwell, or give us some sign as to which way to go. We are running low on air, and we want to get out of here." At 1914 hours, the victims from Ladder 2 radioed the following: "Send someone up to the stairwell to the fifth floor and stand in the doorway and start yelling. We can't find the door."
Recommendation #7: Fire departments should ensure that a Rapid Intervention Team is established and in position upon arrival.4
Discussion: A Rapid Intervention Team (RIT) should respond if all companies are engaged in active fire fighting activities, multiple alarm fires, and other incidents where fire department members are subject to hazards that would be immediately dangerous to life and/or health in the event of an equipment failure, sudden change of conditions, or mishap.9 The team should report to the officer in command and remain at the command post until an intervention is required to rescue a fire fighter(s) in distress.
A RIT is specially trained in search-and-rescue techniques. In addition to standard fire fighting gear, the RIT is equipped with search-and-rescue tools and equipment, including a first-aid kit and a resuscitator for aiding injured fire fighters. Many fire fighters who are overcome by smoke or who are caught or trapped by fire actually become disoriented first. They are lost in smoke and cannot find their way to an exit, or their SCBAs run out of air. They become trapped, and then fire or smoke kills them. The primary contributing factor, however, is disorientation.
When the IC orders the RIT to conduct an emergency search or rescue, the companies can regroup and take roll call. With a RIT in place, they can respond immediately to the location given by lost or disoriented fire fighters to conduct rescue operations.
Recommendation #8: Implement an overall health and safety program such as the one recommended in NFPA 1500, Standard on Fire Department Occupational Safety and Health Program.4
Discussion: NFPA 1500 provides the framework for a safety and health program for fire departments. The specified goal of the standard is to reduce the probability of occupational fatalities, illnesses, and disabilities among fire fighters. NFPA points out that the standard is meant to be appropriate for voluntary compliance tailored to the needs of each individual department. Formal implementation of the standard, particularly the development of a written plan for compliance with NFPA 1500, should include development of fire service occupational health programs as outlined in both NFPA 1500 and 1582. At the time of this incident, a formal written safety and occupational health program was not available. Note: Since the incident, the department involved has developed a Structural Fire Fighting Development Program. The Program address the following: (1) Operational Tactics and Strategies Within the Incident Command System, (2) Rapid Intervention Teams, (3) Search and Rope Rescue Procedures, (4) Thermal Imaging Technology, (5) Radio Communications on the Fire Ground and Emergency Procedures, (6) Building Construction in the Fire Service, and (7) High Rise Fires.
Recommendation #9: Fire departments should consider using a marking system when conducting searches.10
Discussion: Several methods of marking searched rooms can be used by the fire service: chalk or crayon marks, masking tape, specially designed door markers, and latch straps over doorknobs. SOPs usually dictate the method of marking; however, any method used must be known to and clearly understood by all personnel who may participate in the search. It is recommended that search crews use a two-part marking system. The crew affixes half of the mark when entering the room and completes the mark when exiting the room. This avoids duplication of effort by alerting other rescuers that the room is being or has been searched. If a search crew becomes lost, this mark will serve as a starting point for others to begin looking for them.
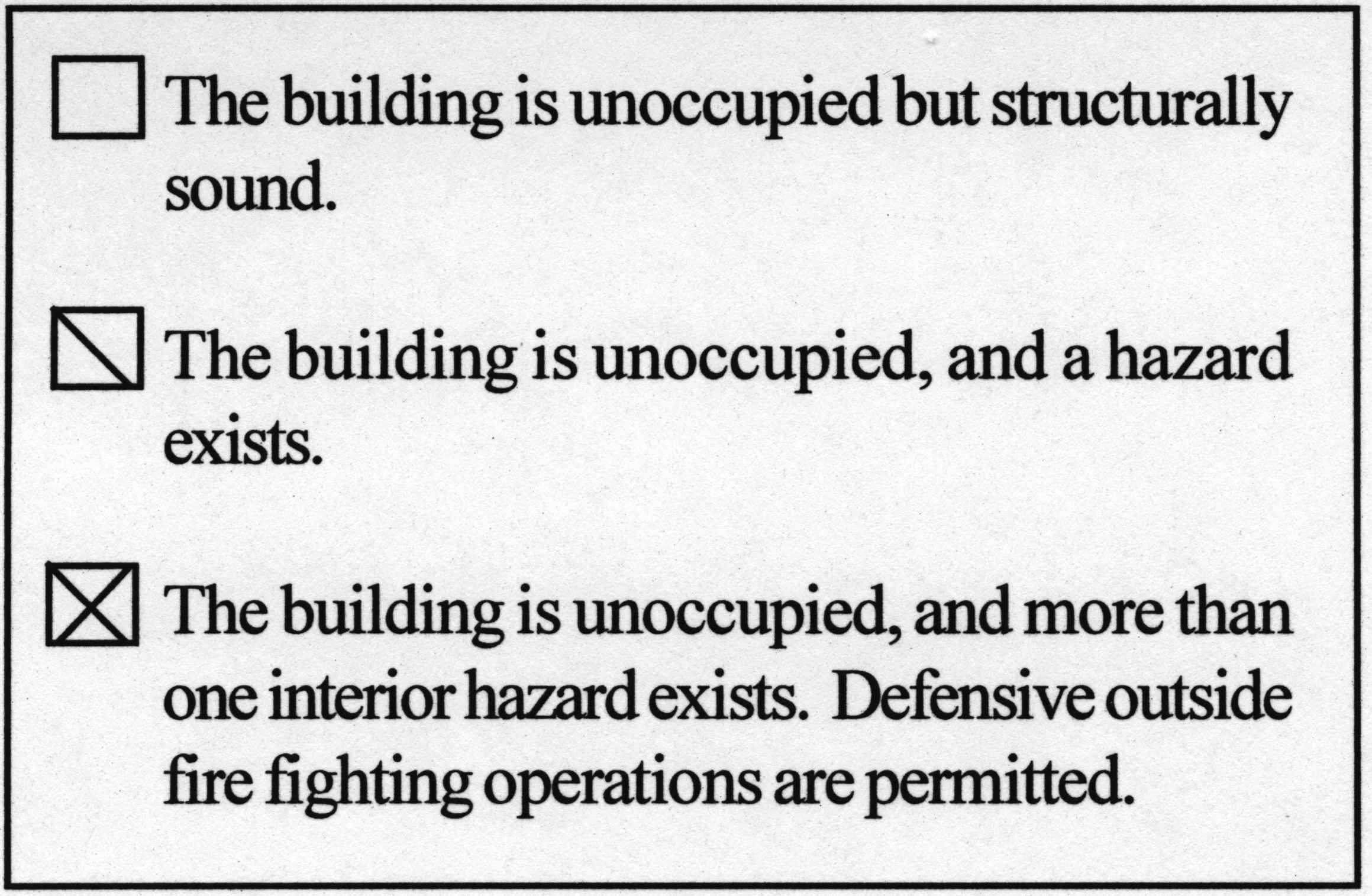
Recommendation #10: Fire departments should identify dangerous vacant buildings by affixing warning placards to entrance doorways or other openings where fire fighters may enter .1
Discussion: Vacant buildings can and do pose numerous hazards to fire fighters' health and safety. Hazards should be identified and warning placards affixed to entrance doorways or other openings to warn fire fighters of the potential dangers. Hazards can be structural as the result of building deterioration or damage from previous fires. Structural hazards can occur when building owners or salvage workers remove components of the building such as doors, railings, windows, electric wiring, utility pipes, etc. Abandoned materials such as paper and flammable or hazardous substances and collapse hazards constitute additional dangers fire fighters may encounter. Collapse hazards can be chimney tops, parapet walls, slate and tile roof shingles, metal and wood fire escapes, advertising signs, and entrance canopies. For example, a warning placard may be a 12-inch-square piece of metal painted reflective yellow so that it glows in the dark and indicates to fire fighters that hazards exist inside the building. Following are examples of warning placards developed and used by the New York City Fire Department.
Recommendation #11: Fire departments should ensure that officers enforce and fire fighters follow the mandatory mask rule per administrative guidelines established by the department.10
Discussion: Since carbon monoxide (CO) is given off in varying quantities during all fires, and other toxic materials are typically present, it is paramount that officers enforce and fire fighters follow the department's guidelines for the wearing of masks at structure fires. In this incident, a number of fire fighters reported not wearing their masks inside the structure even while encountering moderate smoke conditions. Far more fire deaths occur from carbon monoxide than from any other toxic product of combustion. This colorless, odorless gas is present in every fire. The poorer the ventilation and the more inefficient the burning, the greater the quantity of carbon monoxide formed. Concentrations of carbon monoxide in air above five hundredths of one percent (0.05 percent) (500 ppm) can be dangerous. When the level is more than 1 percent, unconsciousness and death can occur without physiological signs. Even at low levels of exposure fire fighters should not use signs and symptoms for safety factors. Headaches, dizziness, nausea, vomiting, and cherry-red skin can occur at many concentrations, based on an individual's dose and exposure. Therefore, these signs and symptoms are not good indicators of safety.7 Table 1 lists the toxic effects of carbon monoxide.10
A 1-percent concentration of carbon monoxide in a room will cause a 50-percent level of carboxyhemoglobin in the blood stream in 2½ to 7 minutes. A 5-percent concentration can elevate the carboxyhemoglobin level to 50 percent in only 30 to 90 seconds. Because the newly formed carboxyhemoglobin may be traveling through the body, a person previously exposed to a high level of carbon monoxide may react later.8 If fire fighters develop any of these signs, they should immediately exit the structure and receive the proper medical care. Severe exposures to carbon monoxide can cause nerve injury or brain damage. If fire fighters are overcome with carbon monoxide, they should not be allowed to re-enter a smokey atmosphere. If fire fighters suspect they have been exposed to carbon monoxide, they should notify their officer or the IC. In this incident, several fire fighters stated they experienced nausea, dizziness, and disorientation; however, some of these fire fighters re-entered the structure to search for the victims.
Recommendation #12: Fire departments should explore the use of thermal imaging cameras to locate lost or downed fire fighters and civilians in fire environments.11
Discussion: Thermal Imaging Cameras (TICs), as reported by their manufacturers, can be used for a myriad of fire-related situations. In a search-and-rescue operation, a fire fighter can use the TIC to scan a room in seconds rather than crawl across the entire floor in search of civilians or downed fire fighters. TICs can be used to conduct size-ups and to find the source of fire upon arrival at the scene. They can also be used to provide vital information for planning fire attack, overhaul, and ventilation. TICs are also useful at hazmat incidents, and they can be used to scan large areas for hot spots in wildland fires. TICs should be used in a timely manner, and fire fighters should be properly trained in their use and be aware of their limitations.
Carbon Monoxide (CO)(ppm) |
Carbon Monoxide in air (percent) |
Symptoms |
|---|---|---|
100 |
0.01 |
No symptoms-no damage |
200 |
0.02 |
Mild headache; few other symptoms |
400 |
0.04 |
Headache after 1 to 2 hours |
800 |
0.08 |
Headaches after 45 minutes; nausea, collapse, and unconsciousness after 2 hours. |
1,000 |
0.1 |
Dangerous; unconscious after 1 hour |
1,600 |
0.16 |
Headache, dizziness, nausea after 20 minutes. |
3,200 |
0.32 |
Headache, dizziness, nausea after 5 to 10 minutes; unconsciousness after 30 minutes. |
6,400 |
0.64 |
Headache, dizziness, nausea after 1 to 2 minutes; unconsciousness after 10 to 15 minutes. |
12,800 |
1.26 |
Immediate unconsciousness, danger of death in 1 to 3 minutes. |
Table 1. Toxic Effects of Carbon Monoxide.10
Recommendation #13: Manufacturers and research organizations should conduct research into refining existing and developing new technology to track the movement of fire fighters on the fireground.
Discussion: Fire fighter fatalities often are the result of fire fighters becoming lost or disoriented on the fireground. The use of systems for locating lost or disoriented fire fighters could be instrumental in reducing the number of fire fighter deaths on the fireground. One such system, a wireless tracking system, requires locating three accurately placed spread-spectrum transmitters around a building to provide positioning information. Other systems may include a UHF Radio system or an Infrasound Low Frequency Detector. Research into refining existing systems and developing new technologies for tracking the movement of fire fighters on the fireground should continue.
REFERENCES
1. Dunn V [2000]. Vacant building fires. Firehouse Magazine. May 2000, pp. 20-26.
2. Brunacini, AV [2000]. Written expert review of NIOSH FACE report 98F-47 of August 21, 2000, from AV Brunacini, to R Braddee, Division of Safety Research, National Institute for Occupational Safety and Health, Centers for Disease Control and Prevention, Public Health Service, U.S. Department of Health and Human Services.
3. National Fire Protection Association [1995]. NFPA 1561, standard on fire department incident management system. Quincy, MA: National Fire Protection Association.
4. National Fire Protection Association [1997]. NFPA 1500, standard on fire department occupational safety and health program. Quincy, MA: National Fire Protection Association.
5. National Fire Protection Association [1997]. NFPA 1521, standard on fire department safety officer. Quincy, MA: National Fire Protection Association.
6. Morris GP, Brunacini N, Whaley L [1994]. Fire ground accountability: the Phoenix system. Fire Engineering 147(4):45-61.
7. Dunn V [1998]. Managing and controlling fireground risks and dangers-Part 1. Firehouse Magazine. August 1998, pp. 26-29.
8. Norman J [1998]. Fire officers handbook of tactics. 2nd ed. Saddle Brook, NJ: Fire Engineering Books and Videos.
9. Massachusetts Firefighting Academy. Rapid intervention crew: impact series student handout. Stow, MA: Massachusetts Firefighting Academy.
10. International Fire Service Training Association [1995]. Essentials of fire fighting. 4th ed. Stillwater, OK: Fire Protection Publications, Oklahoma State University.
11. http://www.firehouse.com/news/99/10/19_camera.html
INVESTIGATOR INFORMATION
This investigation was conducted by Richard W. Braddee, Team Leader; Frank C. Washenitz, Thomas P. Mezzanotte, and Nancy T. Romano, Safety and Occupational Health Specialists; and Theodore Pettit, Senior Fire Fighter Investigator, Fire Fighter Fatality Investigation and Prevention Program, Division of Safety Research, NIOSH, and Tim R. Merinar, Engineer, and Tom McDowell, Physical Scientist, Respirator Branch, Division of Respiratory Disease Studies, NIOSH.
EXPERT REVIEW
Expert review was provided by Francis L. (Frank) Brannigan, Society of Fire Protection Engineers (Fellow); Alan V. Brunacini, Chief, City of Phoenix Fire Department; and Vincent Dunn, Deputy Chief (Ret.), FDNY.
1st Alarm 1815 hours |
2nd Alarm 1819 hours |
3rd Alarm 1842 hours |
4th Alarm 1854 hours |
5th Alarm 1929 hours |
|---|---|---|---|---|
Engine 1 Captain |
Engine 2 Lieutenant |
Engine 3 Lieutenant |
Engine 8 Captain |
Engine 5 Lieutenant |
Engine 6 Lieutenant |
Engine 16 |
Engine 7 Lieutenant |
Engine 15 Lieutenant |
Engine 10 Lieutenant |
Engine 12 Lieutenant |
Aerial Scope 2 3 Fire Fighters |
Ladder 2 Lieutenant |
Ladder 4 Captain |
|
Engine 13 |
Car 2 (IC#2) Deputy Chief |
Car 1 (Chief) Chief |
|
|
Ladder 1 Captain |
|
|
|
|
Ladder 5 |
|
|
|
|
Rescue 1 Lieutenant |
|
|
|
|
Car 3 (IC#1) District Chief |
|
|
|
|
Table 2. Fire Alarms for Cold-Storage and Warehouse Building Fire - Massachusetts
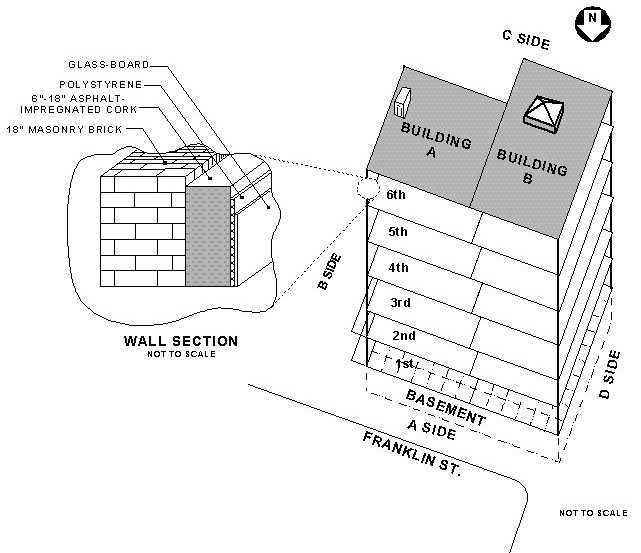
Figure 1. Cold Storage and Warehouse Building Layout, Plain View
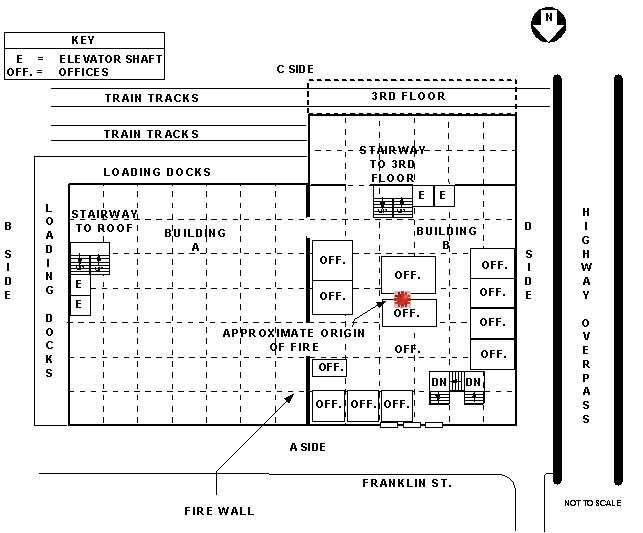
Figure 2. Cold Storage and Warehouse Building, 2nd Floor Layout, Plain View
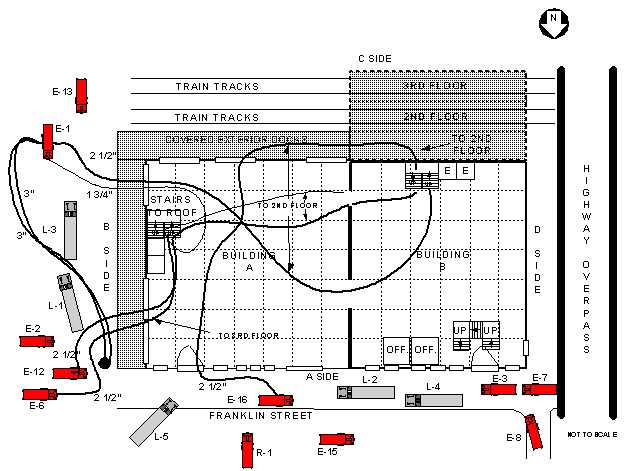
Figure 3. Cold Storage and Warehouse Building, Hoseline/Apparatus Layout, First Floor View
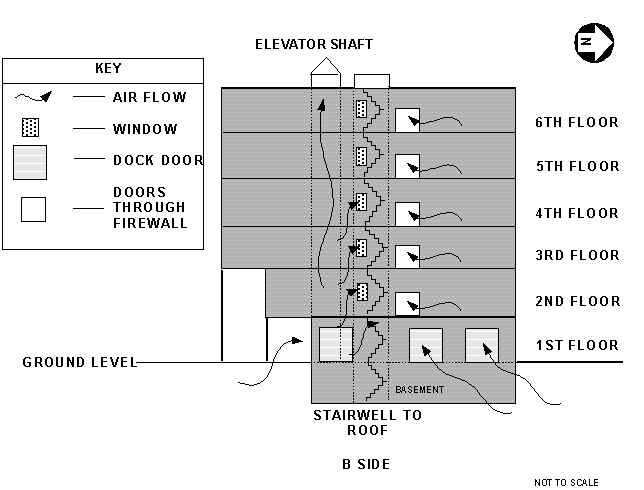
Figure 4. Cold Storage and Warehouse Building, B Side, Exterior Section View
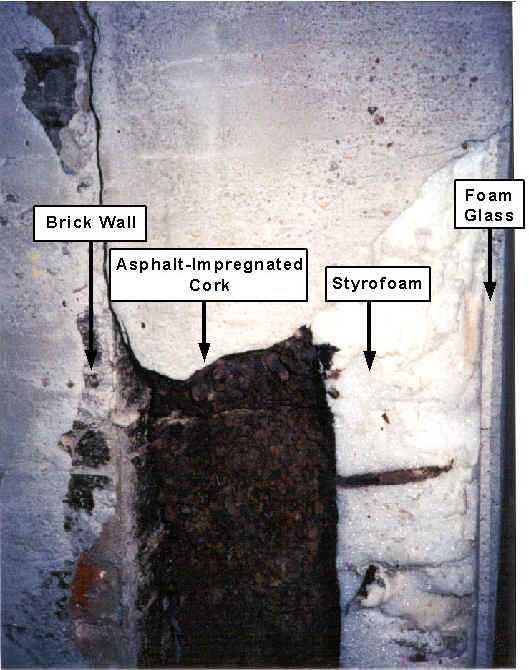
Photo 1. Interior Insulation of Cold-Storage and Warehouse Building
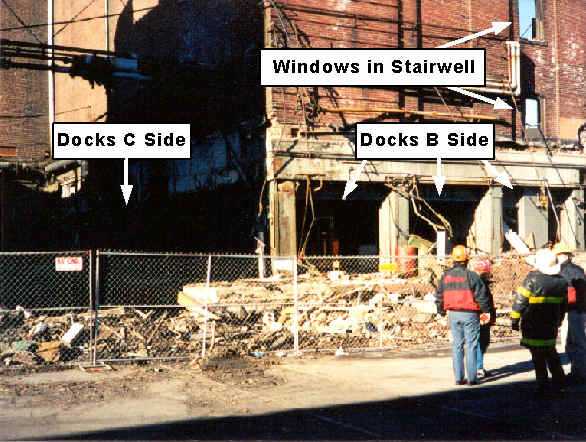
Photo 2. Corner "B/C" of Cold-Storage and Warehouse Building
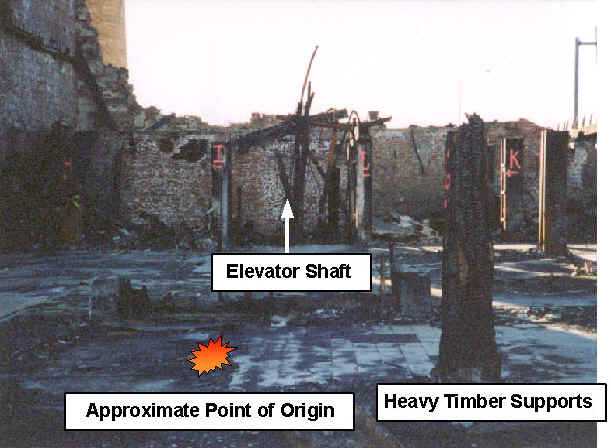
Photo 3. Second Floor "B" Building

Photographed by Roger B. Conant.
Photo 4. Cold-Storage and Warehouse Building Shortly After First Alarm - 1825 Hours

Photo 5. Cold-Storage Freezer Room
© 1999 Telegram & Gazette Staff/Paul Kapteyn
All Rights Reserved
Photo 6. Firewall Between Building A and B, Cold-Storage and Warehouse Building
Photographed by Roger B. Conant.
Photo 7. Cold-Storage and Warehouse Building After Third Alarm - 1842 Hours

© 1999 Roger B. Conant.
All Rights Reserved
Photo 8. Cold-Storage and Warehouse Building at 2030 Hours
ATTACHMENT
(This attachment was originally sent as an official letter summarizing the results of a NIOSH evaluation of the fire department's SCBA maintenance program.)
DEPARTMENT OF HEALTH & HUMAN SERVICES
Public Health Service
Centers for Disease Control
and Prevention (CDC)
National Institute for Occupational
Safety and Health - ALOSH
1095 Willowdale Road
Morgantown, WV 26505-2888
NIOSH Reference: TN-11472
Phone: (304) 285-5907
Fax: (304) 285-6030
May 1, 2000
Dear Chief:
During our visit to the Fire Department on April 20, 2000, Tim Merinar and I had the opportunity to evaluate your fire department's self-contained breathing apparatus (SCBA) maintenance program. The objectives of our visit were to evaluate your SCBA maintenance program and to make recommendations for improvement. This evaluation consisted of visiting the SCBA maintenance area, interviewing fire department personnel associated with the maintenance of SCBA, reviewing SCBA maintenance records and procedures, and evaluating the compressed-air and oxygen cylinder refilling stations located at your training and equipment maintenance facility. Our evaluation process benefitted substantially from the cooperation of your staff. Their cooperation was instrumental in providing us with information necessary for the evaluation of your SCBA maintenance program.
Your current SCBA maintenance program was evaluated and compared to the respirator and SCBA maintenance requirements listed in the following recognized national standards:
- Title 29, Code of Federal Regulations (CFR) Part 1910.134 known as The OSHA Respirator Standard.
- National Fire Protection Association (NFPA) 1404, Standard for a Fire Department Self-Contained Breathing Apparatus Program, 1996 Edition.
- National Fire Protection Association (NFPA) 1500, Fire Department Occupational Safety and Health Program, 1997 Edition.
- American National Standards Institute, Inc. (ANSI), American National Standard for Respiratory Protection, ANSI Z88.2-1992.
These standards specify the minimum benchmark requirements that all fire department respirator programs should strive to meet or exceed. Compliance with these standards is considered to be essential to maintain SCBA in a condition meeting the certification requirements of the National Institute for Occupational Safety and Health (NIOSH) found in Title 42, Code of Regulation, Part 84, Subpart H, as well as the National Fire Protection NFPA 1981 Standard on Open-Circuit Self-Contained Breathing Apparatus for the Fire Service, 1997 Edition. Failure to maintain your SCBA in an approved condition voids the NIOSH approval until such time as each affected SCBA can be inspected, serviced, and returned to an approved condition.
The following areas were identified within the Fire Department SCBA maintenance program as areas where improvement is needed in order to comply with the referenced national standards:
1) NIOSH recommends that your SCBA maintenance program be under the direct control of one designated individual who is a Fire Department employee and who has no other fire fighting or administrative responsibility. In general, this individual's area of responsibility could be tailored to meet the department's needs, but should include supervision and control of all aspects of the program including the SCBA preventive maintenance program, repair, testing, record keeping, and auditing. Our evaluation revealed no documented policy designating an authority with jurisdiction over the SCBA maintenance program. It was also noted that personnel currently responsible for the SCBA maintenance program have numerous responsibilities in other areas.
- Title 29, Code of Federal Regulations (CFR), Part 1910.134 (the OSHA Respirator Standard) at 1910.134(c) requires each respirator program to be administered by a suitably trained program administrator.
2) The Fire Department should establish written standard operating procedures for managing its various SCBA maintenance, repair, and testing functions. During our visit, we provided draft copies of generic standard operating procedures and record keeping forms that may assist you in developing your program documents. Procedures should be developed to address each of the following areas:
- a. SCBA Maintenance Training
b. SCBA Inspection
c. SCBA Maintenance
d. Air Quality Program
e. Recharging Cylinders
f. Record Keeping
g. Identification of Defective SCBA and Removal from Service - NFPA 1404, Chapter 1-5.5 and 1-5.6 require the authority having jurisdiction to establish written standard operating procedures and training policies for members responsible for respiratory protection use, cleaning, and maintenance.
- NFPA 1404, Chapter 1-5.7 specifies that the authority having jurisdiction shall establish written standard operating procedures for inspection, maintenance, repair, and testing of respiratory protection equipment.
- NFPA 1404, Chapter 7-2.3 specifies that written policies shall be established to ensure that air is obtained only from a source that meets the requirements of CGA G7.1, Commodity Specifications for Air.
- NFPA 1404, Chapter 7-2.5 specifies that proper cylinder recharging procedures and safety precautions shall be posted in a conspicuous location at each fill station.
- The OSHA Respirator Standard 29 CFR 1910.134(c)(1)(v) and 1910.134(h)(4) require the employer to develop schedules and procedures for inspecting respirators and ensuring that respirators that fail inspection or are otherwise found to be defective are removed from service.
3) A preventive maintenance program should be established to ensure regularly scheduled preventative maintenance is conducted on each SCBA at least annually. It is noted that the Fire Department does not operate a preventive maintenance program but rather attempts to repair defective SCBA on an as-needed basis.
- The OSHA Respirator Standard 29 CFR 1910.134(c)(1)(v); 1910.134(c)(1)(vi); and 1910.134(h) require the employer to develop and implement a written respiratory protection program that includes specific procedures and schedules for cleaning and disinfecting, storage, inspection, maintenance, and repair of respirators used by employees.
- NFPA 1404, Chapter 6-1.2 and 6-1.3 require annual inspection and servicing of SCBA by qualified personnel. Chapter 6-1.3 requires annual servicing to be conducted following the manufacturer's recommendations and should include :
- a. Disassembly of the SCBA into major components
b. Flow testing of the regulator
c. Disassembly and cleaning of the regulator
d. Replacement of worn parts, or those recommended by the manufacturer in the regulator assembly.
e. Disassembly of the low-air alarm and cleaning and replacement of component parts as necessary.
f. Cleaning and replacement of components of the facepiece and harness assembly, and replacement of component parts as necessary.
g. Reassembly of the entire SCBA and testing for proper operation of all components.
h. Proper recording of all performed maintenance on record keeping forms. - NFPA 1404, Chapter 6-2.1 specifies that a preventative maintenance program shall be established by the authority having jurisdiction for all SCBA used in the organization.
- NFPA 1404, Chapter 6-2.2 specifies that the SCBA preventative maintenance program shall be conducted in order to prevent SCBA malfunction and failures of equipment during use.
- NFPA 1500, Chapter 5-3.1 specifies the fire department shall adopt and maintain a respiratory protection program that addresses the selection, inspection, safe use, and maintenance of respiratory protection equipment, training in its use, and the assurance of air quality testing.
- NFPA 1404, Appendix A, A-6.2 states that an SCBA should be rebuilt by its manufacturer or by a person trained and certified by the manufacturer at intervals as recommended by the manufacturer.
Specific guidelines for determining and scheduling preventive maintenance actions can best be compiled with assistance from your SCBA manufacturer. Frequency of complete SCBA overhaul should be based on the manufacturer's recommendation. If no manufacturer's recommendation is provided, NIOSH recommends that rebuilding of SCBA assemblies be performed every 3 years.
It is apparent that in order for the Fire Department to establish a comprehensive preventive maintenance program, the department will need to acquire additional resources. It would be impossible for your current SCBA maintenance staff to continue to complete repairs on mobile apparatus, power tools, and other equipment as well as perform all tasks necessary for repair and comprehensive preventive maintenance for nearly 150 SCBA. In addition to increased staff, the acquisition of spare SCBA would allow your SCBA maintenance staff to perform preventative maintenance without interruptions to emergency response.
4) Records should be maintained for each SCBA, facepiece, and cylinder at the department. During our visit, we were shown a filing system where repair and testing information was maintained for each SCBA and filed according to company assignment. Some electronic files had also been developed to help track some SCBA services such as cylinder hydrostatic test schedules. NIOSH recommends that the computerized records system be expanded to address the following standard excerpts:
- NFPA 1404, Chapter 2-2.3 specifies that an individual record of each SCBA regulator and harness assembly shall be maintained. This record shall include the inventory or serial number, date of purchase, date of manufacture, date placed into service, location, maintenance and repairs, replacement parts used, upgrading, and test performance.
- NFPA 1404, Chapter 2-2.4 specifies that an individual record of each SCBA cylinder shall be maintained. This record shall include the inventory or serial number date of purchase, date of manufacture, date placed into service, location, hydrostatic test pressure and dates, and any inspection and repairs. The hydrostatic test dates shall appear on each cylinder according to the manufacturer's instructions and applicable government agencies.
- NFPA 1404, Chapter 2-2.5 specifies that an individual record of each SCBA facepiece shall be maintained. This record shall include the inventory or serial number, date of purchase, location, maintenance and repairs, replacement parts, upgrading, and test performance.
- NFPA 1500, Chapter 2-7.5 specifies that each fire department shall assure that inspection, maintenance, repair, and service records are maintained for all vehicles and equipment used for emergency operations and training.
- The OSHA Respirator Standard 29 CFR 1910.134(h)(3) lists the requirements for respirator inspections. 1910.134(h)(iv)(A and B) list the requirements for documenting each inspection.
- The American National Standard for Respiratory Protection, ANSI Z88.2-1992, Chapter 10.2 specifies that the SCBA user shall inspect the respirator, and that a record of inspection dates shall be kept for each respirator.
It is apparent that the computer support at the Fire Department would have to be substantially upgraded to permit the development of an effective electronic filing and information management system.
5) A program should be developed to ensure that all SCBA cylinders meet the US Department of Transportation (DOT) standards for periodic requalification and service life limitations. These standards are listed in Title 49, Code of Federal Regulations (CFR), Part 173.34(e). A review of the records kept at the Training Center indicated that some in-service cylinders had past-due hydrostatic test dates. DOT requirements for the fiberglass-wrapped cylinders utilized by the Fire Department require that each cylinder be submitted every three years to a DOT-certified retester for inspection and hydrostatic testing. The DOT requirements limit the service life for these cylinders to 15 years from the date of manufacture, regardless of the last date of requalification.
- NFPA 1500, Chapter 5-3.8 specifies that SCBA cylinders shall be hydrostatically tested within the periods specified by the manufacturers and the applicable governmental agencies.
- NFPA 1404, Appendix A, A-6.2 specifies that breathing gas cylinders be tested as prescribed in Title 49, Code of Federal Regulations (CFR), Part 178, Shipping Container Specification Regulations.
- Title 42, Code of Federal Regulations (CFR), Part 84.81(a), NIOSH Requirements for Respiratory Protection Devices requires cylinders used on NIOSH-approved SCBA to meet the minimum DOT requirements.
6) The Fire Department should develop and implement a standard operating procedure that specifies that air samples will be collected from each SCBA cylinder filling station and analyzed by an accredited laboratory on a quarterly basis.
- NFPA 1500, Chapter 5-3.1 specifies the fire department shall adopt and maintain a respiratory protection program that includes provisions for air quality testing.
- NFPA 1500, Chapter 5-3.7.1 specifies that when a fire department manufacturers its own breathing air, the fire department shall be required to provide documentation that a sample of the breathing air obtained directly from the point of transfer from the filling station to the SCBA cylinders has been tested at least quarterly.
- NFPA 1404, Chapter 7-1.1 specifies that written policies shall be established to ensure that air is obtained only from a source that meets the requirements of CGA G7.1, Commodity Specifications for Air.
- NFPA 1404, Chapter 7-1.2 requires each fire department to have its breathing air tested by an accredited laboratory at least every three months.
7) The Fire Department should develop and implement an SCBA facepiece fit-testing program to ensure that all SCBA users are able to achieve a proper face-to-facepiece seal.
- The OSHA Respirator Standard 29 CFR 1910.134(f) requires employers to have all employees who wear tight-fitting facepiece respirators fit-tested with the same make, model, style, and size facepiece used by the employee.
- NFPA 1404, Chapter 4-11(b) specifies that the authority having jurisdiction shall evaluate the ability of each of its department members to demonstrate that a proper face-to-facepiece seal has been achieved.
8) Annual evaluations of the SCBA Maintenance Program should be conducted to monitor and evaluate the effectiveness of the overall SCBA maintenance program.
- The OSHA Respirator Standard 29 CFR 1910.134(h)(3)(1)(ix) requires the employer to develop and maintain as part of the overall written respiratory protection program, procedures for regularly evaluating the effectiveness of the program.
- NFPA 1404, Chapter 8-1.1 specifies that the authority having jurisdiction shall review the organization's respiratory protection program annually for the purposes of determining the need to upgrade or change various aspects of the program.
These recommendations are based upon the premise that all SCBA are life-saving devices which will only perform as well as they are maintained. Since they are expected to function and perform properly each time they are used, it is important that SCBA maintenance and inspection be given the utmost priority at the department level.
During our visit, we provided your SCBA maintenance personnel with a copy of the peer-reviewed document Respirator Maintenance Program Recommendations for the Fire Service developed by NIOSH and published in the Journal of the International Society for Respiratory Protection. We also provided draft copies of generic standard operating procedures and record keeping forms that may assist you in developing improvements to your overall SCBA maintenance program.
During our visit, we also inspected and evaluated the oxygen cylinder refilling station located at your training and equipment maintenance facility. Oxygen cylinders are typically refilled for use in oxygen resuscitators and other emergency medical equipment used to administer oxygen therapy. The OSHA Respirator Standard 29 CFR 1910.134 as well as the NFPA 1404 Standard for a Fire Department Self-Contained Breathing Apparatus Program, do not specifically address these types of medical devices. However, safe handling practices dictate that oxygen refilling systems as well as oxygen equipment be stored in a clean, dry, air-conditioned location that is locked to limit access only to those individuals who have been properly trained and qualified to work with oxygen equipment. All cleaning, repair, and refilling operations should be conducted using the appropriate special tools which are cleaned, maintained, and dedicated only for use on oxygen equipment. The oxygen cylinder refilling station that we examined failed to meet the above requirements.
The NIOSH Fire Fighter Injury Investigation Report 98F-23, Oxygen Regulator Flash Severely Burns One Fire Fighter - Florida, and the joint FDA and NIOSH Public Health Advisory: Explosions and Fires in Aluminum Oxygen Regulators both contain a number of recommendations on safe handling procedures for handling and filling portable oxygen cylinders. Both documents address special precautions which should be taken for oxygen cylinder filling stations. A copy of each document is enclosed.
The Compressed Gas Association pamphlet CGA G-4 (1996 revision) Oxygen (especially chapter 4) and the NFPA 53 Guide on Fire Hazards in Oxygen-Enriched Atmospheres, 1994 Edition are also excellent sources of information on oxygen cylinder storage and safe handling procedures.
I trust this information is beneficial to your needs. If you have any questions or require additional information, please contact me at (304) 285-6337.
Sincerely yours,
Thomas W. McDowell
Physical Scientist
Respirator Branch
Division of Respiratory Disease Studies
This page was last updated on 10/17/01
- Page last reviewed: November 18, 2015
- Page last updated: October 15, 2014
- Content source:
- National Institute for Occupational Safety and Health Division of Safety Research