


Nine Career Fire Fighters Die in Rapid Fire Progression at Commercial Furniture Showroom South Carolina
 ShareCompartir
ShareCompartir
 Death in the Line of Duty...A summary of a NIOSH fire fighter fatality investigation
Death in the Line of Duty...A summary of a NIOSH fire fighter fatality investigation
F2007-18 Date Released: February 11, 2009
SUMMARY
On June 18, 2007, nine career fire fighters (all males, ages 27 56) died when they became disoriented and ran out of air in rapidly deteriorating conditions inside a burning commercial furniture showroom and warehouse facility. The first arriving engine company found a rapidly growing fire at the enclosed loading dock connecting the showroom to the warehouse. The Assistant Chief entered the main showroom entrance at the front of the structure but did not find any signs of fire or smoke in the main showroom.
 |
|
Incident Scene |
He observed fire inside the structure when a door connecting the rear of the right showroom addition to the loading dock was opened. Within minutes, the fire rapidly spread into and above the main showroom, the right showroom addition, and the warehouse. The burning furniture quickly generated a huge amount of toxic and highly flammable gases along with soot and products of incomplete combustion that added to the fuel load. The fire overwhelmed the interior attack and the interior crews became disoriented when thick black smoke filled the showrooms from ceiling to floor. The interior fire fighters realized they were in trouble and began to radio for assistance as the heat intensified. One fire fighter activated the emergency button on his radio. The front showroom windows were knocked out and fire fighters, including a crew from a mutual-aid department, were sent inside to search for the missing fire fighters. Soon after, the flammable mixture of combustion by-products ignited, and fire raced through the main showroom. Interior fire fighters were caught in the rapid fire progression and nine fire fighters from the first-responding fire department died. At least nine other fire fighters, including two mutual-aid fire fighters, barely escaped serious injury.
NIOSH investigators concluded that, to minimize the risk of similar occurrences, fire departments should:
- develop, implement and enforce written standard operating procedures (SOPs) for an occupational safety and health program in accordance with NFPA 1500
- develop, implement, and enforce a written Incident Management System to be followed at all emergency incident operations
- develop, implement, and enforce written SOPs that identify incident management training standards and requirements for members expected to serve in command roles
- ensure that the Incident Commander is clearly identified as the only individual with overall authority and responsibility for management of all activities at an incident
- ensure that the Incident Commander conducts an initial size-up and risk assessment of the incident scene before beginning interior fire fighting operations
- train fire fighters to communicate interior conditions to the Incident Commander as soon as possible and to provide regular updates
- ensure that the Incident Commander establishes a stationary command post, maintains the role of director of fireground operations, and does not become involved in fire-fighting efforts
- ensure the early implementation of division / group command into the Incident Command System
- ensure that the Incident Commander continuously evaluates the risk versus gain when determining whether the fire suppression operation will be offensive or defensive
- ensure that the Incident Commander maintains close accountability for all personnel operating on the fireground
- ensure that a separate Incident Safety Officer, independent from the Incident Commander, is appointed at each structure fire
- ensure that crew integrity is maintained during fire suppression operations
- ensure that a rapid intervention crew (RIC) / rapid intervention team (RIT) is established and available to immediately respond to emergency rescue incidents
- ensure that adequate numbers of staff are available to immediately respond to emergency incidents
- ensure that ventilation to release heat and smoke is closely coordinated with interior fire suppression operations
- conduct pre-incident planning inspections of buildings within their jurisdictions to facilitate development of safe fireground strategies and tactics
- consider establishing and enforcing standardized resource deployment approaches and utilize dispatch entities to move resources to fill service gaps
- develop and coordinate pre-incident planning protocols with mutual aid departments
- ensure that any offensive attack is conducted using adequate fire streams based on characteristics of the structure and fuel load present
- ensure that an adequate water supply is established and maintained
- consider using exit locators such as high intensity floodlights or flashing strobe lights to guide lost or disoriented fire fighters to the exit
- ensure that Mayday transmissions are received and prioritized by the Incident Commander
- train fire fighters on actions to take if they become trapped or disoriented inside a burning structure
- ensure that all fire fighters and line officers receive fundamental and annual refresher training according to NFPA 1001 and NFPA 1021
- implement joint training on response protocols with mutual aid departments
- ensure apparatus operators are properly trained and familiar with their apparatus
- protect stretched hose lines from vehicular traffic and work with law enforcement or other appropriate agencies to provide traffic control
- ensure that fire fighters wear a full array of turnout clothing and personal protective equipment appropriate for the assigned task while participating in fire suppression and overhaul activities
- ensure that fire fighters are trained in air management techniques to ensure they receive the maximum benefit from their self-contained breathing apparatus (SCBA)
- develop, implement and enforce written SOPS to ensure that SCBA cylinders are fully charged and ready for use
- use thermal imaging cameras (TICs) during the initial size-up and search phases of a fire
- develop, implement and enforce written SOPs and provide fire fighters with training on the hazards of truss construction
- establish a system to facilitate the reporting of unsafe conditions or code violations to the appropriate authorities
- ensure that fire fighters and emergency responders are provided with effective incident rehabilitation
- provide fire fighters with station / work uniforms (e.g., pants and shirts) that are compliant with NFPA 1975 and ensure the use and proper care of these garments.
Additionally, federal and state occupational safety and health administrations should:
- consider developing additional regulations to improve the safety of fire fighters, including adopting National Fire Protection Association (NFPA) consensus standards.
Additionally, manufacturers, equipment designers, and researchers should:
- continue to develop and refine durable, easy-to-use radio systems to enhance verbal and radio communication in conjunction with properly worn SCBA
- conduct research into refining existing and developing new technology to track the movement of fire fighters inside structures.
Additionally, code setting organizations and municipalities should:
- require the use of sprinkler systems in commercial structures, especially ones having high fuel loads and other unique life-safety hazards, and establish retroactive requirements for the installation of fire sprinkler systems when additions to commercial buildings increase the fire and life safety hazards
- require the use of automatic ventilation systems in large commercial structures, especially ones having high fuel loads and other unique life-safety hazards.
Additionally, municipalities and local authorities having jurisdiction should:
- coordinate the collection of building information and the sharing of information between building authorities and fire departments
- consider establishing one central dispatch center to coordinate and communicate activities involving units from multiple jurisdictions
- ensure that fire departments responding to mutual aid incidents are equipped with mobile and portable communications equipment that are capable of handling the volume of radio traffic and allow communications among all responding companies within their jurisdiction.
INTRODUCTION
On June 18, 2007, nine male career fire fighters (the victims), aged 27 to 56, died when they became disoriented in rapidly deteriorating conditions inside a burning commercial furniture showroom and warehouse facility. At least seven other municipal fire fighters and two mutual aid fire fighters barely escaped serious injury.
The National Institute for Occupational Safety and Health (NIOSH), Division of Safety Research, Fire Fighter Fatality Investigation and Prevention Program, learned of the incident on June 19, 2007 through the national news media. On June 19, 2007, the U.S. Fire Administration (USFA) notified NIOSH of the fatalities. That same day, a Safety Engineer and a General Engineer from NIOSH traveled to South Carolina to initiate an investigation of the incident. The NIOSH investigators traveled to the incident site and met with representatives of the Bureau of Alcohol, Tobacco and Firearms (ATF), National Institute of Standards and Technology (NIST), South Carolina State Law Enforcement Division (SLED), and South Carolina Occupational Safety and Health Administration (SC-OSHA). The NIOSH investigators were on-site June 20-22, and the NIOSH General Engineer returned June 24th to work with representatives of NIST to collect data related to the structures constructiona for the NIOSH investigation and for a comprehensive fire reconstruction model. Note: The NIST Building and Fire Research Laboratory is developing a computerized fire model to aid in reconstructing the events of the fire. When completed, this model will be available at the NIST website: http://www.nist.gov/el/. (Link Updated 1/17/2013)
a The fire completely destroyed the structure and the sheet metal roof was removed at the direction of ATF before NIOSH and NIST were allowed access to the structure. Consequently, detailed information on the construction was not available and NIOSH and NIST frequently relied on photographs of the structure after the fire.
On July 9, 2007, three NIOSH investigators (Safety Engineer, General Engineer, and Safety and Occupational Health Specialist), along with representatives of NIST, returned to South Carolina. Meetings were conducted with the Fire Chief; Assistant Chief; the citys Director, Safety Management Division; and the citys Workers Compensation administrator.
During the weeks of July 9-13, July 16-20, and August 27-31, 2007, interviews were conducted with officers and fire fighters who were on-duty and dispatched to the incident scene, as well as fire fighters who were off-duty and came to the scene to offer assistance. Fire fighters from two mutual aid departments were also interviewed during these times. NIST representatives participated in many of the NIOSH interviews to collect information for their computerized fire model.
During the course of the ensuing investigation, the NIOSH investigators met with chief officers and fire fighters from the initial responding department, two local mutual aid departments, NIST staff, the county coroner, the county emergency response dispatch center staff, city building inspectors, city water system officials, representatives of the International Association of Fire Fighters (IAFF) labor union, U.S. Fire Administration staff, ATF, and representatives of the citys Fire Review Team (FRT).
NIOSH investigators reviewed some departmental standard operating procedures,b the victims training records, chief officers training records, and floor plans and photographs of the structure. Photographs were obtained from a number of sources including NIOSH, NIST, the city police department, the FRT and national media.c NIOSH investigators visited the citys fire training academy, met with the training officer, and reviewed the training schedule (see Appendix I). The departments maintenance and repair facility (for in-house maintenance and repair of fire apparatus, equipment, and self-contained breathing apparatus (SCBA)) was visited and maintenance records were reviewed. An independent inspection report for one of the apparatus involved in the incident, that had been contracted for by the city, was reviewed (see Appendix II). The citys fire and police dispatch center was visited as well as the dispatch center for the first responding mutual aid department. Other sources of information used in this investigation include state and federal OSHA regulations, NFPA standards, fire department pre-plan information (see Appendix III), coroners reports, copies of the fireground radio transmissions provided by the city legal department, a transcript of the dispatch audio records provided by the FRT, and the FRT Phase I and Phase II reports.1,2
b NIOSH investigators reviewed two Standard Operating Procedures (SOPs) provided to NIOSH: Standard Operating Procedures Engine Company 2 (undated) and Fire Department Policies and Procedures Manual dated July 25, 2005. The city reported that there were additional SOPs in place at the time of the incident.
c Some photographs used in this NIOSH report have been altered to remove names, faces and other identifiers.
NIOSH contracted with a leading expert in personal protective clothing to evaluate the clothing and personal protective equipment worn by the victims (see Appendix IV). This evaluation took place on August 29, 2007. The evaluation site and handling of the evidence materials was coordinated with the assistance of the county coroners office and the city police department. The PPE evaluation was witnessed by representatives of NIOSH, NIST, the FRT, the county coroners office, the city police department, and the state fire marshals office.
The lead NIOSH investigator participated in a meeting convened by the U.S. Fire Administration on September 20, 2007 to discuss the status of ongoing investigations and share information not of a confidential nature. This meeting consisted of representatives of the U.S. Fire Administration, ATF, the FRT, the county coroner, NIST and NIOSH. The lead NIOSH investigator participated in a similar meeting convened by the FRT on December 18, 2007. This meeting consisted of representatives of the FRT, ATF, the county coroner, NIST, and NIOSH.
Safety and Health RegulationsSouth Carolina is one of 26 states and territories which administers its own occupational safety and health program through an agreement with the U.S. Department of Labor, Occupational Safety and Health Administration (OSHA). The South Carolina Occupational Safety and Health Administration (SC-OSHA) has jurisdiction over private and public sector employers and employees within the state. The state occupational safety and health act requires employers to provide their employees with a safe and healthy worksite which is free of hazards which may cause injuries and illnesses to workers. South Carolina has adopted the federal OSHA Standards verbatim, with a few exceptions.3 Most notably, South Carolina OSHA has revised the federal OSHA Respiratory Protection Standard paragraph 1910.134(g)(4)(ii), commonly known in the fire service as the two in two out rule, to allow fire fighters to enter immediately-dangerous-to-life-or-health (IDLH) atmospheres with only one fire fighter located outside the IDLH atmosphere until additional fire fighters arrive, provided certain conditions are met.
Following the fatal fire, SC-OSHA cited the fire department for several alleged violations and assessed penalties.4 The fire department and city contested these findings and SC-OSHA and the city reached a settlement in which the fire department was cited for two violations, an inadequate fire department incident command system and failure to ensure use of personal protective equipment by some fire fighters at the incident.5 SC-OSHA also cited the furniture store employer for locked exit doors, fire doors not operating properly, and not implementing an emergency action plan at the store.4
Fire Department
At the time of the incident, the career fire department was an ISOd Class I rated department with 19 fire companies located throughout the city. The fire department serves a population of approximately 106,000 in a geographic area of about 91 square miles. In June 2007 the fire department consisted of approximately 240 uniformed fire fighters and fire officers. The department operated 16 engine companies and 3 ladder truck companies at 14 stations in the city. Each apparatus was staffed with four fire fighters but routinely operated with three fire fighters per apparatus (a captain, engineer, and fire fighter), depending on the staffing available each shift. The standard work shift was 24 hours on-duty and 48 hours off-duty, with fire fighters assigned to one of three rotating shifts. Each shift was supervised by an Assistant Chief. On the day of the incident, the department had 61 fire fighters, 4 Battalion Chiefs and an Assistant Chief working on-duty. Note: At the time of the incident, the fire department did not have a safety officer position and a safety officer was not designated at the incident. Since then, the fire department has hired a full-time permanent safety officer.
d ISO is an independent commercial enterprise which helps customers identify and mitigate risk. ISO can provide communities with information on fire protection, water systems, other critical infrastructure, building codes, and natural and man-made catastrophes. Virtually all U.S. insurers of homes and business properties use ISOs Public Protection Classifications (PPC) to calculate premiums. In general, the price of fire insurance in a community with a good PPC is substantially lower than in a community with a poor PPC, assuming all factors are equal. ISOs PPC program evaluates communities according to a uniform set of criteria known as the Fire Suppression Rating Schedule (FSRS). The FSRS has three main parts fire alarm and communications (10%), the fire department (50%), and water supply (40%). The FSRS references nationally recognized standards developed by the National Fire Protection Association (NFPA) and the American Water Works Association. Rated fire departments are classified 1 through 10 with Class 1 being the best rating a fire department can receive. More information about ISO and their Fire Suppression Rating Schedule can be found at the website http://www.isogov.com/about/.
The fire department utilized the 911 dispatch center operated by the municipal police department (PD). The local county also maintains an emergency communications / dispatch center and provides communications for two small fire departments. Some mutual aid fire departments within the county maintain their own dispatch centers.
The first mutual aid department to respond to the scene was a career department that employs 60 fire fighters and officers. It maintains four stations and serves a population of approximately 24,000 residents in an area of approximately 30 square miles. Jurisdictional boundaries between this mutual aid department and the municipal department were intermingled. Adjoining properties in the same block could be in different jurisdictions. This led to incidents where a department would be the first to arrive at a working fire outside its jurisdiction.
The second mutual aid department to respond to the scene was a combination department with 44 fire fighters that serves a rural population of 14,000.
Training
In South Carolina, it is up to the local fire chief to decide what level of training is required for fire department personnel to obtain in order to meet SC-OSHA training requirements. At the time of the incident, this municipal fire department required fire fighters to receive basic training to at least Fire Fighter I certification from the South Carolina Fire Academy or some other source. While the South Carolina Fire Academy is accredited by the International Fire Service Accreditation Congress to provide a number of NFPA level courses, at the time of the incident, the fire department recognized training from sources other than the South Carolina Fire Academy as meeting their basic certification requirements. Note: Basic fire fighter certification required by the fire department at the time of the incident did not meet NFPA 1001, Standard for Firefighter Professional Qualifications. 6
Once hired, the recruits were assigned to the departments training center for 10 days of hands-on training after which the new fire fighters were assigned to companies throughout the city. The departments training focused on equipment use, SCBA use, ladder drills, hydrant hookup, hose lays, hose pulls, rescue drills, and live-burn exercises (see training schedule Appendix I ). A training officer supervised the recruit training and oversaw the departments training program. Individual companies normally trained from 0930 to 1130 hours each day with each companys captain responsible for the training. Training on hydrant location and hook-up was done once per month. Driver / operator training was mainly on-the-job hands-on training. Individual fire fighters could request to receive driver / operator training. The request would then be reviewed and approved through the departments chain of command.
Training records provided by the city for the nine victims consisted of verification of the weekly in-station training, certificates indicating training on subjects such as National Incident Management System (NIMS), weapons of mass destruction (WMD) and emergency medical services medical first responder. SCBA facepiece fit test records were also provided. Training records for the chief officers were provided, consisting mainly of copies of National Incident Management System (NIMS) training certificates.
Victims
Note: Throughout this report, the 9 victims are identified by the order in which they were located at the scene, identified by the County Coroner, removed from the structure and transported. The following table provides information on each victim.
| Victims (Order located) |
Rank
|
Apparatus
|
Age |
Experience
(yrs) |
|---|---|---|---|---|
|
1
|
Engineer |
Engine 19
|
37
|
9
|
|
2
|
Fire fighter |
Engine 19
|
56
|
32
|
|
3
|
Fire fighter |
Engine 16
|
46
|
2
|
|
4
|
Assistant Engineer |
Ladder 5
|
27
|
1.5
|
|
5
|
Captain |
Engine 16
|
49
|
29
|
|
6
|
Captain |
Engine 19
|
48
|
30
|
|
7
|
Acting Captain |
Ladder 5
|
40
|
12.5
|
|
8
|
Captain |
Engine 15
|
34
|
11.5
|
|
9
|
Fire fighter |
Ladder 5
|
27
|
4
|
Equipment and Personnel
The municipal fire department initially responded to the alarm with 3 apparatus and 9 fire fighters including Engine 11 (E-11 acting captain, acting engineer and fire fighter), Engine 10 (E-10 captain, acting engineer and fire fighter), Ladder 5 ( L-5 acting captain, engineer (assistant engineer), and fire fighter), a battalion chief (BC-4) and an Assistant Chief (AC). Note: Fire department procedures stated that where structures were 5 stories or less in height, the first alarm assignment would be 2 engines, 1 ladder truck, and a Battalion Chief. For structures over 5 stories in height, the first alarm assignment would be 3 engines, 1 ladder truck, a Battalion Chief and the Assistant Chief. Once on-scene, the Incident Commander could request additional resources as deemed necessary. Procedures also stated that a confirmed report of smoke showing would automatically send an additional engine. When a ranking officer arrived on-scene, that officer automatically became Incident Commander.
Engine 16 (E-16 captain, engineer, and fire fighter) was dispatched after BC-4 (the initial Incident Commander (IC)) radioed dispatch to confirm smoke was showing at the incident site as per department procedures. E-16 was designated as the third-due engine responding to all structure fires in the western district (where the incident occurred) if not assigned on the initial dispatch. Chief Officers requested Engine 15 (E-15), Engine 12 (E-12), Engine 19 (E-19), Engine 6 (E-6), Engine 3 (E-3), Engine 13 (E-13), Engine 9 (E-9), and Ladder 4 (L-4) as the incident escalated. Additional responders included the Battalion Chief from the neighboring district (BC-5) and the Battalion Chief of training (BC-T). A large number of off-duty officers and fire fighters also responded to the incident scene. Some of the off-duty fire fighters responded with turnout gear, others did not.
Only the units directly involved in the operations preceding the fatal event are discussed in this report. The activities of the additional mutual aid departments that were dispatched after the structure collapsed are not addressed by this report.
Timeline
Note: This timeline is provided to set out, to the extent possible, the sequence of events as the fire departments responded. The times are approximate and were obtained from review of the dispatch audio records, witness interviews, photographs of the scene and other available information. In some cases the times may be rounded to the nearest minute, and some events may not have been included. The timeline is not intended, nor should it be used, as a formal record of events.
The response, listed in order of arrival (time approximate) and events, include:
1907 hours
- Dispatch for possible fire behind furniture store
1909 hours
- BC-4, E-10, E-11, L-5 enroute
- BC-4 confirms smoke showing while enroute
- E-10, L-5, E-16 acknowledge hearing BC-4 confirm fire
- AC enroute
1910 hours
- E-16 enroute as third-due engine
- E-15 relocates to western district
- BC-4 arrives on scene and reports trash fire at side of building.
- BC-4 radios for E-10 to come down side of building
1911 hours
- Assistant Chief (AC) on scene
- E-10 and E-11 on scene
1912 hours
- AC radios for E-16 to come inside building when they arrive on-scene.
- (Showroom clear with no fire/smoke showing)
- Ladder 5 on scene
- Fire Chief (enroute) radios E-15 to relocate to Station 11
- AC radios dispatch to send Engine 12
- BC-4 radios Car 2 and says he knows fire is inside building
- Engine 12 dispatched to scene
1913 hours
- BC-4 radios E-12 that he needs E-12 to lay a supply line to E-10
- E-11 acting captain radios I need an 1 ½ inside this building
- (Door connecting showroom to loading dock was opened by AC showing heavy fire in loading dock)
- AC radios E-15 to come on
- AC radios E-15 and says to bring 1 ½ hose line inside to right rear of building
- E-6 begins relocating to the west side
1914 hours
- AC radios BC-4 and says fire is inside the rear of the building and moving towards the showroom
- AC radios dispatch to send E-6
- E-6 dispatched to scene
- Fire Chief radios dispatch to send E-19 and have E-6 relocate to Station 11
1915 hours
- AC radios E-16 to bring 2 ½ hose line in front door
- E-16 radios AC to confirm assignment
- E-16 on-scene
1916 hours
- L-5 engineer and L-5 fire fighter both radio E-11 to charge line (1 ½ line pulled by L-5 / E-11 crews)
- E-19 enroute
- L-5 again requests E-11 to charge hose line
- Fire Chief on scene
1917 hours
- E-12 on scene - assigned to lay supply line to E-10
- E-15 on scene
1919 hours
- Fire Chief radios E-6 and tells them to come to scene and come in front door
- E-6 responds they are enroute
- Fire Chief radios dispatch to call the power company
- E-16 captain radios charge that 2 ½
1920 hours
- E-11 engineer radios the E-11 acting captain to see if he wants the 2 ½ hose line charged.
- AC replies not until the supply line is charged
- E-19 on scene
- E-12 radios E-10 water coming 10
- E-12 engineer radios dispatch that the police department is needed because cars are running over hoses. Dispatch replies that the police department is enroute
1921 hours
- AC radios E-16 engineer - 16, what about that supply line? E-16 engineer replies he is looking for a hydrant.
- E-6 on scene
1922 hours
- E-11 engineer radios E-16 that tank water is down to half-full
- E-16 engineer replies he is looking for hydrant
1924 hours (see Photo #1)
- Battalion Chief 5 (BC-5) on scene
- Fire Chief radios E-12 to boost water pressure on supply line by 50 pounds
- E-12 acknowledges
- AC radios.. We need that 2 ½ (referring to 2 ½ hoseline off E-11)
- E-3 is relocated to Station 16/19
- Mutual aid department # 1 on-scene
1925 hours
- E-10 radios that tank water is down to one-quarter full
- Fire Chief radios E-12 to boost supply water pressure to E-10 by 50 more pounds
- E-12 acknowledges
- Mutual aid department # 1 radios the fire department with no response
1926 hours
- E-16 engineer radios that water coming
- Dispatch radios Fire Chief and informs him that dispatch has received a phone call from a civilian saying he is trapped at the rear of the building
- Fire Chief acknowledges
1927 hours
- Inaudible radio traffic possibly lost inside or trapped inside
- Fire Chief radios AC and says that the warehouse door has been opened and a 2 ½ hose line is in operation. Fire Chief also asks about the rescue attempt of the trapped civilian and tells AC to do what he can do.
- Dispatch radios AC to inform him that the trapped civilian is banging on exterior wall with a hammer
1928 hours
- AC radios for E-11 and gets no response. Note: This may be when the AC is looking for fire fighters to assist with rescue of the civilian and mutual aid fire fighters are pressed into action.
1929 hours
- Broken radio traffic of fire fighter in distress asking which way out then everyone out
1930 hours (see Photo # 2)
- E-11 radios that 2 ½ hose line is charged
- Several different fire fighters in distress radio need some help out, need help getting out, also lost connection with the hose
- AC radios Fire Chief that they are attempting to free civilian trapped in warehouse
1931 hours 1934 hours (see Photo #3)
- More broken radio traffic from fire fighters in distress
- L-5 repositioned to D-side by off-duty fire fighters
- Fire Chief asks for E-3 to come to scene and lay supply line to L-5
- BC-5 reports civilian is out of building
- E-16 engineer radios dispatch that police department is needed to prevent traffic from running over supply line.
- FF calls Mayday
- Fire Chief asks AC is everyone out? AC responds the civilian is out
- Fire Chief radios AC to make sure his people are accounted for.
- E-15 FF exits building (out of air) reports he didnt call the Mayday
- Fire Chief radios who called Mayday
- Fire Chief radios we need to vacate the building
- Dispatch tells Fire Chief that the L-5 engineer emergency button (on radio) has been activated
- Fire Chief radios for E-15 captain with no response
- E-15 FF changes air cylinder and goes back inside
1935 hours 1936 hours (see Photos # 4, # 5, and # 6)
- Front windows knocked out
- E-6 crew (captain, engineer, and FF) along with E-15 engineer and FF exit showroom
- Fire Chief orders mutual aid crew to search for missing fire fighters
- Fire Chief continues to radio for E-15 captain and crew with no response
- Fire Chief instructs everyone else to stay off radio
- Conditions at front of showroom change dramatically turbulent thick dark smoke rolls out windows
1937 hours
- Fire Chief continues to radio for E-15 captain and crew with no response
- E-13 is dispatched to scene
- E-7 relocates to Station 13
- Fire rolls out windows at front of showroom
1938 hours (see Photos # 7 and # 8)
- Mutual aid crew exits building
- Fire Chief continues to radio for E-15 captain and crew with no response
- Fire Chief radios for everyone to abandon the building
- Training Chief (BC-T) radios for E-15 captain
- BC-T radios E-16 engineer to boost water supply pressure to E-11.
1939 hours
- AC radios E-16 to give me some more water
- BC-T also radios E-16 for more water pressure
- E-16 engineer acknowledges and water pressure is boosted to 200 psi
1940 hours
- E-3 on scene
- Mutual Aid Department # 2 enroute to lay water supply line to L-5
1942 hours
- BC-T continues to radio for E-15 captain (no response)
- Fire Chief radios that no one is to go inside
- E-13 on scene
1943 hours
- Fire Chief asks if everyone is out of front
- BC-T radios E-16 engineer that he needs more water pressure. Engineer responds that the entire hose bed has been stretched out plus two sections of 3 hose. Additional radio communications about civilian vehicle traffic driving over the supply line.
- BC-T radios E-16 engineer and says I need all you can give me!
1944 hours
- AC radios dispatch to call the city water department to increase water pressure in the area.
- Fire Chief radios for E-15 captain
- E-3 engineer radios that water is coming (water supply established to L-5)
Additional crews continued to arrive on-scene and contributed to the fire suppression efforts. Engine 13 began laying a supply line to L-5 at 1947 hours. The Fire Chief radioed dispatch to send Ladder 4 to the scene at 1948 hours. The Fire Chief radioed dispatch and requested that the Mayor be notified at 1950 hours. A portion of the roof over the right side of the showroom collapsed causing the front façade to begin collapsing at 1951 hours. Eventually, almost the entire roof over the main showroom and the right side addition collapsed. Ladder 4 was put into operation in the front parking lot at approximately 2005 hours. The fire was brought under control after 2200 hours. Recovery operations continued until after 0400 hours the next morning.
Personal Protective Equipment
The fire department issued each fire fighter a full set of black turnout gear and station uniforms when they were hired and sent to the recruit training class. The department issued helmets, hoods, gloves, and boots. The Chief Officers (Battalion Chief rank and higher) wore a set of brown turnout gear from a different manufacturer. At the time of the incident, each fire fighter was allowed to purchase and wear his own turnout gear, or bring their gear from other departments they served in, if they desired, so long as it met the requirements of the department.
Following the incident, the personal protective equipment (PPE turnout clothing, SCBA, radio, hand tools, etc) worn by each of the nine victims was secured by the city police department. On August 29, 2007, the PPE was examined in detail by a personal protective clothing expert contracted by NIOSH. The PPE was examined, documented and photographed through a systematic process. The county coroners office coordinated the PPE examination at the request of NIOSH. Representatives of NIOSH, NIST, the FRT, the county coroners office, the city police department, and the state fire marshals office were present during the examination. Each victims PPE was severely damaged by fire and heat exposure due to the length of time it took to locate and recover the victims. The evaluation indicated melting of polyester station uniforms (non-NFPA 19757 compliant) in the areas where the turnout clothing was degraded by the fire exposure. The PPE examination also identified examples where turnout gear was not being properly worn such as turnout coat collars not fully extended upward and helmet ear flaps not deployed. A summary of the complete PPE inspection is contained in Appendix IV. A copy of the complete PPE inspection report is available upon request from the NIOSH Fire Fighter Fatality Investigation and Prevention Program.
The city fire and police departments utilized a type-2 trunked radio system (computer-aided) that automatically assigned radio frequencies as needed to different talk groups. Each apparatus riding position was assigned a radio so that each on-duty fire fighter had access to a radio. Each radio contained an emergency notification button that, when activated, would send a signal to the dispatch center with the radios identity. On the day of the incident, radios were available, but at least one fire fighter did not carry his assigned radio. The county in which this incident occurred maintained its own dispatch center for emergency medical services (EMS) and the smaller outlying volunteer fire departments. Some smaller fire departments operated as public service districts (PSDs) and operated their own dispatch centers. Thus not all fire departments who were on scene could communicate directly with the city fire department due to the multiple radio systems in place.
Apparatus and Equipment Maintenance
The fire department operated a maintenance and repair facility at one of the stations, where in-house maintenance was performed on all fire apparatus, equipment and SCBA. Annual pump flow testing was conducted and recorded. During the NIOSH investigation, interviewed fire fighters reported a number of recurring maintenance problems on apparatus and power equipment to the NIOSH investigators.
During the NIOSH investigation, fire fighters reported during interviews that Engine 11 (E-11) required specific procedures to engage the pump. When interviewed by NIOSH investigators, the maintenance supervisor reported that E-11 had a hydraulic transmission and a non-electric pump, and if the engine was not throttled to full throttle before the pump was engaged, the pump would not discharge at full capacity. The city reported that there were no records or reports of operational issues with E-11 prior to this event, and that daily equipment checks were performed. In December 2008, the city contracted with a nationally recognized company to conduct independent testing and evaluation of E-11. The city indicated that no changes had been made to Engine 11 since the fire. A copy of the December 16, 2008 inspection report was provided to NIOSH for review (Appendix II). The results of this testing and evaluation indicated that Engine 11 was generally in good acceptable working order with 3 maintenance findings that were corrected during the inspection, and 8 findings needing corrective action. In addition, the report highlighted findings of the Engine 11 pump inspection. The report reads, When shifting the [pump] lever downward from top position, proper operation calls for a pause in center (neutral) position momentarily before bringing the lever to the complete downward position. Failure to pause at the center (neutral) position can cause a long excessive delay in engaging of pump. There is an expected delay even in proper operation of this pump. Please check with manufacturer for exact acceptable delay time line.
During the NIOSH investigation, fire fighters reported to NIOSH investigators that the fire departments procedure was to refill cylinders when the pressure dropped to 1500 psi which is well below the required 90% level found in the OSHA Respirator Standard8 and NFPA 18529 (1500 psi is 68% of full cylinder pressure or 2216 psi). NIOSH investigators examined a small number of SCBA cylinders in service on city fire apparatus and did find some with cylinder pressures below 2000 psi.
Structure
The structure involved in this incident was a one-story, commercial furniture showroom and warehouse facility totaling over 51,500 square feet that incorporated mixed-construction types. The structure was non-sprinklered. The facility had been renovated and expanded a number of times over the past 15 years. The original structure was constructed in the 1960s as a 17,500 square foot grocery store with concrete block walls and lightweight metal bar joists (metal roof trusses) supporting the roof to create an open floor plan. After being converted to a furniture retail store, the original structure was expanded by adding a 6,970 square foot addition on the right side (D-side) in 1994 and a 7,020 square foot addition to the left (B-side) in 1995. Both additions were attached to the original exterior walls and consisted of steel beams supporting the walls and roof. To provide access between the original structure and the two additions, the exterior walls on the B and D sides of the original structure were each penetrated in 3 locations to form six 8 X 8 openings that were equipped with metal roll-up fire doors. These fire doors were equipped with fusible links designed to automatically close the doors in the event of a fire. In 1996, a 15,600 square foot warehouse was added to the rear of the main showroom. The main showroom and the warehouse were connected by an enclosed wood-framed loading dock of approximately 2,250 square feet. Double metal doors connected the rear of the right-side addition to the loading dock area. These metal doors swung outward (opened into the loading dock). Additional access to the loading dock area was available from the rear of the original structure. (See Diagram 1)
At the time of the incident, the showroom included painted sheet-metal siding on the B and D side exterior walls with a combination of sheet metal and concrete block in the rear (C-side) and a front masonry and block façade (at the A-side). The roof over the main showroom (original structure) was constructed of sheet-metal roof decking covered by foam insulation and a weather membrane. Both right and left showroom additions included roofs constructed of sheet metal roof decking over fiber glass insulation. The fire caused extensive damage to the roof structure, making an analysis of the roof construction difficult.
The warehouse was a free-standing, clear-span structure with sheet-metal walls and roof. Both structures contained concrete floors. The main showroom measured 9 feet from the floor to a suspended drop ceiling and approximately 14 feet to the roof, creating almost 5 feet of void space above the suspended ceiling. The warehouse measured 29 feet from the floor to the roof. The warehouse contained rows of metal storage shelving that contained a variety of furniture items including couches, chairs, mattresses, etc. (see Photo 9 showing storage racks in warehouse).
The roofs over the main showroom, the showroom additions on both the B and D sides of the structure, and the warehouse contained limited penetrations (ventilation ductwork, utilities, etc.). Thus there were limited openings for smoke and hot gases to escape naturally in the event of a fire.
According to city building officials, the property was annexed into the city in 1990. The original structure and the 3 additions were considered as 4 separate structures for code enforcement purposes. Separate permits were issued for the construction of the left and right side additions and the warehouse. City building officials indicated to NIOSH investigators that after the fire, the furniture store property was determined to be non-code compliant (not in compliance with applicable codes). Work had been performed on the loading dock area and the maintenance shop without permits between 1996 and 2005. Other code violations included the accumulation of trash outside the loading dock, large quantities of flammable liquids, solvents, and thinners in the loading dock area, and storage of furniture and flammable materials in non-permitted areas.
At the time of the incident, city ordinances required commercial structures over 15,000 square feet to be equipped with a sprinkler system. The original structure was grandfathered (exempt from this requirement) while the left and right additions (at the B and D-sides) did not meet the threshold requirement. Thus, since the store was considered as 4 separate structures, the facility had been exempt from sprinkler system requirements.
The structure had been inspected by the fire department on a number of occasions. In 1987, fire inspection duties were transferred from the fire department to the city with the last documented fire code inspection by the city in 1998. The fire department continued to perform periodic pre-plan inspections. A building pre-plan form obtained from the fire department dated April 26, 2006 noted that store contents were household furniture and office equipment and that the rear warehouse contained racks approximately 30 feet high (see Appendix III). The pre-plan form did not mention the large volume of furniture and flammable materials (fuel load) contained in the structure. It was reported to NIOSH investigators by fire fighters during interviews that trash from the furniture business, including packing materials, cardboard, broken furniture and other flammable materials, were routinely stored against the building near the loading dock on the west (D) side of the structure (see Diagram 2).
Weather
At the time of the incident, the temperature was approximately 86 degrees Fahrenheit (F) with a dew point of 72 degrees F and a relative humidity of 63 percent. The sky was partly cloudy with light winds blowing from the south up to 11 miles per hour.10
INVESTIGATION
The furniture store fire on June 18, 2007, was originally dispatched as a possible fire behind a commercial retail furniture store. The initial Incident Commander radioed dispatch that the fire was a bunch of trash free-burning against the side of the structure. The fire very rapidly grew into an incident of major proportions. (A computerized fire model will be available in the future from NIST at http://www.nist.gov/el/). (Link Updated 1/17/2013)
Summary of Initial Sequence of Events
On June 18, 2007, at approximately 1907 hours, the fire department was dispatched to a possible fire behind a large commercial retail furniture store. Two engines (Engine 11 and Engine 10), one ladder truck (Ladder 5), and the Battalion Chief (BC-4) were dispatched per department procedures. The on-duty Assistant Chief (AC) was at Station 11 and responded to the scene. While enroute, BC-4 observed heavy dark smoke rising into the air and radioed dispatch that smoke was coming from the direction of the store. Per department procedures, this initiated the response of the third-due engine (Engine 16) to the scene.
BC-4 arrived on scene driving east to west, pulled past the store and drove down the alley to the loading dock located on the D-side of the structure. BC-4 observed fire burning from ground level to over the roofline outside of the covered loading dock. Note: The covered loading dock connects the front showroom area to the rear 15,600-square foot warehouse facility. BC-4 radioed dispatch that the fire was a bunch of trash free-burning against the side of the structure. The dispatcher asked the responding units if they heard BC-4s report on the fire conditions. E-10, L-5, and E-16 acknowledged.
When the AC arrived on-scene, he parked in the parking lot in front of the main showroom right addition. The AC and BC-4 briefly discussed their observations and directed Engine 10 to back down the alley to the loading dock area. The AC entered the store through the main entrance located in the center of the front of the structure (A-side). The AC walked down the center of the showroom to the rear (in the original structure) then went back outside. He did not observe any smoke or fire in the main showroom. BC-4 drove his car to the front of the showroom and observed the AC coming out of the showrooms main entrance. The AC remained at the front of the store while BC-4 returned to the D-side. Note: Departmental policy was that the highest ranking officer on-scene was the Incident Commander. Incident Command (IC) was never formally announced at this incident.
While the E-11 crew looked for a hydrant to establish water supply, the AC and the E-11 acting captain re-entered the main showroom. The AC radioed E-16 to come inside the front door when they arrived on scene. E-16 acknowledged. Ladder 5 (L-5) arrived on-scene at 1912 hours and pulled into the parking lot in front of the furniture store, facing east. BC-4 radioed the AC and informed him that the fire was now inside the structure. The AC radioed Dispatch and requested that Engine 12 (E-12) be sent to the scene. The Fire Chief advised the dispatcher to relocate Engine 15 (E-15) to Station 11. BC-4 radioed E-12 and instructed them to lay a supply line to E-10. E-12 acknowledged.
The Assistant Chief detected fire when he opened a door connecting the rear of the right showroom addition to the loading dock area. The E-11 acting captain radioed that he needed a 1 ½ hand line inside the building. When E-15 radioed that they had relocated to the west-side, the AC instructed E-15 to come to the scene. The AC also instructed E-15 to bring a 1 ½ hand line inside to the rear right-side of the structure. The AC radioed that the fire was inside the rear of the structure and was moving towards the showroom.
The E-11 acting captain went outside and met the L-5 crew pulling a 1 ½ hand line off E-11. The AC radioed dispatch and requested that Engine 6 (E-6) be sent to the scene. E-6 was dispatched at 1914 hours. The Fire Chief (enroute) radioed dispatch to change the assignment to have Engine 19 dispatched to the scene and have E-6 relocate to Station 11. E-16 radioed the AC to ask if they were to go to the rear of the building. The AC instructed E-16 to come to the front door and bring a 2 ½ hand line inside. The Fire Chief arrived on-scene at 1916 hours. Note: Beginning at approximately 1916 hours, the L-5 engineer is heard over the radio asking for the 1 ½ hose line from E-11 to be charged. Diagram 2 shows the location of Engine 10 and Engine 11 in relation to the structure and how the attack lines were deployed during offensive operations.
A mutual aid department noticed heavy black smoke in the area and self-dispatched to the scene. The fire had already spread to the warehouse when the mutual aid department arrived on-scene. After some discussion with the Fire Chief, the mutual aid department was assigned to the rear of the warehouse (C-side) to begin fire suppression.
The burning furniture quickly generated large volumes of smoke, toxic gases and soot that added to the fuel load. At approximately 1926 hours, a store employee called the citys 911 Dispatch center and reported that he was trapped inside the back of the building. Note: The employee was actually working near the front of the warehouse opposite the covered loading dock (see Diagram 3.) The employee stated he was banging on the exterior wall with a hammer. The dispatcher told the employee to continue banging on the wall and to stay calm and stay as low to the floor as he could. The dispatcher radioed the Fire Chief and informed him of the situation. This information was also relayed to the city police dispatcher and a police officer on-scene verbally informed some fire fighters of the situation. The city Assistant Fire Chief and a Battalion Chief (BC-5) quickly instructed a crew of four fire fighters from the mutual aid department to initiate the rescue attempt on the B-side of the warehouse. This crew quickly located the point where the trapped civilian was banging on the exterior wall. They were able to cut through the exterior wall (metal siding) using a Haligan bar and axe. The fire fighters were able to safely extricate the civilian at approximately 1933 hours. The civilian employee rescue was announced over the radio. The mutual aid fire fighters assisted the employee to the front parking lot where he was checked by EMTs.
As the civilian was being rescued, the fire was extending into the main showroom. The fire quickly outgrew the available suppression water supply. The interior fire attack crews could not contain the spread of the fire. Note: At this point, three hose lines were inside the main showroom the initial 1½ inch hose line, a 2½ inch hose line and a 1 inch booster line. All three hose lines were pulled off Engine 11 which was being supplied by Engine 16 through a single 2 ½ inch supply line approximately 1,850 feet long. Water supply from Engine 16 to Engine 11 was established at approximately 1926 hours. The interior crews from Engine 11, Ladder 5, Engine 16, Engine 15, Engine 19, and Engine 6 became disoriented as the heat rapidly intensified and visibility dropped to zero as the thick black smoke filled the showroom from ceiling to floor. The interior fire fighters realized they were in trouble and began to radio for assistance. At least one Mayday was called. Another fire fighter radioed that he had lost contact with the hose line and needed help. One fire fighter activated the emergency button on his radio.
Note: During this incident fire fighters experienced intermittent radio communication problems and interruptions. Audio transcripts of the fireground channel recorded multiple instances where fire fighters inside the structure (including some of the victims) transmitted over the radio but the transmissions were not heard or not understood. The first recorded transmission of a fire fighter requesting assistance occurred at approximately 1927 hours and transmissions requesting we need help, lost connection with the hose, and Mayday continued until at least 1934 hours. The first Mayday was recorded at approximately 1932 hours. The first recorded transmissions indicating chief officers were aware of the fire fighters calling for assistance was at approximately 1933 hours.
The Engine 6 crew and three fire fighters from E-15 were able to find the front door and exit the showroom. The front showroom windows were knocked out to improve visibility. Fire fighters, including two fire fighters from the mutual aid crew who extricated the trapped civilian, were sent inside to search for the missing fire fighters at approximately 1936 hours. The two mutual aid fire fighters made brief contact with two disoriented fire fighters just as the flammable mixture of gases and combustion by-products in the showroom ignited, filling the showroom with flames. The two mutual aid fire fighters lost contact with the two disoriented fire fighters and were driven outside by the intense heat and flames (see Photo 7). One of the rescuers received second degree burns on his face, neck, hands, and arms. An off-duty Battalion Chief and the Engine 6 engineer also entered the structure for a rescue attempt. They also were driven out by the rapid fire spread.
While fire fighters were known to be trapped inside, the number and their identities were not known. Interior fire fighters were caught in the rapid fire progression and nine fire fighters from the first-responding fire department were killed.
The operational details of each responding apparatus company are listed below. Per department procedures, chief officers requested additional apparatus as the need was identified.
Engine 10The E-10 crew (consisting of a captain, engineer, and fire fighter) was in-transit returning to quarters when the fire dispatch came in. The crew could see smoke billowing from the incident scene as they pulled onto the highway and they heard BC-4 report over the radio a trash fire on the side of the structure. Note: E-10 and Ladder 5 are quartered at the same station. The fire fighters on E-10 and L-5 had switched positions so that another fire fighter could train on pumping E-10.
The AC and BC-4 were already on-scene when Engine 10 arrived. The AC directed E-10 to back down the alley parallel to the D-side of the store toward the loading dock. The crew observed smoke and flames inside the loading dock area and coming out an exhaust fan in the D-side wall. The E-10 captain pulled a booster line (1 red hose) and knocked down the outside trash fire while the E-10 fire fighter pulled a 1 ½ pre-connected hand line to the loading dock. BC-4 returned to the loading dock after meeting with the AC and observed fire burning inside the structure so he radioed dispatch to report that the fire was now inside the building. The E-10 captain decided to use the 1 ½ hand line for the interior attack. The E-10 engineer charged the 1 ½ hand line from the engines tank-water supply. Fire was readily visible inside the loading dock area as the E-10 fire fighter and captain advanced the hoseline inside the loading dock about 20 to 25 feet. At their furthest point of entry, the E-10 crew could just see the door connecting the enclosed loading dock to the showroom right-side addition. This area became fully involved in flames as the E-10 crew directed water onto the fire. The 60 gallons per minute (gpm) flow from their 1 ½ handline was insufficient to control the fire. According to the fire fighters interviewed by NIOSH, the flames appeared to float in the air and burned floor to ceiling. The water didnt appear to have any effect on the fire so the crew started to retreat. Note: The E-10 crew told NIOSH investigators that the water pattern produced by their fog nozzle just pushed the flames around the room as they attempted to extinguish the fire. After the fire, at least 28 one-gallon cans of extremely flammable solvents were found inside the loading dock suggesting that at some point a vapor fire was burning inside the loading dock. As they were backing out, the hose either burst or was burned through by the fire. Water spraying from the ruptured hose aided the fire fighters (improved visibility and provided a protective water curtain) in locating the door and moving outside.
The E-10 engineer pulled some sections of 2 ½ supply line from E-10 out to the street to meet E-12 which had been assigned to provide a water supply line. When the E-10 attack crew exited the loading dock, they asked fire fighters from Engine 12 (E-12), just arriving on-scene, to repair the damaged 1 ½ hand line. The E-10 captain and fire fighter got the 1 booster line that they had previously pulled off E-10 and advanced the booster line to the loading dock door. The booster line did not have any effect on the fire so they backed the line out, switched back to the 1 ½ hand line (that had been repaired by the E-12 crew) and moved back inside the loading dock. By this time the Fire Chief was on scene. The Fire Chief came to the loading dock and yelled inside to tell the E-10 captain not to advance any further. A few seconds later, the Fire Chief ordered the E-10 crew to back outside and operate from the doorway. Note: The E-10 crew was inside the loading dock 3 times for a total of approximately 15 minutes. BC-4 observed that the fire had extended into the warehouse. BC-4 returned to the front of the building and asked the manager if he had keys for the warehouse at the rear of the loading dock. The manager said no, so BC-4 returned to the loading dock and directed the E-12 crew and off-duty fire fighters who had responded to the scene to cut through the warehouses roll-up door with a power saw. The crews experienced trouble with getting the saw to run properly and used axes and Haligan bars to open the warehouse doors. BC-4 also directed the E-10 crew to assist with opening up the warehouse. BC-4 then directed the E-10 crew to get a 2 ½ hand line with a stack-tipped nozzle from E-10 and pull it to the warehouse door. By this time, the warehouse was becoming well involved. A second 2 ½ hose line was later pulled from E-10 and put into operation.
BC-4 was able to look inside the warehouse and he observed a large amount of fire inside. BC-4 went back to the front of the building and directed 2 off-duty fire fighters to move Ladder 5 to the D-side and set it up for aerial water pipe operation. BC-4 also met with an off-duty captain and asked him to take over getting L-5 set up for operation. Note: This off-duty captain is also an Assistant Chief at a neighboring mutual aid fire department located about 20 miles away. A crew from the mutual aid department responded and the captain used this mutual aid crew to assist with establishing water supply to L-5 by supplying it with tank water and then stretching supply lines to Engine 12. Per department procedures, off-duty fire fighters are allowed to respond to working fires and become involved in fire suppression activities. Off-duty fire fighters are supposed to check in with the IC, give the IC their ID card or drivers license, and get an assignment. The civilian owner of a small yellow frame building located next to the D-side of the furniture warehouse advised BC-4 that his building was full of vehicles, gasoline, oil, and other flammables (see Diagram # 2). BC-4 talked to the deputy chief of the first mutual aid department about the building and asked him to get a hand line to protect the yellow building. Once L-5 was put into operation at approximately 1944 hours, it also was used to protect this building.
Engine 11The Engine 11 (E-11) crew (acting captain, acting engineer, and fire fighter) was in quarters at Station 11 and the engine was being washed when the fire dispatch was initiated. The AC and BC-4 were also at station 11. E-11 was the first due engine but Engine 10 was in the vicinity and arrived on-scene first. While enroute to the scene, the E-11 crew heard BC-4 radio that smoke was coming from the location of the furniture store. The original fire dispatch stated that the fire was at the rear, so E-11 turned left off the highway onto a side street and drove behind the building. The AC radioed for E-11 to come back to the front of the store and pull into the second entrance to the parking lot. E-11 circled around and turned right into the parking lot in front of the store just as E-10 backed down the alley on the D side. E-11 got on scene at 1911 hours just before BC-4 radioed that the fire was inside the structure. The acting captain on E-11 directed the E-11 acting engineer and fire fighter to lay a supply line to E-10. The E-11 fire fighter (suction man) started walking down the street looking for a hydrant. The E-11 fire fighter returned to E-11 before making a hydrant connection when Ladder 5 (L-5) arrived on-scene. The E-11 acting engineer was directed by the L-5 acting captain to reposition E-11 near the front door facing northeast.
The E-11 acting captain entered the main showroom doors and walked down the center aisle to the rear of the main showroom. The showroom was clear with no smoke visible inside. The AC had preceded the E-11 acting captain inside the showroom and the two walked into the right addition and walked to the rear of the right showroom addition. They both observed a small wisp of light smoke visible at ceiling level in this area. They were not immediately alarmed by this smoke and the AC opened the double door leading to the loading dock. They reported seeing lots of fire and smoke beyond the door. The AC attempted to pull the door shut but he could not shut the door due to the air rushing from the showroom toward the fire. The E-11 acting captain helped pull the door shut and the AC told the acting captain to get a 1 ½ hand line.
At 1913 hours, the E-11 acting captain radioed that he needed an inch-and-a-half inside the building. The E-11 acting captain then went outside and met the acting captain from Ladder 5 (L-5) pulling a 1 ½ preconnected hand line off E-11. They both pulled the 1 ½ pre-connected hand line through the center doors and down the center aisle. The hand line just reached the rear of the center showroom. The E-11 acting captain told the L-5 acting captain he was going to go outside to add in another section of hose. The E-11 acting captain added 5 more sections of 1 ½ hose (the second pre-connected hose line on E-11) and dragged it inside. The L-5 acting captain and L-5 fire fighter were at the nozzle at this time. The L-5 crew pulled the nozzle toward the rear of the right side addition (the line was still not charged at this point). The E-11 fire fighter entered the main showroom flaking more slack in the hose line. The E-11 acting captain asked him to go find out why they did not yet have water pressure on the 1 ½ hose.
After waiting a short time for water pressure, the E-11 acting captain went outside to find out why they still didnt have water pressure. The E-11 acting captain and engineer were able to get the pump in operation by cycling the engine transmission to get the pump in gear. Note: Fire fighters interviewed by NIOSH stated that E-11 required specific procedures to engage the pump; an independent inspection of the apparatus confirmed these findings. On the day of the incident, the E-11 engineer was serving as the acting captain so E-11 was driven and operated by a fire fighter less experienced in its operation.
The E-11 acting captain then re-entered the structure. He had to don his facepiece and go on air because gray-colored smoke was starting to accumulate in the center of the showroom. Fire was still not visible in the showroom at this point.
The Engine 16 (E-16) captain and fire fighter entered the showroom with a 2 ½ hose line that was uncharged at this point. The E-11 acting captain told the E-16 captain he would go find out why the 2 ½ hose line was still uncharged. As he started to exit the showroom, the inside conditions changed very rapidly. The smoke turned very thick and grayish black. The E-11 acting captain had to find the 1 ½ hose and follow it outside. E-11 was still without a water supply at this point. After talking with the E-11 acting engineer about the water supply situation, the E-11 acting captain walked around to the loading dock area to look for the E-11 fire fighter.
While at the D-side, BC-4 asked the E-11 acting captain to help with setting up a 2 ½ hose line to the warehouse. Note: This 2 ½ hose line was pulled from E-10. The E-11 acting captain was just stepping up to the warehouse door when the Fire Chief ordered everyone out of the warehouse. The E-11 acting captain observed that the other fire fighters in this area had things under control so he went back to the A-side. When the E-11 acting captain returned to the front, fire was blowing out the front windows. He heard the Fire Chief give an order to evacuate. The E-11 acting captain got into the E-11 cab and sounded the airhorn 3 times for an evacuation signal.
Ladder 5Ladder 5 (L-5) was the third apparatus to arrive on-scene and initially positioned in the parking lot in front of the furniture store just west of E-11. The L-5 crew included an acting captain (Victim # 7), an assistant engineer (Victim # 4) and a fire fighter (Victim # 9 - who had switched assignments with the E-10 fire fighter). Note: This fire department typically dispatches ladder trucks as extra manpower, and not for ventilation activities. The ladder trucks do not have their own pumps and must be supplied by an engine in order to flow a master stream.
The L-5 acting captain directed the E-11 acting engineer to reposition E-11 near the front door of the main showroom. It is assumed that the L-5 acting captain heard the E-11 acting captain radio for a hand line inside the structure so the L-5 crew started to pull a 1 ½ preconnected hand line off of E-11. When the L-5 crew took this hand line inside, they met the E-11 acting captain coming outside to get a hose line. The L-5 crew took the 1 ½ hose line to the rear of the right-side addition (after the E-11 acting captain added additional sections to the hose line) and after some delay in getting water, advanced into the loading dock through the double doors connecting the showroom to the loading dock. This was the last confirmed location of the L-5 crew.
Between approximately 1932 and 1934 hours, L-5 was repositioned from the front of the showroom to the D-side by off-duty fire fighters who had responded to the scene. Fire fighters from a mutual aid department along with off-duty fire fighters worked to establish water supply to L-5. Engine 3 arrived on scene at approximately 1940 hours and also worked to get a water supply established to L-5. Water supply was established at approximately 1944 hours.
Engine 16At the time of the incident, Engine 16 (E-16) was designated as the 3rd due engine on all confirmed structure fires in the departments western district if not assigned on the initial dispatch. Note: NIOSH investigators were told that the 3rd due engine is designated as the Safety Team and should have been held on stand-by at the scene. However, the crew was instructed to engage in fire suppression activities before they arrived on-scene.
The crew was in quarters when the fire dispatch was initiated. The E-16 crew consisted of a captain (Victim # 5), an engineer, and a fire fighter (Victim # 3). E-16 started to move toward the scene when BC-4 reported smoke in the area. At approximately 1915 hours, the AC radioed E-16 to bring a 2 ½ hose line in the front door. E-16 arrived on scene driving west to east. The E-16 captain and fire fighter dismounted the engine and went to talk to the AC. They took a 2 ½ hose line with a stacked-tip nozzle (uncharged) into the main showroom and advanced it to the double doors leading to the loading dock and met up with the acting captain from E-11. This was the last confirmed location of the E-16 crew.
The E-16 engineer was instructed to lay a supply line for E-11 so he drove east on the highway toward where a hydrant had been previously located. This hydrant had been removed in 2004 because it had received damage from heavy truck traffic in the immediate area. He continued east to the next hydrant located approximately 1,200 feet away. Note: 1,850 feet of a single 2 ½ supply line was stretched from E-11 to the hydrant. The E-16 engineer reported hearing the radio traffic about the civilian worker being trapped in the rear of the building just as he was pulling up to the hydrant. (see Diagram # 2)
At approximately 1919 hours, the E-16 captain radioed to charge the 2 ½ hoseline (inside the building). The E-11 engineer radioed the E-11 acting captain to ask if he wanted the 2 ½ hoseline charged. The AC responded to not charge the 2 ½ hoseline until the supply line from E-16 to E-11 was charged. Note: Water supply from E-16 to E-11 was not yet established at this point. Water supply from E-16 to E-11 was established at approximately 1926 hours. After the hose was stretched out, traffic on the highway began to drive over the supply line from E-16 to E-11. The E-16 engineer radioed dispatch that the city police were needed for traffic control. As crews attempted to battle the escalating fire, water supply became an issue. Later, during the time period from 1937 hours to 1941 hours, chief officers in front of the showroom repeatedly called the E-16 engineer to boost water pressure to E-11 as the fire escalated out of control. At approximately 1941 hours, the E-16 engineer was instructed to switch to another radio channel to clear up the main channel for rescue purposes.
Engine 12The Engine 12 (E-12) crew, consisting of an acting captain, assistant engineer, and two fire fighters were in quarters at the time of the initial dispatch. At approximately 1912 hours, the AC radioed dispatch to send E-12 to the scene. While enroute, BC-4 radioed E-12 and instructed them to lay a supply line down the alley on the D-side of the building to E-10. Engine 12 acknowledged this assignment. The Fire Chief also radioed the same instructions.
Engine 12 arrived on-scene at approximately 1917 hours and hooked up a 2 ½ supply line to E-10, then drove across the highway and down a side street to a hydrant, laying out 15 sections of supply line. The E-12 engineer hooked up to the hydrant and operated the pumps supplying E-10 throughout the incident. Water supply to E-10 was established at approximately 1920 hours. The E-12 acting captain and fire fighters assisted the E-10 crew by repairing the 1 ½ hoseline that had burst, then forced open the walk-thru door at the front of the warehouse and advanced a 2 ½ hoseline inside the warehouse about 10 feet before being ordered to withdraw. The 2 ½ hoseline was then operated through the doorway into the warehouse. The fire was reported to be burning so hot that the water immediately turned to steam and did little good in suppressing the fire.
Note: The E-12 crew reported that while forcing open the warehouse door, they experienced problems with a gasoline powered saw that had the wrong type of blade (for cutting plywood, not metal). Crews had to use axes to cut through the metal siding. The E-12 crew also cut holes in the metal siding along the D-side walls for ventilation and to direct water streams inside the building (see Photo 10).
Later in the incident, additional supply lines were stretched to E-12 so that E-12 could pump to E-11 and L-5 and L-4. Chief Officers radioed E-12 to boost the water pressure to E-10 at least 3 times during the incident. The E-12 engineer also radioed dispatch to have the city police department stop traffic on the highway from running over the supply lines.
Engine 15The Engine 15 crew was in quarters when the first alarm crews were dispatched. The E-15 crew consisted of a captain (Victim # 8), engineer, and two fire fighters. One of the E-15 fire fighters ( fire fighter # 2) was newly hired and was responding to his first working structure fire with the department. Per department procedures, E-15 began to relocate from downtown to the west side. The E-15 crew reported that smoke was visible from a couple of miles away as they relocated so they began running hot (Code 3 - lights and sirens on). At approximately 1912 hours, the Fire Chief radioed dispatch to have Engine 15 relocate to Station 11. Almost immediately, the AC radioed for E-15 to come to the scene. Then the AC radioed E-15 to bring a 1 ½ hose line to the right rear of the building.
Engine 15 arrived on-scene at approximately 1917 hours just as Engine 16 began dropping a supply line for Engine 11. The E-15 captain instructed the E-15 engineer to get dressed to go inside the building. Note: During the NIOSH interviews, numerous fire fighters reported that most fire fighters responding after the first alarm would be expected to enter a structure fire for additional interior support. Coordinated ventilation and ladder truck operations reportedly were seldom initiated.
The E-15 captain and two fire fighters donned their SCBA and proceeded to Engine 11. One fire fighter took a pike pole and Haligan bar while the other fire fighter took an axe. They briefly talked with the E-11 engineer. They observed two hose lines going through the front entrance and followed the hose lines (one 1 ½ and one 2 ½) inside. Visibility at the front of showroom was still good at this time and the crew did not go on air until they were about 10 feet inside the door. As the E-15 crew advanced further, the visibility decreased. They were aware of other crews working to their right. The E-15 captain discussed with his crew that he wanted to work a hose line to the center and left rear of the main showroom to cut the fire off from spreading in that direction (contain fire to the right rear corner). The E-15 captain instructed fire fighter # 2 to go outside and get a hose line.
Fire fighter # 2 went outside and pulled a booster line (1 red hose) as far as he could down the center walkway through the main showroom. By this point, the visibility had decreased to where it was difficult to distinguish other fire fighters moving nearby. Fire fighter # 2 moved as far as he could and then began to flow water from the booster line toward a red glow overhead. He ran low on air and followed the hoseline toward the front entrance. Once outside he changed his air cylinder, then followed the hoseline back inside. He heard airhorns sounding (evacuation signal)and followed the hoseline back outside.
The E15 engineer donned his PPE and went to the front door where he assisted fire fighter # 2 in pulling the booster line through the front door. The E15 engineer advanced inside the showroom about 10 feet where he encountered thick black smoke from ceiling to floor. He could see a red glow at the rear of the showroom but no distinct flames. He ran low on air and went outside and changed his SCBA cylinder then re-entered the main showroom. It was noticeably hotter inside the showroom as the E15 engineer entered the second time. The engineer heard three airhorn blasts then heard radio traffic about evacuating the building so he followed the hose line outside.
After the E-15 captain (Victim # 8) and fire fighter # 1 moved deeper into the showroom, the E-15 captain instructed fire fighter # 1 to go get another hose line. Note: This was the last confirmed location of the E-15 captain. Fire fighter # 1 found a charged booster hose and dragged this hose as far as he could in the direction of where he had last seen the E-15 captain. Fire fighter # 1 did not encounter the E-15 captain or his other crew members when he returned to the rear of the showroom. Fire fighter # 1 opened the hose line nozzle a couple of times but couldnt see much fire. Fire fighter # 1 noticed that it was starting to get really hot and the thickening smoke was reducing visibility to near zero. His low air alarm began to go off so he started to follow the hose line outside. He came to a point where the hose line ran underneath furniture and he couldnt follow the hose line any further so he jumped over the furniture. Once on the other side of the furniture, he searched for the hose line but could not locate it. As he searched for hose lines, he saw the bright flashing light of a PASS device and moved toward the light. He encountered the engineer from Engine 6 who was looking for his crew. The E-6 engineer guided the E-15 fire fighter to the front of the showroom and when they got close enough to the front entrance to hear the sound of Engine 11 running outside, the E-15 fire fighter bolted through the door (shortly after 1931 hours). The E-15 fire fighter went to Engine 11 and asked the E-11 engineer to switch out his SCBA cylinder. At approximately 1934 hours, while changing his cylinder, the E-15 fire fighter was asked if he had radioed a Mayday and he reported that he had not.
While changing cylinders, the E-15 fire fighter heard that fire fighters were missing inside the building. Note: During the timeframe of approximately 1935 to 1936 hours, fire fighters outside the main entrance knocked out the showroom windows to improve visibility inside the building. After changing cylinders, he followed the hose lines back inside the main showroom to search for his crew. He advanced about 50 feet into the showroom and encountered intense heat and could see fire burning everywhere around him. He met the E-6 crew (captain, engineer, and fire fighter) following the hoseline to exit the showroom. The E-6 engineer told the E-15 fire fighter he couldnt go any further and he needed to get out. These four fire fighters exited the showroom with the E-15 fire fighter jumping through a showroom window to the right of the doorway. The E-15 engineer and fire fighter # 2 also exited the main entrance at approximately the same time. The E-15 captain did not exit the building.
Engine 19The Engine 19 crew was in quarters when the fire dispatch was initiated. The Engine 19 crew consisted of a captain (Victim # 6), engineer (Victim # 1), and one fire fighter (Victim # 2). Engine 6 had just been dispatched to the scene when, at approximately 1914 hours, the Fire Chief radioed dispatch to send Engine 19 to the scene and to have Engine 6 relocate to Station 11.
Engine 19 arrived on scene at approximately 1920 hours and parked in the middle of the highway in front of the furniture store. The E-19 crew entered the main showroom through the front entrance. There are few details about their activities after this point.
Engine 6The Engine 6 crew, consisting of a captain, engineer, and one fire fighter were in quarters when they heard the initial fire dispatch. Engine 6 is the second engine to relocate to the western district per fire department procedures. At approximately 1914 hours, the AC radioed dispatch to send Engine 6 to the scene. When Engine 6 was dispatched, the Fire Chief radioed for Engine 6 to relocate to Station 11 and for Engine 19 to come to the scene. At approximately 1919 hours, the Fire Chief radioed for Engine 6 to come to the scene and to come in the front door. Engine 6 was already enroute (relocating to the west side) and acknowledged that they were enroute.
Engine 6 arrived on scene at approximately 1921 hours. The E-6 captain and E-6 fire fighter went to the front door and donned their SCBA masks. They followed the 1 ½ hose line into the building. The E-6 captain observed light smoke coming out the front door and also at the connection of the main showroom and the right side addition (exterior wall). Visibility was initially about 5 to 10 feet but visibility was reduced as they advanced into the showroom interior. There was little heat and the E-6 captain and fire fighter were able to walk into the showroom standing upright as they followed the hose line to the rear of the main showroom then into the right side addition. The E-6 engineer entered the showroom a couple of minutes later after donning his turnout gear, SCBA, and grabbing a pike pole from E-6. He reported the smoke at the front of the showroom was intensifying and beginning to bank down. He followed the 1 ½ hose line to the rear of the main showroom. A booster line reached only to the right rear side of the main showroom. He could hear other fire fighters talking in the direction the 1 ½ hose line was running (into the right addition) and began opening up sheetrock walls and pushing up ceiling tiles to look for fire extension.
The E-6 captain and fire fighter met other crews near the double doors to the loading dock. The other fire fighters stated they were going to get another hose line so the E-6 captain worked the nozzle of the 1 ½ hand line for approximately 5-6 minutes while the E-6 fire fighter attempted to pull slack in the line so they could advance closer to the fire in the loading dock area. The water pressure on the 1½ hose line fluctuated and at one point water pressure dropped to near zero. The E-6 captain attempted to radio outside to ask what happened to the water pressure but the on-off button on his radio had broken off during his entry so he couldnt turn on his radio. The E-6 crew noticed that the interior conditions suddenly deteriorated very rapidly with visibility decreasing and in less than 30 seconds, the heat became unbearable.
As the E-6 engineer was opening the walls and ceiling at the rear of the main showroom, three or four unidentified fire fighters approached him and frantically stated that they were running out of air and couldnt find the way outside. The E-6 engineer heard their low-air alarms sounding as they bumped into him then pulled away from him and disappeared into the smoke. This happened in a matter of seconds. During the short contact with the other fire fighters, the E-6 engineer was turned around several times and became separated from the hoseline. He moved in short circles until he found the hose line and began following it. Almost immediately, the E-6 engineer encountered another fire fighter (later identified as the E-15 fire fighter # 1) who also stated he was out of air and couldnt find his way outside. The E-6 engineer led the E-15 fire fighter along the hose line (at one point having to reverse directions) until they got within a few feet of the front door. They could hear the sound of Engine 11 running outside and the E-15 fire fighter ran outside, followed by the E-6 engineer. After checking on the condition of the E-15 fire fighter, the E-6 engineer re-entered the main showroom.
As the E-6 fire fighter was pulling slack in the 1 ½ hose line, another fire fighter, searching for the way out, ran into him and momentarily knocked him off the hose line. As the E-6 fire fighter regained the hose and stood up, water pressure in the hose was lost. At this point, the heat began to intensify and the E-6 fire fighter decided it was time to retreat. At the same time, he began hearing radio traffic of the Mayday followed by attempts by the Fire Chief and the dispatcher to identify who was calling Mayday and who had activated their emergency button.
As the heat rapidly intensified, the E-6 captain began following the hoseline outside. His low air alarm started to sound and he burned his hands feeling for the hose line. His facepiece began to pull down onto his face as he exhausted his remaining air supply. He encountered the E-6 fire fighter who told the E-6 captain he had the hose line and they began moving toward the front of the building. By this time, the E-6 captain was almost completely out of air and he bolted toward the front of the building. The E-6 engineer was following the hoseline back into the showroom looking for his crew and encountered the E-6 captain who was now out of air and becoming disoriented. The engineer grabbed his captain and guided him toward the front door until they could hear the sound of Engine 11 running outside. They made their way outside followed seconds later by the E-6 fire fighter and the E-15 fire fighter # 1. The front showroom windows were just being knocked out when the E-6 crew exited the showroom (see Photo 4).
Engine 9The Engine 9 (E-9) crew, consisting of a captain, engineer, and fire fighter were in quarters at Station 9 when they heard the fire dispatch. The crew monitored the fireground radio traffic and knew that a serious situation was developing. They heard the Fire Chief calling for additional resources and Engine 9 was dispatched to relocate to Station 10 and arrived at 1946 hours. At 1951 hours, E-9 was directed to drive past the incident site and stretch a 2 ½ supply line from the hydrant west of the site back to the site to Engine 13 to supply Ladder 4 before it arrived. After stretching the supply line, the E-9 crew worked on the D-side of the structure supporting fire suppression activities.
Engine 13The Engine 13 (E-13) crew consisting of a captain, engineer, and fire fighter were in quarters when they heard the fire dispatch. E-13 was dispatched to the scene at approximately 1937 hours and arrived on-scene at 1942 hours. The E-13 crew worked to help establish water supply to Ladder 5 by stretching a 2 ½ supply line from E-12 to L-5. The E-13 crew then assisted with fire suppression activities.
Engine 3The Engine 3 (E-3) crew consisting of a captain, engineer and fire fighter was out of service at a special event several miles outside of the city when they heard radio traffic about the fire. When they heard the incident was a confirmed structure fire, they began moving back to the city. At approximately 1924 hours, E-3 was directed to relocate to cover Station 16/19. At approximately 1931 hours, the Fire Chief called dispatch and requested the next closest engine company. E-3 was still enroute to Station 16/19 so the Fire Chief requested that E-3 come to the scene and lay a supply line to Ladder 5. At approximately the same time, L-5 was repositioned from in front of the structure to the D-side by off-duty fire fighters who had arrived at the scene.
E-3 arrived on-scene at 1940 hours. The E-3 suction man (fire fighter) took their 5 adaptor to connect to the hydrant, but E-19 (driven by the acting captain of E-11) arrived at the hydrant first. E-3 stretched a 2 1/2 supply line from E-19 (the next hydrant west of the structure) to L-5 and water supply was established at 1944 hours. After establishing water supply, the E-3 engineer stayed at the engine and the rest of the E-3 crew worked on the D-side of the structure operating a 2 ½ hand line. Fire fighters cut holes into the sheet metal siding and at one point, the E-3 fire fighter and an off-duty fire fighter attempted to advance a hoseline inside the showroom by crawling under the metal shelving located along the D-side wall. They were only able to advance 5 or 6 feet and had to withdraw because of the intense fire and heat inside the burning showroom.
Ladder 4The Ladder 4 crew consisting of an acting captain, engineer, and fire fighter were in-quarters at the time of the initial dispatch. The crew monitored the radio traffic and knew things were escalating. The Fire Chief radioed dispatch at approximately 1948 hours and requested that Ladder 4 be dispatched to the scene. At approximately 1952 hours, the Fire Chief radioed dispatch and requested Engine 9 be sent from Station 10 to lay supply line for L-4.
Ladder 4 was on scene at approximately 1956 hours and BC-4 directed the crew on where to position in the front parking lot. Portions of the showroom roof had already collapsed when L-4 got set up. Engine 19 began supplying water to L-4 at approximately 2002 hours through one 2 ½ supply line. At approximately 2006 hours, L-4 radioed the Fire Chief and requested another supply line be set up to L-4 so that both nozzles on the bucket could be put into operation. The mutual aid department laid a 4 supply hose to L-4. L-4 initially operated with 300 gpm flowing through one nozzle. L-4 operated at 750 gpm when the second supply line was set up.
Mutual AidJurisdictional boundaries separating the municipal fire department from surrounding fire departments were irregular and often intermingled. As commercial areas were annexed into the city, jurisdictional boundaries often split blocks. For example, the furniture store involved in this incident was within the citys jurisdiction. Residential structures directly behind the furniture store property that were within the same block were in the jurisdiction of a mutual aid fire department that operates as a public service district (PSD). This mutual aid fire department had 60 fire fighters operating from 4 stations and served a population of approximately 24,000 in an area of approximately 30 square miles. Note: This fire department operated its own dispatch system. This fire department routinely used positive pressure fans for ventilation purposes and routinely deployed thermal imaging cameras at structure fires.
Two crews from the mutual aid department were in close vicinity to the incident scene for a special event and noticed heavy smoke. The acting battalion chief (BC) for the mutual aid department (who was at the special event with the crews) radioed his dispatch and said the mutual aid crews were going to the scene. The dispatcher reported that the municipal fire department was already on scene. The acting battalion chief (BC), Engine 2 (E-2) with a crew consisting of an acting captain and an engineer / fire fighter, and Rescue 1 (R1) with a crew of an engineer and a fire fighter, proceeded to the scene and arrived at approximately 1924 hours. The BC radioed dispatch that they were on-scene and also requested that Engine 1 (E-1) be dispatched.
The BC immediately went to the D-side of the furniture showroom and talked with the city Fire Chief. The BC informed the Fire Chief he had two crews on scene and another crew on the way. The BC also offered the use of their thermal imaging camera and their large diameter (4) supply hose (LDH). According to the acting battalion chief, the city Fire Chief initially told him that the mutual aid departments assistance would not be needed. The BC asked the Fire Chief if he wanted the mutual aid department to cover the rear of the warehouse and the Fire Chief said yes.
At approximately 1925 hours, the BC directed E-1 to drive down the street at the rear of the warehouse and set up operations there. The BC also radioed dispatch to send Truck 1 (T-1). E-1 arrived on scene at approximately 1926 hours with a captain, engineer, and two fire fighters. E-1 connected to a hydrant located just east of the warehouse. The E-1 captain and fire fighters advanced a 1 ¾ preconnected hand line inside the warehouse through a door located on the B-side at the rear near the B-C corner at approximately 1930 hours.
Engine 2 (E-2) and Rescue 1 (R-1) parked in the middle of the highway in front of the main showroom. The two crews (two fire fighters on each apparatus) donned their turnout gear and proceeded to the D-side of the showroom to join up with their BC when a city police officer stopped them and said a male employee was trapped in the rear of the structure and had telephoned 911 for assistance. They proceeded to the front of the showroom and were directed by the city AC and BC-5 to assist them in rescuing the trapped employee. They radioed their dispatch at approximately 1928 hours that the city fire department wanted them to assist in rescuing the employee, then proceeded around the B-side of the showroom to the rear after knocking a lock off a wooden gate at the B-C corner to gain access (see Diagram 3).
The fire fighters located the area where the employee was banging on the exterior wall. The fire fighters used a Haligan bar and axes to cut through the metal siding and opened a hole large enough for the employee to crawl through. The mutual aid departments dispatch was notified at approximately 1931 hours that the employee had been rescued. The fire fighters assisted the employee to the front parking lot to receive medical attention. Note: The Assistant Chief of the municipal fire department radioed for an ambulance after the employee was extricated. Dispatch reported an ambulance was already in route.
The fire fighters returned to the front entrance and observed heavy black smoke filling the showroom and pushing out the door, but no visible fire. They observed city fire fighters yelling about fire fighters missing inside the structure. They reported hearing orders for the front showroom windows to be knocked out to improve visibility inside the showroom. The E-2 acting captain and R-1 engineer knocked out the windows to the right of the doorway while the city BC-5 knocked out the windows to the left of the doorway. The fire fighters noted that air rushed inside the showroom after the windows were knocked out. The E-2 acting captain cut his hand (requiring time off) while knocking out the windows. The E-6 and E-15 fire fighters (from the city department) exited the building at approximately 1935 hours while the windows were being knocked out. Some of the city fire fighters were completely out of air. At approximately 1936 hours, the Fire Chief instructed the mutual aid fire fighters to go inside and search for the missing city fire fighters. Two city fire fighters (an off-duty battalion chief and the E-6 engineer) also entered the showroom. The R-1 engineer and the E-2 fire fighter teamed up and followed the hoselines inside the front door a short distance. They encountered two fire fighters who were in distress. One was down on his hands and knees screaming for help and also attempting to drag the other fire fighter. The R-1 engineer attempted to assist the fire fighters while the E-2 fire fighter guided them back to the hose line. The showroom erupted in flames and the heat knocked the fire fighters to the floor, causing them to become separated. Both rescue teams were forced to evacuate. The E-2 fire fighter found the door first and assisted the R-1 engineer outside at approximately 1938 hours. They both reported hearing PASS devices going off inside the structure. The R-1 engineer received second degree burns to his face, hands, and arm.
The R-1 engineer reported that other fire fighters were just inside the door so another rescue attempt was made. An off-duty captain from the mutual aid department, along with city fire fighters, attempted to advance a 2 ½ hose line back inside the door, but their progress was quickly halted by the intense heat and fire and they were forced to retreat. At 1938 hours, the city Fire Chief radioed for everyone to stay outside and to abandon the building. One last attempt to enter the front entrance (by the off-duty battalion chief and the E-6 engineer) was stopped at the doorway by the intense fire and heat.
At approximately 1935 hours, the mutual aid BC requested that Engine 7 (E-7) be dispatched and come to the rear (C-side) of the warehouse with E-1. At approximately 1943 hours, the mutual aid BC requested Engine 4 (E-4) come to the scene. The BC directed E-4 to go the rear of the warehouse and set the deck gun. At approximately 1948 hours, the BC requested Truck 1 (T-1) to come to the scene.
The mutual aid BC radioed E-4 to hold up at the highway to let T-1 come down the back street first. T-1 arrived on scene at approximately 1950 hours and was set up at the rear of the warehouse to direct a master stream of water down onto the roof of the warehouse. At approximately 1952 hours, E-4 radioed the BC that the city fire department wanted E-4 to set up water supply to the city fire departments Ladder 4 (L-4) in the parking lot at the front of the main showroom. At approximately 2000 hours, the E-4 acting captain announced E-4 was pumping water to the citys L-4.
Water Supply
Water supply was a critical factor in the sequence of events leading up to the nine fatalities. Engine 10 should have been the second due engine and established the water supply to Engine 11. However, E-10 arrived first at 1911 hours and was directed to back down the alley to the loading dock on the D-side of the structure since that was where visible fire was located. Engine 11 positioned in front of the main showroom and the E-11 acting captain went inside the showroom while the E-11 fire fighter looked for a hydrant so E-11 could supply water to E-10. Engine 11 re-positioned closer to the main entrance when L-5 arrived in front of the showroom. Pre-plan information indicated the closest hydrant was located on the street behind the warehouse but this information was not utilized.
Engine 12 was dispatched at 1912 hours and directed to lay a single 2 ½ supply line to Engine 10. Engine 16 was already enroute as the third-due engine. Engine 16 arrived on scene at 1915 hours and Engine 12 arrived on scene at 1917 hours. Engine 12 stretched approximately 750 feet of 2 ½ supply line and had water supply established to E-10 at approximately 1920 hours. Engine 16 stretched approximately 1,850 feet of supply line and had water supply established to E-11 at approximately 1926 hours.
Both E-10 and E-11 put 1 ½ pre-connected hand lines into operation using tank water while waiting for supply lines to be established. The E-11 engineer reported experiencing problems with water pressure after water supply was established. The E-12 and E-16 engineers both radioed that vehicle traffic running over the supply lines were causing problems. Pressure had to be boosted by both E-12 and E-16 well above the 200 psi working limit of the supply hoses being used in order to accommodate for the friction losses and low water volume.
Adequate water supply for the size of the structure and fuel loads inside was never established and hose lines capable of attacking the fire with adequate fire streams were not deployed. Ladder 5 was not put into master stream operation until after the fire had escalated. Additional supply lines for Engine 11, Ladder 5 and Ladder 4 were laid after the fire had escalated.
E19 / E3 laid a second 2 ½ supply line to L-5 at approximately 1944 hours. BC-5 directed the acting captain on E-11 to drive E-15 west to the next hydrant to lay another supply line back to E-11. Then BC-5 told him to take E-19 instead. Engine 3 arrived on scene just as E-19 was positioning to the hydrant.
A small mutual aid department (mutual aid # 2) supplied L-5 with tank water at approximately 1940 hours until a supply line was established at approximately 1944 hours. A second supply line from E-12 to L-5 was also put into service after 2000 hours.
Ladder 4 was put into operation at approximately 2001 hours with a 2 ½ supply line laid by E-9. The first responding mutual aid department (mutual aid # 1) stretched a 4 supply line to L-4 at approximately 2005 hours so that both fire nozzles could be put into operation.
The mutual aid departments utilized 4 supply lines. After the larger diameter supply lines were put into service, the water pressure issues with L-4 and L-5 improved.
ADDITIONAL PHOTOS
Additional photos pertaining to the incident are available in Appendix V.
CAUSE OF DEATH
According to the county coroners report, the cause of death for all nine victims was carbon monoxide toxicity, smoke inhalation and thermal injury due to fire. Diagram 4 shows the approximate location where each of the nine victims was located inside the structure per the city.
RECOMMENDATIONS
Recommendation # 1: Fire departments should develop, implement and enforce written standard operating procedures (SOPs) for an occupational safety and health program in accordance with NFPA 1500.
Discussion: The risk for fatal injury among fire fighters is high compared to other occupations.11 There is an increasing body of scientific literature demonstrating that organizational practices that demonstrate top level management commitment to safety, establish and foster compliance with safety policies and practices, and involve workers in identifying safety hazards and promoting solutions are effective in reducing worker injuries.12-17 Many of these concepts are embodied in NFPA 1500, Standard for a Fire Department Occupational Safety and Health Program.18 Implementation of a strong fire department occupational safety and health program following written procedures and policies such as those outlined by NFPA 1500 can foster and improve the overall safety climate of a fire department, as well as improve specific safety and health areas, such as respiratory protection, risk management, training and competency in fireground operations, tactics, and equipment and apparatus use.
During this investigation, NIOSH investigators reviewed some written departmental SOPs. While these documents contained some individual SOPs, they mainly contained administrative guidelines and did not contain detailed fireground operation procedures that would enhance fire fighter safety and health, such as a risk management plan, a fire department occupational safety and health policy, and other components of a fire department occupational safety and health program as outlined in NFPA 1500.18
It is important to understand the difference between a policy and a procedure. A department policy is a guide to decision-making that originates with or is approved by top management in a fire department. Policies define the boundaries within which the administration expects department personnel to act in specified situations. A procedure is a written communication closely related to a policy. A procedure describes in writing the steps to be followed in carrying out organizational policies. SOPs are standard methods or rules in which an organization or a fire department operates to carry out a routine function. Usually these procedures are written in a policies and procedures handbook and all fire fighters should be well versed as to their content.19 Operational procedures that are standardized, clearly written, and mandated to each department member establish accountability and increase command and control effectiveness.19 The benefits of having clear, concise, and practiced SOPs are numerous. For example, they can become a training outline and a tool to guide fire department members. Above all, a well applied SOP improves departmental safety. 20
Recommendation #2: Fire departments should develop, implement and enforce a written Incident Management System to be followed at all emergency incident operations.
Discussion: National Fire Protection Association (NFPA) 1500 Standard on Fire Department Occupational Safety and Health Program, 2007 Edition,18 and NFPA 1561 Standard on Emergency Services Incident Management System, 2008 Edition,21 both state that an Incident Management System (IMS) should be utilized at all emergency incidents (including but not limited to training exercises). The U.S. Department of Labor, Occupational Safety and Health Administration has issued a guidance document intended to be used by agencies to prepare emergency response plans. The intent of the National Response Team (NRT) guidance is to provide a mechanism for consolidating multiple agencies plans into one functional emergency response plan or integrated contingency plan (ICP). 22
NFPA 1561, Chapter 3.3.29 defines the Incident Management System (also known as the Incident Command System (or ICS) as A system that defines the roles and responsibilities to be assumed by responders and the standard operating procedures to be used in the management and direction of emergency incidents and other functions.21 Chapter 4.1 states The incident management system shall provide structure and coordination to the management of emergency incident operations to provide for the safety and health of emergency services organization (ESO) responders and other persons involved in those activities. Chapter 4.2 states The incident management system shall integrate risk management into the regular functions of incident command. Each fire department or emergency services organization (ESO) should adopt an incident management system to manage all emergency incidents. The IMS should be defined and in writing and include standard operating procedure (SOPs) covering the implementation of the IMS. The IMS should include written plans that address the requirements of different types of incidents that can be anticipated in each fire departments or ESOs jurisdiction. The IMS should address both routine and unusual incidents of differing types, sizes and complexities. The IMS covers more than just fireground operations. The IMS must cover incident command, accountability, risk management, communications, rapid intervention crews (RIC), roles and responsibilities of the Incident Safety Officer (ISO), and inter-operability with multiple agencies (police, emergency medical services, state and federal government, etc.) and surrounding jurisdictions (mutual aid responders).
NIOSH investigators identified several examples in this incident in which recognized guidelines for IMS were not followed. Specific examples include multiple chief officers serving in command roles in an uncoordinated manner, lack of an established accountability system to track fire fighters on scene, a RIC was not established, an ISO was not assigned, and the fire department and police department did not work effectively together to control traffic and protect hoselines delivering water to the scene.
Recommendation # 3: Fire departments should develop, implement and enforce written SOPs that identify incident management training standards and requirements for members expected to serve in command roles.
Discussion: NFPA 1561, Chapter 4.8.3 states Responders who are expected to perform as incident commanders or to be assigned to supervisory levels within the command structure shall be trained in and familiar with the incident management system and the particular levels at which they are expected to perform. 21 NFPA 1001,61021,23 150018 and 152124 are just a few examples of recognized standards addressing fire fighter and officer qualifications.
One of the fire officers primary responsibilities is safety both on the fireground and during normal operations. A partial list of officer qualifications (knowledge, skills, and abilities) necessary to accomplish the primary responsibility of fireground safety identified in these standards include: fire behavior; building construction; conducting pre-incident planning; development applicable codes, ordinances, and standards; identification of fire and life safety hazards; supervising emergency operations; and, deploying assigned resources in accordance with the local emergency plan. Training records for the chief officers who initially responded to this incident were provided to NIOSH by the citys Safety Management Division. These records consisted mainly of NIMS certifications with little additional records to document specific training related to fire fighter and fire officer qualifications.
Recommendation #4: Fire departments should ensure that the Incident Commander is clearly identified as the only individual with overall authority and responsibility for management of all activities at an incident.
Discussion: NFPA 1561, Chapter 5 identifies the responsibilities and overall duties of the Incident Commander (IC).21 Chapter A.3.3.28 states The IC has overall authority and responsibility for conducting incident operations and for managing all incident operations at the incident site. There should be one, clearly identifiable Incident Commander for the duration of the incident, from the arrival of the first fire department unit until the incident is terminated. The Incident Commander must clearly be in charge of all fireground operations to ensure successful completion. If there is no established or single Incident Commander, fireground operations and incident conditions can break down.
Some of the key responsibilities of the Incident Commander, as detailed in NFPA 1561, Chapter 5.3, which are relevant to this incident include:
- Overall authority for the management of the incident (Chapter 5.3.1)
- Ensuring adequate safety measures are in place (Chapter 5.3.2)
- Establishing a stationary command post (Chapter 5.3.7.1)
- Continually conducting a thorough evaluation of the situation (Chapter 5.3.8)
- Maintaining an awareness of the location and function of all companies or units at the scene (Chapter 5.3.10)
- Overall responder accountability for each incident (Chapter 5.3.11)
- Initiating an accountability / inventory worksheet at the beginning of operations and maintaining that system throughout operations (Chapter 5.3.12)
- Evaluating the risk to responders with respect to the purpose and potential results of their actions in each situation (Chapter 5.3.17)
- Utilizing risk management principles (Chapter 5.3.19)
- Activities presenting significant risk to the safety of responders should be limited to situations having the potential to save endangered lives.
- Activities employed to protect property should be recognized as inherent risks to the safety of the responders and actions should be taken to reduce or avoid these risks.
- No risk to the safety of responders should be acceptable where there is no possibility to save lives or property.
- Developing the command organization for the incident (Chapter 5.3.20)
- Assigning intermediate levels of supervision and organizing resources following SOPs based on the scale and complexity of operations (Chapter 5.10.1.2)
- All supervisory personnel assigned to operations functions shall support an overall strategic plan, as directed by the Incident Commander, and shall work toward the accomplishment of tactical objectives (Chapter 5.10.1.3)
Chief Officers at the scene of an incident who are not officially a part of the command structure should refrain from giving tactical directions. One of the clear tenets of the Incident Command System is unity of command. By directing units outside of a role in the IMS, chief officers, by virtue of their rank, can create uncoordinated efforts outside the IMS which may not benefit the operational strategy and can actually have negative impacts upon the operational strategy. The resources that are taken from the operational structure to achieve the goals of the chief officers operating outside the IMS are lost to the tactical level operations or management elements that count on these resources to achieve their tactical objectives. During this incident, formal incident command was never formally announced or transferred as ranking officers arrived on scene. Fire attack operations at the loading dock (D-side) and the main showroom (A-side) were directed by different chief officers and were not coordinated.
Recommendation #5: Fire departments should ensure that the Incident Commander conducts an initial size-up and risk assessment of the incident scene before beginning interior fire fighting operations.
Discussion: Among the most important duties of the first officer on the scene is conducting an initial size-up of the incident. This information lays the foundation for the entire operation. It determines the number of fire fighters and the amount of apparatus and equipment needed to control the blaze, assists in determining the most effective point of fire extinguishment attack, the most effective method of venting heat and smoke, and whether the attack should be offensive or defensive. A proper size-up begins from the moment the alarm is received and it continues until the fire is under control. The size-up should also include assessments of risk versus gain during incident operations. 19, 25-29 Retired Chief Alan Brunacini recommends that the arriving IC drive partially or completely around the structure whenever possible to get a complete view of the structure. While this may delay the ICs arrival by a few seconds, this drive-by may provide significant details not visible from the command post.27 The size-up should include an evaluation of factors such as the fire size and location, length of time the fire has been burning, conditions on arrival, occupancy, fuel load and presence of combustible or hazardous materials, exposures, time of day, and weather conditions. Information on the structure itself including size, construction type, age, condition (evidence of deterioration, weathering, etc), evidence of renovations, lightweight construction, loads on roof and walls (air conditioning units, ventilation ductwork, utility entrances, etc.), and available pre-plan information are all key information which can effect whether an offensive or defensive strategy is employed. The size-up and risk assessment should continue throughout the incident.
Fires in commercial structures are typically more dangerous than residential building fires. Retired Assistant Chief Vince Dunn states that defensive operations should be used more often at special occupancy and commercial buildings. Chief Dunn cites statistics that 4 fire fighters die for every 100,000 residential fires compared to 9 fire fighter deaths for every 100,000 commercial structure fires.30
Interior size-up is just as important as exterior size-up. Since the IC is staged at the command post (outside), the interior conditions should be communicated to the IC as soon as possible. Interior conditions could change the ICs strategy or tactics. For example, if heavy smoke is emitting from the exterior roof system, but fire fighters cannot find any fire in the interior, it is a good possibility that the fire is above them in the roof system. Other warning signs that should be relayed to the IC include dense black smoke, turbulent smoke, smoke puffing around doorframes, discolored glass, and a reverse flow of smoke back inside the building. It is important for the IC to immediately obtain this type of information to help make the proper decisions. Departments should ensure that the first officer or fire fighter inside the structure evaluates interior conditions and reports them immediately to the IC.
In this incident, arriving officers concentrated on the A and D-sides of the structure. A complete 360 degree size-up was never conducted. Pre-plan information did not identify the potential hazards associated with the lightweight metal roof trusses, and the excessive fuel loads associated with the contents. Only one hydrant location was noted on the pre-plan form but it was not used. Smoke emitting from the connection between the original structure and the right-side addition, the deteriorating conditions in the main showroom, a rapid decrease in visibility coupled with a rapid rise in temperature, heavy smoke stains on windows, no visible fire in the showroom with a build-up of smoke and heat, and delays in establishing water supply, were all indicators that could have prompted consideration of switching from offensive to defensive strategies.
Recommendation #6: Fire departments should train fire fighters to communicate interior conditions to the Incident Commander as soon as possible and to provide regular updates.
Discussion: Proper size-up and risk versus gain analysis requires that the Incident Commander have a number of key pieces of information and keep informed of the constantly changing conditions on the fireground. New decisions must be made and old ones revised based upon increased data and improved information. Decisions can be no better than the information on which they are based. The Incident Commander must use an evaluation system that considers and accounts for changing fireground conditions in order to stay ahead of the fire. If this is not done, the attack plan will be out of sequence with the phase of the fire and the IC will be constantly surprised by changing conditions.27, 29, 31 Interior size-up is just as important as exterior size-up. Since the IC is staged at the command post (outside), the interior conditions should be communicated by interior crews as soon as possible to the IC. Interior conditions could change the ICs strategy or tactics. Interior crews can aid the IC in this process by providing reports of the interior conditions as soon as they enter the fire building and by providing regular updates. According to Chief Dunn, one such example would be whenever a suspended ceiling is discovered in a commercial structure, this information should be immediately communicated to the IC.31
Based on a review of the training curriculum and available fire department SOPs, fire fighters and officers at this department were not trained to communicate interior conditions to the outside. During the initial attack, the interior conditions in the front show room (lack of fire) did not match the exterior conditions on the D-side (loading dock area fully involved and also the amount of smoke overhead). During NIOSH interviews, fire fighters and officers who had operated inside the structure reported signs of deteriorating conditions to the NIOSH investigators. However, no interior condition reports were broadcast over the radio (to the chief officers or other fire fighters) during this incident. Verbal exchanges between the attack crews and chief officers took place but this information did not impact the tactics being used. Information concerning the interior conditions could have been used to consider changing from a fast attack mode to a more cautious defensive operation.
Recommendation #7: Fire departments should ensure that the Incident Commander establishes a stationary command post, maintains the role of director of fireground operations, and does not become involved in fire-fighting efforts.
Discussion: According to NFPA 1561, §5.3.1, The incident commander shall have overall authority for management of the incident. 21 In addition to conducting an initial size-up, the Incident Commander must establish and maintain a command post outside of the structure to assign companies and delegate functions, and continually evaluate the risk versus gain of continued fire fighting efforts. In establishing a command post, the Incident Commander shall ensure the following (NFPA 1561, §5.3.7.2):
- The command post is located in or tied to a vehicle to establish presence and visibility.
- The command post includes radio capability to monitor and communicate with assigned tactical, command, and designated emergency traffic channels for that incident.
- The location of the command post is communicated to the communications center.
- The incident commander, or his or her designee, is present at the command post.
- The command post should be located in the incident cold zone.
The use of a tactical worksheet can assist the IC in keeping track of various task assignments on the fireground. It can be used along with pre-plan information and other relevant data to integrate information management, fire evaluation and decision making. The tactical worksheet should record unit status, benchmark times, and include a diagram of the fireground, occupancy information, activities checklist(s), and other relevant information. This can also aid the Incident Commander in continually conducting a situation evaluation and maintaining accountability. 27 To effectively coordinate and direct fire fighting operations on the scene, it is essential that the IC does not become involved in fire fighting efforts. A delay in establishing an effective command post may result in confusion of assignments and lack of personnel and apparatus coordination which may contribute to rapid fire progression. The involvement of the initial IC in fire fighting also hampers the collection and communication of essential information as command is transferred to later arriving officers. In this incident, a stationary command post was never established and separate and uncoordinated activities were taking place in multiple locations. This contributed to a failure to size-up the overall incident scene, to properly evaluate risk versus gain, and to maintain accountability on the fireground.
Recommendation #8: Fire departments should ensure the early implementation of division and group command into the Incident Command System.
Discussion: The early establishment of divisions and groups allows the command structure of an incident to grow more effectively than simply deploying resources and assigning division or group supervisors after units are in place. Delegating division / group command to other officers makes the management of a large incident more feasible by relieving the Incident Commander of these responsibilities which allows the IC to focus on the bigger picture while still maintaining the ability to react to progress reports and other information provided by the division / group commanders. The Model Procedures Guide for Structural Firefighting describes the application of the National Fire Service Incident Management System (NIMS) to structure fire incidents. These procedures recommend the establishment of division and group command.32 In this incident, a strategy of coordinated division and group command was not employed.
Recommendation #9: Fire departments should ensure that the Incident Commander continuously evaluates the risk versus gain when determining whether the fire suppression operation will be offensive or defensive.
Discussion: The initial size-up conducted by the first arriving officer allows the officer to make an assessment of the conditions and to assist in planning the suppression strategy. The following general factors are important considerations during a size-up: occupancy type involved, potential for civilians in the structure, smoke and fire conditions, type of construction, age of structure, exposures, and time considerations such as the time of the incident, length of time fire was burning before arrival, and time fire was burning after arrival.33, 34 The Incident Commander must perform a risk analysis to determine what hazards are present, what the risks to personnel are, how the risks can be eliminated or reduced, and the benefits to be gained from interior or offensive operations.35 The size-up must include continued assessment of risk versus gain during incident operations. According to NFPA 1500 §A-8.3.3, The acceptable level of risk is directly related to the potential to save lives or property. Where there is no potential to save lives, the risk to the fire department members must be evaluated in proportion to the ability to save property of value. When there is no ability to save lives or property, there is no justification to expose fire department members to any avoidable risk, and defensive fire suppression operations are the appropriate strategy.18, 36 Retired New York City Fire Chief Vincent Dunn states When no other persons life is in danger, the life of the firefighter has a higher priority than fire containment.25
The first-responding officer, as well as the IC, needs to make a judgment as to what is at risk people or property. This will help determine the risk profile for the incident. Many fire fighters stand by the notion that all incidents are people events until proven otherwise. Some fire fighters are willing to concede that a fire environment has become too hostile to sustain life and therefore, the only thing left to save is property. Historically, the fire service has a poor history of changing risk-taking based upon the people/property issue.37
In this incident, the store manager was present to inform the chief officers on the status of employees and patrons who had been inside the business. The fire department utilized offensive strategies focused on fire suppression. Truck company operations (search and rescue, ventilation, etc.) were not utilized until the fire department received word that an employee was trapped at the rear of the structure. As conditions inside deteriorated, offensive strategies were continued even as problems with establishing water supply mounted and the civilian was rescued.
Recommendation #10: Fire departments should ensure that the Incident Commander maintains close accountability for all personnel operating on the fireground
Discussion: Personnel accountability on a fireground means identifying and tracking all personnel working at the incident. A fire department should develop its own system and standardize it for all incidents. Accountability on the fireground can be maintained by several methods: a system using individual tags assigned to each fire fighter, a riding list provided by the company officer, a SCBA tag system, or incident command board.18, 19, 21 Modern radio systems also incorporate a means of tracking the identity of fire fighters at an incident scene.
As the incident escalates, additional staffing and resources will be needed, adding to the burden of tracking personnel accountability. An incident command board should be established at this point with an assigned accountability officer or aide. The Incident Commander should also utilize the Incident Management System (IMS). Additionally, fire fighters should not work beyond the sight or sound of their supervising officer unless equipped with a portable radio.
In this incident, the only accountability system used was the daily work roster. Several off-duty fire fighters and mutual aid companies responded without being dispatched. Not all fire fighters entering the structure had their designated hand held radio. Fire fighters were known to be trapped inside the structure, but the number and their identities were not determined until their bodies were recovered.
Recommendation #11: Fire departments should ensure that a separate Incident Safety Officer, independent from the Incident Commander, is appointed at each structure fire.
Discussion: According to NFPA 1561 Standard on Emergency Services Incident Management System, 2008 Edition, paragraph 5.3, The Incident Commander shall have overall authority for management of the incident (5.3.1) and the Incident Commander shall ensure that adequate safety measures are in place (5.3.2). This shall include overall responsibility for the safety and health of all personnel and for other persons operating within the incident management system. While the Incident Commander (IC) is in overall command at the scene, certain functions must be delegated to ensure adequate scene management is accomplished.21 According to NFPA 1500 Standard on Fire Department Occupational Safety and Health Program, 2007 Edition, as incidents escalate in size and complexity, the Incident Commander shall divide the incident into tactical-level management units and assign an incident safety officer (ISO) to assess the incident scene for hazards or potential hazards (8.1.6).18 These standards indicate that the IC is in overall command at the scene, but acknowledge that oversight of all operations is difficult. On-scene fire fighter health and safety is best preserved by delegating the function of safety and health oversight to the ISO. Additionally, the IC relies upon fire fighters and the ISO to relay feedback on fireground conditions in order to make timely, informed decisions regarding risk versus gain and offensive versus defensive operations. The safety of all personnel on the fireground is directly impacted by clear, concise, and timely communications among mutual aid fire departments, sector command, the ISO, and IC.
Chapter 6 of NFPA 1521, Standard for Fire Department Safety Officer, defines the role of the ISO at an incident scene and identifies duties such as: recon of the fireground and reporting pertinent information back to the Incident Commander; ensuring the departments accountability system is in place and operational; monitoring radio transmissions and identifying barriers to effective communications; and ensuring established safety zones, collapse zones, hot zones, and other designated hazard areas are communicated to all members on scene.24 Larger fire departments may assign one or more full-time staff officers as safety officers who respond to working fires. In smaller departments, every officer should be prepared to function as the ISO when assigned by the IC. The presence of a safety officer does not diminish the responsibility of individual fire fighters and fire officers for safety. The ISO adds a higher level of attention and expertise to help the fire fighters and fire officers. The ISO must have particular expertise in analyzing safety hazards and must know the particular uses and limitations of protective equipment.26
A designated safety officer could have assisted at this incident with continual size-up, accountability, and timely communications regarding safety on the fireground and the rapidly deteriorating conditions inside the structure. Note: Since the fatal incident, the fire department has hired a full time, permanent Safety Officer.
Recommendation #12: Fire departments should ensure that crew integrity is maintained during fire suppression operations.
Discussion: Fire fighters should always work and remain in teams whenever they are operating in a hazardous environment.19 Team continuity means team members knowing who is on their team and who is the team leader; team members staying within visual contact at all times (if visibility is low, teams must stay within touch or voice distance of each other); team members communicating needs and observations to the team leader, and team members rotating together to rehabilitation, staging as a team, and watching out for each other (practicing a strong buddy system). Following these basic rules helps prevent serious injury or even death by providing personnel with the added safety net of fellow team members. Teams that enter a hazardous environment together should leave together to ensure that team continuity is maintained.25 In this incident, there were numerous instances where fire fighters were working independently, entering and exiting the structure alone, operating hose lines, pulling walls and ceiling, and other related activities. Working alone increases the risk for themselves, and possibly to others during search and rescue efforts. Federal regulations [the OSHA 2-in-2-out rule, 29 CFR 1910.134 (g)(4)(i)] states at least two employees enter the immediately-dangerous-to-life-or-health (IDLH) atmosphere and remain in visual or voice contact with one another at all times.8
Recommendation #13: Fire departments should ensure that a rapid intervention crew (RIC) / rapid intervention team (RIT) is established and available to immediately respond to emergency rescue incidents.
Discussion: A rapid intervention crew (RIC) or team (RIT) should be designated and available to respond during all fireground operations. 18, 19, 21 The rescue crew should report to the Incident Commander (IC) and be available within the incidents staging area. The rescue crew should be comprised of fresh, well-rested fire fighters, and be positioned and ready to respond when a fire fighter(s) is down or in trouble.18 NFPA 1500, Chapter 8.8, Rapid Intervention for Rescue of Members, provides detailed guidelines for the deployment of rescue teams at emergency incidents. Chapter 8.8.1 states The fire department shall provide personnel for the rescue of members operating at emergency incidents. During the initial stages of an incident, the rescue crew members may be engaged in support operations outside the structure. Once the incident expands in size or complexity and the IC requests additional resources, the rescue crew must be dedicated to stand-by in case rescue operations are needed.18 The rapid intervention crew or team should have all tools necessary to complete the job, e.g., search and rescue ropes, Haligan bar and flat-head axe combo, first-aid kit, resuscitation equipment, extra SCBA cylinders and/or transfill hoses, etc. RIC or RIT teams should have specialized rescue training to prepare them for rescue operations. RIC or RIT teams can intervene quickly to rescue a fire fighter who becomes disoriented, lost in smoke filled environments, trapped by fire, involved in a structural collapse, or has run out of breathing air. In this incident a dedicated rescue crew was never employed and no crews were held outside in standby or rescue mode. Once it was realized that fire fighters were trapped inside the structure, fire fighters from the first-responding mutual aid department as well as off-duty city fire fighters who came to the scene were pressed into service to attempt search and rescue operations at the front entrance.
Recommendation #14: Fire departments should ensure that adequate numbers of staff are available to immediately respond to emergency incidents.
Discussion: NFPA 1710 Standard for the Organization and Deployment of Fire Suppression Operations, Emergency Medical Operations, and Special Operations to the Public by Career Fire Departments (2004 Edition) contains recommended guidelines for minimum staffing of career fire departments.38 NFPA 1710 § 5.2.2 (Staffing) states the following: On-duty fire suppression personnel shall be comprised of the numbers necessary for fire-fighting performance relative to the expected fire-fighting conditions. These numbers shall be determined through task analyses that take the following factors into consideration:
- Life hazard to the populace protected
- Provisions of safe and effective fire-fighting performance conditions for the fire fighters
- Potential property loss
- Nature, configuration, hazards, and internal protection of the properties involved
- Types of fireground tactics and evolutions employed as standard procedure, type of apparatus used, and results expected to be obtained at the fire scene.
The NFPA standard states that both engine and truck companies shall be staffed with a minimum of four on-duty personnel. The standard also states that in jurisdictions with tactical hazards, high hazard occupancies, high incident frequencies, geographical restrictions, or other pertinent factors identified by the authority having jurisdiction, these companies shall be staffed with a minimum of five or six on-duty members.
NFPA 1710 also states that the fire departments fire suppression resources shall be deployed to provide for the arrival of an engine company within a 4-minute response time and/or the initial full alarm assignment within an 8-minute response time to 90 percent of the incidents as established in Chapter 4. The fire department shall have the capability to deploy an initial full alarm assignment within an 8-minute response time to 90 percent of the incidents as established in Chapter 4. The initial full alarm assignment shall provide for the following (Chapter 5.2.4.2):
- Establishment of incident command outside of the hazard area for the overall coordination and direction of the initial full alarm assignment. A minimum of one individual shall be dedicated to this task.
- Establishment of an uninterrupted water supply of a minimum 1520 L/min (400 gpm) for 30 minutes. Supply line(s) shall be maintained by an operator who shall ensure uninterrupted water flow application.
- Establishment of an effective water flow application rate of 1140 L/min (300 gpm) from two hand lines, each of which shall have a minimum of 380 L/min (100 gpm). Each attack and backup line shall be operated by a minimum of two individuals to effectively and safely maintain the line.
- Provision of one support person for each attack and backup line deployed to provide hydrant hookup and to assist in line lays, utility control, and forcible entry.
- A minimum of one victim search and rescue team shall be part of the initial full alarm assignment. Each search and rescue team shall consist of a minimum of two individuals.
- A minimum of one ventilation team shall be part of the initial full alarm assignment. Each ventilation team shall consist of a minimum of two individuals.
- If an aerial device is used in operations, one person shall function as an aerial operator who shall maintain primary control of the aerial device at all times.
- Establishment of an Incident Rapid Intervention Crew (IRIC) that shall consist of a minimum of two properly equipped and trained individuals.
The municipal fire department involved in this incident routinely operated with three fire fighters per apparatus depending on the staffing available during each shift. During this incident, many of the routine and necessary fireground operations were not initiated—e.g., establishment of Incident Command outside the hazard area overseeing all operations, search and rescue, a staged rapid intervention crew (RIC), hydrant connection and water supply, and coordinated ventilation. All resources on scene were engaged in attacking the interior fire. Due to the limited staffing, several fire fighters were operating alone inside the burning structure instead of pairing up with other fire fighters.
Recommendation #15: Fire departments should ensure that ventilation to release heat and smoke is closely coordinated with interior fire suppression operations.
Discussion: Ventilation is the systematic removal and replacement of heated air, smoke, and gases from inside a structure with cooler air. The cooler air facilitates entry by fire fighters and improves life safety for rescue and other fire fighting operations. Ventilation improves visibility and reduces the chance of flashover or backdraft.19 The ventilation opening may produce a chimney effect causing air movement from within a structure toward the opening. This air movement helps facilitate the venting of smoke, hot gases and products of combustion, but may also cause the fire to grow in intensity and may endanger fire fighters who are between the fire and the ventilation opening. For this reason, ventilation should be closely coordinated with hose line placement and offensive fire suppression tactics. Close coordination means the hose line is in place and ready to operate so that when ventilation occurs, the hose line can overcome the increase in combustion likely to occur. If a ventilation opening is made directly above a fire, fire spread may be reduced, allowing fire fighters the opportunity to extinguish the fire. If the opening is made elsewhere, the chimney effect may actually contribute to the spread of the fire.19, 39 Proper ventilation during a structure fire will reduce the tendency for rising heat, smoke, and fire gases, trapped by the roof or ceiling, to accumulate, bank down, and spread laterally to other areas within the structure. Proper ventilation reduces the threat of flashover by removing heat before combustibles in a room or enclosed area reach their ignition temperatures. Proper ventilation reduces the risk of a backdraft by reducing the potential for superheated fire gases and smoke to accumulate in an enclosed area.
The Incident Commander must consider many variables when deciding upon the plan of attack at a structure fire. Ventilation is just one of the many variables that must be considered. Before initiating the fire attack, the IC should ask the following questions:19
- Is there a need for ventilation at this time?
The need must be based upon the heat, smoke, and gas conditions within the structure, the structural conditions, and the life hazard - Where is ventilation needed?
This involves knowing the construction features of the building, the contents, exposures, wind direction and strength, extent of the fire, location of the fire, location of top or vertical openings and location of cross or horizontal openings - What type of ventilation should be used?
Horizontal (either natural or mechanical) or vertical (natural or mechanical)? - Do fire and structural conditions allow for safe roof operations?
Knowledge of the building is paramount.
In this incident, the fire department did not attempt to coordinate ventilation with the offensive interior attack. Chief officers interviewed by NIOSH stated they would not ventilate the type of structure involved in this fire. Crews were directed to attack the fire with hose lines at the loading dock (D-side) and inside the showroom at the right rear addition. Every fire fighter interviewed by NIOSH who was inside the showroom area reported rapidly deteriorating conditions as thick gray and black smoke banked down to floor level reducing visibility to near zero with rapidly intensifying heat. Different ventilation techniques such as cutting holes in the roof or high on the D-side wall may have helped reduce the accumulation of smoke and hot gases inside the showroom. The use of a positive pressure fan at the front entrance along with adequate openings to vent the introduced air, may have helped reduce the amount of accumulating smoke in the front showroom and improved visibility, possibly allowing the disoriented fire fighters inside to find the front entrance.
All ventilation techniques have both a positive and negative aspect. Venting can be a very effective life safety procedure. When venting for life safety purposes, the principle is to pull the fire, heat, smoke and toxic gases away from victims, stairs, and other egress routes. A vent opening made between the fire fighter or victims and their path of egress could be fatal if the fire is pulled to their location or cuts off there path of egress.39 Note: The NIST Fire Dynamic Simulator, a computational fire model, will examine the possible impact of different ventilation strategies and their effect on this incident. The NIST fire model will be available in the future at http://www.nist.gov/el/. (Link Updated 1/17/2013)
Recommendation #16: Fire departments should conduct pre-incident planning inspections of buildings within their jurisdictions to facilitate development of safe fireground strategies and tactics.
Discussion: National Fire Protection Association (NFPA) 1620 Recommended Practice for Pre-Incident Planning, 2003 Edition, § 4.4.1 states the pre-incident plan should be the foundation for decision making during an emergency situation and provides important data that will assist the Incident Commander in developing appropriate strategies and tactics for managing the incident. This standard also states that the primary purpose of a pre-incident plan is to help responding personnel effectively manage emergencies with available resources. Pre-incident planning involves evaluating the protection systems, building construction, contents, and operating procedures that can impact emergency operations. 40 A pre-incident plan identifies deviations from normal operations and can be complex and formal, or simply a notation about a particular problem such as the presence of flammable liquids, explosive hazards, modifications to structural building components, or structural damage from a previous fire.29, 30, 40
In addition, NFPA 1620 outlines the steps involved in developing, maintaining, and using a pre-incident plan by breaking the incident down into pre-, during- and post-incident phases. In the pre-incident phase, for example, it covers factors such as physical elements and site considerations, occupant considerations, protection systems and water supplies, hydrant locations, and special hazard considerations. Building characteristics including type of construction, materials used, occupancy, fuel load, roof and floor design, and unusual or distinguishing characteristics should be recorded, shared with other departments who provide mutual aid, and if possible, entered into the dispatchers computer so that the information is readily available if an incident is reported at the noted address. Since many fire departments have tens and hundreds of thousands of structures within their jurisdiction, making it impossible to pre-plan them all, priority should be given to those having elevated or unusual fire hazards and life safety considerations.
The fire department had conducted several pre-plan inspections of the structure involved in this incident. A building pre-plan form obtained from the fire department dated April 26, 2006 noted that store contents were household furniture and office equipment and that the rear warehouse contained racks approximately 30 feet high (see Appendix III). A more thorough building inspection and pre-incident plan for this single-story commercial building could have potentially identified the flat roof supported by lightweight metal bar joists (metal roof trusses), the immense fuel load considerations (i.e. large quantity of furniture and associated highly flammable furnishings in the showroom as well as stored in various locations throughout the facility), the presence of a drop ceiling and hydrant locations. Evaluating the size and construction features of the structure allows the fire department the opportunity to determine a response protocol for the specific identified hazards and to develop fireground strategies and tactics (hose line placement, water flow calculations, ventilation strategies, etc.) before an incident occurs. The hydrant location closest to the structure was noted on the April 2006 form (on the street to the rear of the warehouse), but was not used until the first mutual aid department set up operations at the rear of the warehouse. The construction features, occupancy (furniture retail), and fuel load present suggested large volumes of water would be necessary to fight a major fire at the site, which should have prompted the need to identify additional nearby hydrants. A more complete pre-planning process could have noted this information which may have aided the Incident Commander in developing a safer and more effective defensive strategy. Individual fire companies should be involved in pre-plan inspections outside their first-alarm territories so that they can become familiar with hazardous structures they may respond to on second and subsequent alarm assignments.
Recommendation #17: Fire departments should consider establishing and enforcing standardized resource deployment approaches and utilize dispatch entities to move resources to fill service gaps.
Discussion: On-scene commanders need to focus on the events occurring at the incident scene. Pre-planned resource deployment can be delegated to the dispatch system. Computer-aided dispatch can make this process automatic. Without a standardized deployment approach, on-scene commanders spend time making decisions that could have already been made. The movement of resources around the jurisdiction to fill coverage gaps should be delegated to others who do not have to focus their attention on the safety of the responders in the hazard zone, such as the dispatch center. According to retired Chief Alan Brunacini, “The IC must be highly familiar with dispatch / communications procedures and stay actively connected to the details of how that system works throughout operations. … The com center knows what resources are available, where they are, and directly controls the status keeping and dispatch system that can move and manage them. The IC must always use the IMS to get the right resources (closest to the incident / appropriate type) in the right place, doing the right things. … Having com work in concert with the IC many times makes a huge difference in the overall command and control.”41 For example, the dispatch center can advise the incident commander of time intervals since the initial dispatch (i.e. 10 minute or 15 minute intervals). Another example would be for dispatch to monitor fireground traffic or signs of problems, such as a Mayday call. The Incident Command System (ICS) Module Procedures Guide provides guidelines for managing major incidents and providing support to the IC by the establishment of a Planning Section to handle duties such as maintaining resource status and evaluating future resource requirements.42
In this incident, the fire departments procedure was for chief officers to call for additional resources as they deemed necessary. Delegating the tactical deployment and relocation of resources to dispatch or chief officers backfilling at other locations within the jurisdiction will allow Incident Commanders to focus on the fireground events. Using a standardized resource deployment approach, any Mayday should trigger the dispatcher to initiate additional measures in response to the emergency, such as notifying the Fire Chief and chief officers of the Mayday transmission and sending additional resources to the incident scene.
Recommendation #18: Fire departments should develop and coordinate pre-incident planning protocols with mutual aid departments.
Discussion: NFPA 1620 provides guidance to assist departments in establishing pre-incident plans. Pre-incident planning that includes agreements formed by a coalition of all involved parties including mutual aid fire departments, emergency medical services companies, and police, will present a coordinated response to emergency situations, and may save valuable time by a more rapid implementation of pre-determined protocols.40 Examples of such pre-incident planning for this incident include better coordination with the police department concerning traffic control and better utilization of the resources available from mutual aid departments, such as large diameter supply hoses.
Recommendation #19: Fire departments should ensure that any offensive attack is conducted using adequate fire streams based on characteristics of the structure and fuel load present.
Discussion: The objective of the offensive fire attack is to apply enough water directly to the burning fuel to achieve extinguishment.39 Determining the number and size of hose lines to deploy at a fire can be estimated by first estimating the size of the structure and applying various flowrate calculations such as what is taught at the U.S. National Fire Academy (area divided by 3) or by estimating the size of the fire. Retired Chief Alan Brunacini in his book Fire Command states Big Fire = Big Water, Little Fire = Little Water.27 In addition to the location and extent of the fire, factors affecting selection and placement of hose lines include the buildings occupancy, construction, and size. In addition, fire load and material involved, mobility requirements, and number of persons available to handle the hose lines are important factors. Regardless of the choice of attack method or the type of fire stream used, successful fire suppression depends upon discharging a sufficient quantity of water to remove the heat being generated, and ensuring that it reaches the fire rather than being turned into steam or being carried away by convective currents. A back-up line, at least as large as the initial attack line, should be in place and charged to protect the initial attack crew before interior fire fighting efforts begin.30 Some experts recommend that a 2 ½-inch-line attack hose lineroutinely be used with commercial and industrial structures if a sizable body of fire is present. The rational is that, compared to a residence, the fire load in commercial structures is usually heavier, will burn longer, and in need of harder hitting streams. In this incident, the loading dock area contained approximately 2,300 square feet of floor space, the right showroom addition contained approximately 7,000 square feet, and the main showroom contained approximately 17,000 square feet of floor space. Applying the National Fire Academy rule (area divided by 3), a minimum of 800 gallons per minute (gpm) of water would have been required at the loading dock. Crews operating at both the loading dock and the right showroom addition initially employed 1 ½ preconnected hand lines capable of flowing 90 gpm. 1-inch booster lines were also deployed. As the fire progressed, 2 ½ hand lines capable of flowing 350 gpm were put into operation, but their use was hindered by inadequate water supply so that the actual flow rates likely never approached these capacities during the incipient fire stage due to the small diameter of the supply lines. Table 1 provides examples of hose sizes and the corresponding flow rates.
| Hose Size | Flow Available |
|---|---|
| 2 ½ inch | 321 gallons per minute |
| (2) 2 ½ inch | 643 gallons per minute |
| 4 inch | 1, 017 gallons per minute |
| 5 inch | 1, 607 gallons per minute |
e Partial Table 13.15 courtesy of IFSTA Pumping Apparatus Driver/Operator Handbook (1999).43
Recommendation #20: Fire departments should ensure that an adequate water supply is established and maintained.
Discussion: Establishing adequate water supply on the fireground is an integral part of fire suppression. A supply hose is used to move large volumes of water between a pressurized water source and a pump that is supplying attack hose lines. It is also used to maintain a water system as a continuous conduit or by connecting water supply sources. Usually, the pressure in supply hose lines are lower than those used for the attack fire hose. According to Fire Hose Practices by IFSTA, the use of a 2 ½ inch hose was once considered the minimum diameter for a supply line, but is no longer recognized as an adequate supply hose. A 3 ½ supply line is now considered the minimum. In most instances, fire departments and industrial establishments have gone to a larger diameter supply line: 3 ½, 4, 4 ½, 5, 6, 8, 10 or 12 inches. In most cases, a short length of 5 or 6 diameter hose is used. With the ever-increasing demand for greater fire flow (water supply) over long distances, large diameter hoses (LDH) are used as above-ground water mains to allow for greater flow of water available for fire suppression, and to decrease friction loss due to a smaller diameter hose.44
The fire department involved in this incident routinely deployed 2 ½ hose as the main water supply line. In this incident, 23 50-foot sections of 2 ½ supply line were laid to a hydrant capable of supplying 1,256 gpm at 56 psi. Engine 16, stationed at the hydrant, pumped through the 23 sections of supply hose to supply Engine 11 located near the front entrance. Difficulties with the Engine 11 pump delayed the establishment of a constant water supply to the initial attack line (500 feet of 1 ½ hose line), causing the Engine 11 engineer to switch between tank water and the supply line. Crews also attempted to deploy a 1 booster line and a 2 ½ attack line (200 feet) from Engine 11. The deployment of a 1 ½ attack line over 250 feet increased the friction loss and lowered the water flow below safe and acceptable levels (150 gpm minimum). As the fire progressed and the need for additional water increased, chief officers radioed to the E-16 engineer to increase the water pressure. The officers ordered the E-16 engineer to go to 300 psi which was well over the maximum limit of 200 psi working pressure for the hose. It is likely that every time the 1" or the 2 ½" line nozzles were opened, the 1 ½" line pressure would drop. The 1 ½" line was the only one that was in position to effectively attack the fire at the rear of the showroom. To offset the reduced water flow (perceived as lack of water pressure at the nozzle), the engine operator was instructed to increase the pressure to pump more water, but this action would only increase the friction losses in the small diameter hose. A similar scenario developed on the D-side of the structure where Engine 12 was stationed at a hydrant pumping water through a single 2 ½ supply hose over 600 feet to Engine 10 which was pumping to multiple attack hoses. Additional supply hoses, increasing the volume of water available to both Engine 10 and Engine 11, were not added until after the fire fighters were determined to be missing. As the fire intensified and the need for additional water flow increased, the use of large diameter hoses for supply lines would have increased the water available at the pumps (E-10 and E-11).
Recommendation #21: Fire departments should consider using exit locators such as high intensity floodlights, flashing strobe lights, or hose markings, or safety ropes to guide lost or disoriented fire fighters to the exit.
Discussion: The use of high-intensity floodlights, flashing strobe lights, or other high visibility beacons can be set up at the entry portals of burning structures as an aid to assist fire fighters in situations requiring emergency escape.39 If staffing permits, a fire fighter can be stationed at the doorway to assist with flaking hose through the entrance and to assist exiting fire fighters. Hose lines can be marked with raised chevrons pointing in the direction of the pump (to the outside). Another option for locating exits is the deployment of safety rope lines as crews enter a structure. The end of the safety rope is secured outside the doorway and the rope is laid out as the crew advances inside. During this incident, several fire fighters inside the structure became disoriented as the conditions deteriorated. Most of the fire fighters working inside the structure ran out of air. During the NIOSH interviews, fire fighters stated they had to search for a hoseline to follow outside. Other fire fighters reported hearing the sound of Engine 11 running in the parking lot and then moving toward the sound. Safety ropes were not deployed by the initial crews who entered the structure.
Recommendation #22: Fire departments should ensure that Mayday transmissions are received and prioritized by the Incident Commander.
Discussion: The Incident Commander must monitor and prioritize every message, but only respond to those that are critical during a period of heavy communications on the fireground. A radio transmission reporting a trapped fire fighter is the highest priority transmission that Command can receive. Mayday transmissions must always be acknowledged and immediate action must be taken.45, 46 As soon as fire fighters become lost or disoriented, trapped or unsuccessful at finding their way out of the interior of a structural fire, they must initiate emergency radio transmissions. A Mayday call should receive the highest communications priority from dispatch, the IC, and all other units on-scene. In this incident, there were multiple radio transmissions of fire fighters asking for assistance in finding the exit. There was no reaction to these radio transmissions for several minutes, possibly due to the large volume of radio traffic and/or the chief officers being distracted by engaging in fireground activities. The sooner the IC is notified and a RIT is activated, the greater the chance of the fire fighter(s) being rescued.
Recommendation # 23: Fire departments should train fire fighters on actions to take if they become trapped or disoriented inside a burning structure.
Discussion: Fire fighters must act promptly when they become lost, disoriented, injured, low on air, or trapped.45-50 First, they must transmit a distress signal while they still have the capability and sufficient air, noting their location if possible. The next step is to manually activate their PASS device. To conserve air while waiting to be rescued, fire fighters should try to stay calm, be focused on their situation and avoid unnecessary physical activity. They should survey their surroundings to get their bearings and determine potential escape routes such as windows, doors, hallways, changes in flooring surfaces, etc.; and stay in radio contact with the IC and other rescuers. Additionally, fire fighters can attract attention by maximizing the sound of their PASS device (e.g. by pointing it in an open direction); pointing their flashlight toward the ceiling or moving it around; and using a tool to make tapping noises on the floor or wall. A crew member who initiates a Mayday call for another person should quickly try to communicate with the missing member via radio and, if unsuccessful, initiate another Mayday providing relevant information on the missing fire fighters last known location.
In this incident, fire fighters radioed that they had lost contact with the hose, needed assistance getting out, and at least one fire fighter radioed Mayday then activated the emergency button on his radio. None of these radio transmissions gave any information regarding the fire fighters locations i.e. rear of the main showroom, near the loading dock, etc. At least one fire fighter entered the structure without a radio.
Recommendation #24: Fire departments should ensure that all fire fighters and line officers receive fundamental and annual refresher training according to NFPA 1001 and NFPA 1021.
Discussion: Initial and continual training provides an opportunity to ensure that all fire fighters and line officers are proficient in their knowledge and skills in recognizing and mitigating hazards. Training on structural fire fighting should include, but not be limited to, departmental standard operating procedures, fire fighter safety, building construction, and fireground tactics. NFPA 1500, Chapter 5, requires that the fire department provide an annual skills check to verify minimum professional qualifications of its members.18 NFPA 1001 Standard for Fire Fighter Professional Qualifications was established to facilitate the development of nationally applicable performance standards for uniformed fire service personnel.6 NFPA 1021 Standard for Fire Officer Professional Qualifications was developed in the same way to determine that an individual possesses the skills and knowledge to perform as a fire officer.23 The intent of both of these standards is to develop clear and concise job performance requirements (JPRs) that can be used to determine that an individual, when measured to the standard, possesses the skills and knowledge to perform as a fire fighter or a fire officer, and that these JPRs can be used by any fire department in the country.
Training is an ongoing process, whether held daily, weekly or monthly, it allows members to maintain proficiency at their present levels, meet certification requirements, learn new procedures, and keep up with emerging technology. This fire department required fire fighters to receive basic fire fighter training certification before being considered for employment. Once recruits were hired they were put through a ten day hands-on training and then assigned to their station. This ten day training included equipment use, SCBA use, ladder drills, hydrant hookup, hose lays, hose pulls, rescue drills, and live-burn exercises. The training provided for basic hose line operations was minimal. Hands-on training should also include topics such as hazard recognition, ventilation tactics, ICS/NIMS, scene size-up, and basic hose line operations. The basic training certification required by the fire department at the time of this incident did not meet NFPA Fire Fighter I requirements.
Recommendation #25: Fire departments should implement joint training on response protocols with mutual aid departments.
Discussion: Mutual aid companies should train together and not wait until an incident occurs to attempt to integrate the participating departments into a functional team. Differences in equipment and procedures need to be identified and resolved before an emergency occurs when lives may be at stake. Procedures and protocols that are jointly developed, and have the support of the majority of participating departments, will greatly enhance overall safety and efficiency on the fireground. Once methods and procedures are agreed upon, training protocols must be developed and joint-training sessions conducted to relay appropriate information to all affected department members.
Fire departments should develop and establish good working relationships with surrounding departments so that reciprocal assistance and mutual aid is readily available when emergency situations escalate beyond response capabilities. During this incident, there was little coordination and communication between the municipal and the mutual aid departments, although fire fighters from the mutual aid department played key roles in rescuing the trapped employee, attempting to search the main showroom for missing fire fighters, and establishing water supply. Coordination of fireground efforts could have been enhanced if protocol planning, communication procedures (such as radio frequency/channel selection), and prior training had taken place among mutual aid departments.
Recommendation #26: Fire departments should ensure apparatus operators are properly trained and familiar with their apparatus
Discussion: Modern fire apparatus are complex equipment. Fire fighters require considerable knowledge, skills and abilities in order to properly and safely operate fire apparatus. NFPA 1002 Standard for Fire Apparatus Driver/Operator Professional Qualifications, Chapter 5 lists the requisite knowledge and skills necessary to safely operate fire apparatus equipped with fire pumps.51 Prior to this incident, the fire department provided driver / operator training that consisted mainly of on-the-job training. Individual fire fighters could request to be trained as a driver / operator and this request would be approved through the fire department chain-of-command. Fire fighters then received hands-on training during normal work hours. During this incident, an operator who was not experienced with one of the engines encountered trouble getting the pump to go into gear for pump operations. A detailed inspection report provided by the city (see Appendix II) demonstrates that specialized training and experience was needed to properly engage the pump.
Recommendation #27: Fire departments should protect stretched hose lines from vehicular traffic and work with law enforcement or other appropriate agencies to provide traffic control.
Discussion: In urban settings, fire hose is commonly used on the fireground to transfer water from the distribution system (usually from a hydrant) to the fire apparatus supplying water to the attack lines. Fire hose is often stretched across roadways and through parking lots. Fire hose may be damaged in a variety of ways while being used on the fireground. Fire departments should avoid laying or pulling hose over rough terrain, sharp edges or objects. A damaged hose may impede fire suppression activities or put fire fighters in an unsafe position by reducing the water needed for fire suppression while attacking the fire. Fire departments should provide protection for deployed hose lines that may potentially be run over by vehicular traffic or be damaged by vibration. This can be done by the use of chafing blocks, hose ramps, or hose bridges.19 Many commercial versions are available or these items can be custom made. Fire departments should also position someone at these protective devices so vehicular traffic can be properly guided across or re-routed, and to make sure the hose does not move around. Fire departments should work with the local police and law enforcement agencies to ensure adequate traffic control, warning barricades, and traffic re-direction takes place. During this incident, fire apparatus engineers radioed dispatch multiple times requesting public safety assistance for traffic control because civilian vehicle traffic was running over the 2 ½ supply lines, disrupting the water supply. During the incipient stage of the fire, traffic was not being redirected and protective devices were not in use (see Photo 11).
Recommendation #28: Fire departments should ensure that fire fighters wear a full array of turnout clothing and personal protective equipment appropriate for the assigned task while participating in fire suppression and overhaul activities.
Discussion: NFPA 1500 Standard on Fire Department Occupational Safety and Health Program, Chapter 7 contains the general recommendations for fire fighter protective clothing and protective equipment.18 Chapter 7.1.1 specifies that the fire department shall provide each member with protective clothing and protective equipment that is designed to provide protection from the hazards to which the member is likely to be exposed and is suitable for the tasks that the member is expected to perform. Chapter 7.1.2 states protective clothing and protective equipment shall be used whenever the member is exposed or potentially exposed to the hazards for which it is provided. Chapter 7.1.3 states structural fire-fighting protective clothing shall be cleaned at least every 6 months as specified in NFPA 1851 Standard on Selection, Care, and Maintenance of Structural Fire Fighting Protective Ensembles. 52 Chapter 7.2.1 states members who engage in or are exposed to the hazards of structural fire fighting shall be provided with and shall use a protective ensemble that shall meet the applicable requirements of NFPA 1971 Standard on Protective Ensembles for Structural Fire Fighting and Proximity Fire Fighting. 53 Chapter 7.9.7 states when engaged in any operation where they could encounter atmospheres that are immediately-dangerous-to-life-or-health (IDLH) or potentially IDLH, or where the atmosphere is unknown, the fire department shall provide and require all members to use SCBA that has been certified as being compliant with NFPA 1981 Standard on Open-Circuit Self-Contained Breathing Apparatus for Fire and Emergency Services. 54 Additionally, the OSHA Respirator Standard requires that all employees engaged in interior structural fire fighting use SCBAs.8 During this incident, there were multiple instances where fire fighters were observed working in close proximity to the burning structure with incomplete personal protective ensembles including incomplete turnouts (i.e. no turnout pants, turnout coats unfastened, suspenders improperly worn, no gloves, no hoods), entering the burning structure without an SCBA, and off-duty fire fighters actively working in street clothing with no personal protection at all. The evaluation report of the PPE worn by the nine victims identified instances where the PPE was not properly worn such as turnout coat collars not fully extended upward and helmet ear flaps not deployed (see Appendix IV).
It is important to note that the 2007 revision to NFPA 1982 Standard on Personal Alert Safety Systems (PASS) includes new heat and flame resistance requirements resulting from documented reports where PASS devices were not heard during fatal fireground incidents.55 Laboratory testing conducted by NIST determined that exposure to high temperature environments caused the loudness of the tested PASS alarm signal to be reduced. This reduction in loudness can cause the alarm signal to become indistinguishable from background noise at an emergency scene. Initial laboratory testing by NIST highlighted that this sound reduction may begin to occur at temperatures as low as 300°F. Thus the use of PASS devices meeting NFPA 1982, 2007 Edition requirements is highly recommended.
Recommendation #29: Fire departments should ensure that fire fighters are trained in air management techniques to ensure they receive the maximum benefit from their self-contained breathing apparatus (SCBA).
Discussion: SCBA air cylinders contain a finite volume of air, regardless of the size. Air consumption will vary with each individuals physical condition, the level of training, the task performed, and the environment. Depending on the individuals air consumption and the amount of time required to exit an immediately-dangerous-to-life-and-health (IDLH) environment, the low air alarm may not provide adequate time to exit. Working in large structures (high rise buildings, warehouses, and supermarkets) requires that fire fighters be cognizant of the distance traveled and the time required to reach the point of suppression activity from the point of entry. When conditions deteriorate and the visibility becomes limited, fire fighters may find that it takes additional time to exit when compared to the time it took to enter the structure.46, 56 NFPA 1404 Standard for Fire Service Respiratory Protection Training Paragraph 5.1.4.2 requires fire departments to train fire fighters on air management techniques so that the individual fire fighter will develop the ability to manage his or her air consumption while wearing an SCBA. NFPA 1404 specifies that the individual air management program should include the following directives:
- Exit from an IDLH atmosphere should be before consumption of reserve air supply begins.
- Low air alarm is notification that the individual is consuming the reserve air supply.
- Activation of the reserve air alarm is an immediate action item for the individual and the team.57
Fire departments and fire fighters should regularly conduct training exercises in which fire fighters perform various exercises and work tasks at different work rates until their SCBA cylinder air is exhausted so that fire fighters become familiar with the time they can expect to work before the low air alarm sounds, and how long they have to exit once the low air alarm sounds. In order to comply with NFPA 1404, fire departments and fire fighters should follow the Rule of Air Management which states Know how much air you have in your SCBA and manage that air so that you leave the hazardous environment before your low-air alarm activiates.57, 58 By being aware of these time parameters, fire fighters can make educated decisions on the time they can safely spend in IDLH atmospheres. In this incident, the majority of fire fighters who entered the main showroom ran out of air. Some of the fire fighters were able to exit. The nine victims are all believed to have run out of air.
Recommendation #30: Fire departments should develop, implement and enforce written SOPs to ensure that SCBA cylinders are fully charged and ready for use.
Discussion: During this incident, many of the fire fighters who entered the main showroom became disoriented due to the rapidly deteriorating conditions and ran low or completely exhausted their air supply. The examination of the remains of the SCBA used by the 9 victims suggested that all 9 SCBA were out of air. The SCBA used by this fire department include cylinders that are rated for a 30-minute duration when fully charged to 2216 psi. During the NIOSH interview process, several fire fighters stated that the fire departments procedures were to refill cylinders when the pressure dropped to 1500 psi which is well below the required 90% level (1500 psi is 68% of full cylinder pressure). Although NIOSH did not examine all department SCBAs or a scientific sample of SCBAs, examination of a small convenience sample of in-service SCBAs did identify some below 2000 psi. Cylinders designed to be fully charged at 2,216 psi should be refilled whenever the pressure falls to 1,994 psi. Due to gauge accuracy and the type of scale used on the face of the cylinder pressure gauge, any cylinder at or below 2000 psi should be topped off to ensure fire fighters are entering IDLH conditions with a full cylinder. The OSHA Respirator Standard, 29 CFR 1910.134(h)(3)(iii) states Air and oxygen cylinders shall be maintained in a fully charged state and shall be recharged when the pressure falls to 90% of the manufacturer's recommended pressure level.8 NFPA 1852 and good SCBA practice dictate that SCBA air cylinders be refilled whenever the cylinder pressure falls to 90% of the manufacturers recommended pressure level.9, 59 A 30-minute cylinder typically holds 1,200 liters of air when fully charged. A cylinder charged to 1,500 psi would hold approximately 812 liters of air. A fire fighter working at a moderate work rate (40 liter per minute air consumption rate) would exhaust a cylinder holding 1500 psi in approximately 20 minutes (812 liters divided by 40 liters per minute). Fire fighters working at a higher work rate or breathing under duress (such as in an emergency situation) would exhaust a cylinder much quicker. During extreme exertion, the actual service time can be reduced by 50 percent or more. 9 A number of fire fighters inside the showroom were running low on air within 20-25 minutes.
Recommendation #31: Fire departments should use thermal imaging cameras (TICs) during the initial size-up and search phases of a fire.
Discussion: Thermal imaging cameras (TIC) can be a useful tool for initial size up and for locating the seat of a fire. Infrared thermal cameras can assist fire fighters in quickly getting crucial information about the location of the source (seat) of the fire from the exterior of the structure which can help plan an effective and rapid response. Knowing the location of the most dangerous and hottest part of the fire may help fire fighters determine a safer approach and avoid exposure to structural damage in a building that might have otherwise been undetectable. Ceilings and floors that have become dangerously weakened by fire damage and are threatening to collapse may be spotted with a thermal imaging camera. A fire fighter about to enter a room filled with flames and smoke can use a TIC to assist in judging whether or not it will be safe from falling beams, walls, or other dangers. The use of a thermal imaging camera may provide additional information the Incident Commander can use during the initial size-up. Thermal imaging cameras (TICs) should be used in a timely manner, and fire fighters should be properly trained in their use and be aware of their limitations.60
The use of a TIC during initial size-up and entry into the structure might have confirmed the presence of hot smoke and gases in the concealed space above the suspended ceiling, which would have been an indicator that more defensive tactics should be considered. TICs were available on the fireground but never put into service.
Recommendation #32: Fire departments should develop, implement and enforce written SOPs and provide fire fighters with training on the hazards of truss construction
Discussion: Fire departments should develop, implement and enforce SOPs or SOGs concerning safe fireground tactics when operating in structures containing truss construction and then train fire fighters to recognize the hazards of lightweight truss construction and the appropriate actions to take.61,62 Fire departments should use pre-incident planning and building inspections to identify structures within their jurisdiction that contain truss construction. Pre-plan information should be entered into the dispatcher's computer so that when a fire is reported at pre-planned locations, the dispatcher can notify by radio all first responders with critical information.61, 62 Fire departments should ensure that the Incident Commander conducts an initial size-up and risk assessment of the incident scene before beginning interior fire-fighting operations. Hidden voids within truss construction provide large areas for smoke and hot gases to accumulate unseen. These hidden voids provide the potential for rapid fire spread, which may go unnoticed by fire fighters working below. The Rapid Intervention Team should be immediately notified when truss construction is identified. Fire departments should use defensive strategies whenever trusses have been exposed to fire or structural integrity cannot be verified. Unless life-saving operations are under way, fire fighters should immediately be evacuated and an exterior attack should be used.61, 62 Fire fighters performing fire-fighting operations under or above trusses should be evacuated as soon as it is determined that the trusses are exposed to fire (not according to a time limit). A collapse zone should be established when operating outside a burning building, since truss roof collapses can push out on the walls, causing a secondary collapse of the exterior walls. The collapse zone should be equal to the height of the building plus allowance for scattering debris, usually at least 1½ times the height of the building.39, 61, 63 Defensive overhauling procedures should be used after fire extinguishment in a building containing truss construction. Outside master streams should be used to soak the smoldering truss building and prevent rekindling.39, 61, 63
Recommendation #33: Fire departments should establish a system to facilitate the reporting of unsafe conditions or code violations to the appropriate authorities.
Discussion: In 1987 the responsibility for fire code inspections was transferred from the fire department to the city. In order to facilitate open communication, fire department personnel and building code officials should be cross-trained on each-others duties and responsibilities. Fire fighters should have a basic understanding of what a code violation is and building code inspectors should have a basic understanding of fire fighter safety issues. The fire department conducted a number of pre-plan inspections at the structure involved in this incident. However, unsafe conditions and code violations were not noted on the pre-plan inspection form presented to NIOSH. The pre-plan form did note the presence of the warehouse with storage shelves approximately 30 feet high, but did not note the light weight metal roof trusses and the excessive fuel loads associated with the contents. Such information could be used to facilitate safer conditions for employees, the public and fire fighters and emergency responders called to the scene. The accumulation of trash outside the loading dock, large quantities of flammable liquids, solvents, and thinners in the loading dock area and storage of furniture and flammable materials in non-permitted areas were determined to be code violations after the incident. The identification and reporting of these conditions to the responsible authorities prior to the incident could potentially have resulted in corrective actions.
Recommendation #34: Fire departments should ensure that fire fighters and emergency responders are provided with effective incident rehabilitation
Discussion: Effective emergency incident rehabilitation is an important element of fire fighter health and safety. Quoting Gregory Cade, former U.S. Fire Administrator, Emergency responder rehabilitation is designed to ensure that the physical and mental well-being of members operating at the scene of an emergency do not deteriorate to the point where it effects their safety. It can prevent serious and life-threatening conditions such as heat stroke and heart attacks from occurring. Fireground rehab is the term often used for the care given to fire fighters and other responders while performing their duties at an emergency scene. Fireground rehab includes monitoring vital signs, rehydration, nourishment, and rest for responders between assignments.64, 65 During this incident, the municipal fire department did not practice fireground rehab.
Recommendation #35: Fire departments should provide fire fighters with station / work uniforms (e.g., pants and shirts) that are compliant with NFPA 1975 and ensure the use and proper care of these garments.
Discussion: Fire fighters involved in structural fire fighting and other emergency activities should be provided, at a minimum, station / work uniforms that are certified and compliant with NFPA 1975 in order to avoid the potential for burn injuries that are more severe as the result of using thermally unstable or rapidly deteriorating materials (e.g., fabrics that contain a significant portion of polyester or other synthetic fabrics that easily melt at low temperatures). Ideally, the prescribed station / work uniforms should also be flame resistant certified to the optional requirements specified in NFPA 1975.7 The use of NFPA 1975-compliant station / work uniforms is specified in NFPA 1500 (paragraphs 7.1.5 and 7.1.6), which also recommends that departments provide for the adequate cleaning of station / work uniforms provided to their members (7.1.7).18 According to Appendix A.5.3.10 of NFPA 1500, clothing that is made from 100 percent natural fibers or blends that are principally natural fibers should be selected over other fabrics that have poor thermal stability or ignite easily. Appendix A.5.3.10 further states The very fact that persons are fire fighters indicates that all clothing that they wear should be flame resistant (as children's sleepwear is required to be) to give a degree of safety if unanticipated happenings occur that expose the clothing to flame, flash, sparks, or hot substances. This would include clothing worn under their structural fire-fighting protective ensemble. While compliance with NFPA standards is voluntary, in many instances NFPA standards represent fire service best practices available for ensuring fire fighter safety and health, especially where state and federal laws are silent on health and safety issues.
In this incident, the fire fighters were not supplied with nor were they wearing station/work uniforms that were compliant with NFPA 1975. Although the use of polyester work clothing was not a direct contributing factor to the nine fatalities that occurred in this incident, the wearing of polyester-based uniforms can contribute to significant potential for severe burn injury.
Recommendation #36: Federal and state occupational safety and health administrations should consider developing additional regulations to improve the safety of fire fighters, including adopting National Fire Protection Association (NFPA) consensus standards.
Discussion: Fire fighters have a high rate of injury death compared to other occupations,11 yet federal and state regulations addressing the risks of fire fighting are sparse. In September 2007, the federal Occupational Safety and Health Administration (OSHA) requested information from the public to evaluate what action, if any, the US Department of Labor should take to further address emergency response and preparedness, including the safety of fire fighters during common responses such as structural fires, as well as rare and unexpected events, such as natural disasters and terrorist attacks.66 In this request for information, OSHA noted that elements of emergency responder health and safety are currently regulated by a number of standards, many of which were promulgated decades ago, and none designed as a comprehensive emergency response standard. Consequently, existing standards do not address the full range of hazards or concerns currently facing emergency responders, including fire fighters.
NIOSH provided comments in response to this request.67 NIOSH expressed support for this information gathering process, and provided data, information, and recommendations from NIOSH fire fighter fatality investigations and research. NIOSH suggested that OSHA consider regulating all types of emergency incidents, both common and rare events, and that OSHA consider the full continuum of emergency response activities, from pre-planning for emergency response activities through recovery and post-incident treatment. NIOSH provided information from fire fighter fatality investigations, including large numbers of investigations in which NIOSH recommended that fire departments: comply with NFPA standards for personal protective clothing and equipment,52, 53 require the use of Personal Alert Safety Systems,55 require minimum standards for safety and health training, require the use of an Incident Management System to manage emergency events,21 require a designated Safety Officer at emergency events, require the use of thermal imaging cameras at structure fires, require that fire departments have written SOPS and a written safety and health program, and require that RIT teams be established at emergency events before fire fighters enter IDLH environments. NIOSH referenced several NFPA standards in these comments.
Compliance with existing federal and state occupational safety and health regulations may not be adequately protecting fire fighters, and is inconsistent with industry best practices developed through the NFPA consensus process. In addition to OSHA considering additional regulations to protect fire fighters, state occupational safety and health agencies that cover public employees should similarly consider enhancing the protection of fire fighters through their state regulations.
Recommendation #37: Manufacturers, equipment designers, and researchers should continue to develop and refine durable, easy-to-use radio systems to enhance verbal and radio communication in conjunction with properly worn SCBA.
Discussion: The use of Personal Protective Equipment (PPE) and an SCBA make it difficult to communicate, with or without a radio.68,69 Faced with the difficult task of communicating while wearing a SCBA, fire fighters sometimes momentarily remove their face pieces to transmit a message directly or over a portable radio. Considering the toxic and oxygen-deficient hazards posed by a fire and the resulting products of combustion, removing the SCBA face piece, even briefly, is a dangerous practice that should be prohibited. Even small exposures to carbon monoxide and other toxic agents present during a fire can affect judgment and decision making abilities. To facilitate communication, equipment manufacturers have designed face piece-integrated microphones, intercom systems, throat mikes and bone mikes worn in the ear or on the forehead.69, 70
Recent testing of portable radios in simulated fire fighting environments by the National Institute for Standards and Technology (NIST) has identified that radios are vulnerable to exposures to elevated temperatures. Some degradation of radio performance was measured at elevated temperatures ranging from 100OC to 260OC, with the radios returning to normal function after cooling down. Additional research is needed in this area.71
During this incident fire fighters experienced intermittent radio communication problems and interruptions. Audio transcripts of the fireground channel recorded multiple instances where fire fighters inside the structure (including some of the victims) transmitted over the radio, but the transmissions were not heard or could not be understood. Effective radio communication is an important part of safe fireground operations.
Recommendation #38: Manufacturers, equipment designers and researchers should conduct research into refining existing and developing new technology to track the movement of fire fighters inside structures.
Discussion: Fire fighter fatalities often are the result of fire fighters becoming lost or disoriented on the fireground. The use of systems for locating lost or disoriented fire fighters could be instrumental in reducing the number of fire fighter deaths on the fireground. The National Institute for Standards and Technology (NIST) has been evaluating the feasibility of real-time fire fighter tracking and locator systems.68, 72 Research into refining existing systems and developing new technologies for tracking the movement of fire fighters on the fireground should continue.
Recommendation #39: Code setting organizations and municipalities should require the use of sprinkler systems in commercial structures, especially ones having high fuel loads and other unique life-safety hazards, and establish retroactive requirements for the installation of fire sprinkler systems when additions to commercial buildings increase the fire and life safety hazards
Discussion: This recommendation focuses on fire prevention and minimizing the impact of a fire if one does start. The NFPA Fire Protection Handbook states throughout history there have been building regulations for preventing fire and restricting its spread. Over the years these regulations have evolved into the codes and standards developed by committees concerned with fire protection. The requirements contained in building codes are generally based upon the known properties of materials, the hazards presented by various occupancies, and the lessons learned from previous experiences, such as fire and natural disasters.73 Although municipalities have adopted specific codes and standards for the design and construction of buildings, structures erected prior to the enactment of these building laws may not be compliant. Such new and improved codes can improve the safety of existing structures.73 Sprinkler systems are one example of a safety feature that can be retrofitted into older structures. Sprinkler systems can reduce fire fighter fatalities since such systems can contain and may even extinguish fires prior to the arrival of the fire department. In this incident, this structure incorporated mixed-used construction types and was non-sprinklered. The original structure was built in the 1960s (17,500 square feet), with additions added in 1994 (6,970 square feet) and 1995 (7,020 square feet). The structure was annexed into the city in 1990. City ordinances required commercial structures over 15,000 square feet to have a sprinkler system. The original structure was grandfathered, and the subsequent additions were treated as separate buildings so the facility was never sprinklered. The additions were treated as separate structures with the end result being that each addition did not meet the threshold at which a sprinkler system would be required.
Recommendation #40: Code setting organizations and municipalities should require the use of automatic ventilation systems in commercial structures, especially ones having high fuel loads and other unique life-safety hazards.
Discussion: The use of automatic ventilation systems in roofs and enclosed void spaces that would open in the event of a fire and allow smoke, hot fire gases and heat to escape could aid fire fighters by helping control fire spread. Smoke venting through these openings would also give Incident Commanders and fire fighters very useful information related to the fires size, location and stage of growth. Many European standards such as the UK legislation requirements of BS7346 part 1 (European National (EN) 12101) & BS 5588 part 5 require automatic roof ventilation systems that automatically open to ensure rapid dispersal of smoke, heat and toxic gases.74
Recommendation #41: Municipalities and local authorities having jurisdiction should coordinate the collection of building information and the sharing of information between building authorities and fire departments.
Discussion: Municipalities and local authorities having jurisdiction should develop a questionnaire or checklist to ensure that pre-plan inspections collect the appropriate information. The questionnaire or checklist could focus on building characteristics including the type of construction, materials used, occupancy, fuel load, roof and floor design, and unusual or distinguishing characteristics. Once obtained, this information should be recorded, shared with all departments who provide mutual aid, and if possible, entered into the dispatchers computer so that the information is readily available if an incident is reported at the noted address. Municipalities and local authorities having jurisdiction should also include experienced fire personnel throughout any zoning or building code developmental process concerning life safety to the public and fire department members. Typically, pre-incident planning focuses on commercial buildings and the specific hazards they have due to their size, construction, and contents.
Recommendation #42: Municipalities and local authorities having jurisdiction should consider establishing one central dispatch center to coordinate and communicate activities involving units from multiple jurisdictions.
Discussion: An effective radio communication system is a key factor in fire department operations. The communication system, or central dispatch center, is used for receiving notification of emergencies, alerting personnel and fire apparatus, coordinating the activities of the units engaged in emergency incidents, and providing non-emergency communications for the coordinating fire departments. The dispatch system must be able to identify the type and number of units due to respond to the type of incident in advance based on risk criteria and unit capabilities. The central dispatch center should also monitor fireground activity and inform command of time intervals or of possible missed transmissions such as Maydays. A central dispatch center equipped with regional mutual aid channels could serve multiple jurisdictions.38, 70 This type of system would provide operational advantages in the communication system, reflect a more functional mutual aid system, and reduce overall costs of operating centers in individual jurisdictions. Having a pre-determined response for apparatus arranged by district, address or by type of incident, makes the job of the Incident Commander and the dispatcher much easier. The pre-determined assignment lists the apparatus slated to respond to the incident and should take into account apparatus that are out of service by filling in for such units with similar units. In this incident, the municipal fire department maintained its own dispatch center in cooperation with the city policy department. The neighboring departments either had their own dispatch centers or were serviced by the county dispatch system. The municipal fire department relied upon the chief officers to request companies as the need was identified, instead of having predetermined response assignments.
Recommendation #43: Municipalities and local authorities having jurisdiction should ensure that fire departments responding to mutual aid incidents are equipped with mobile and portable communications equipment that are capable of handling the volume of radio traffic and allow communications among all responding companies within their jurisdiction.
Discussion: Units responding to or engaged at incidents should have the necessary radio frequencies/channels to be in contact with other units providing mutual aid. These units should also have the capability to monitor the fireground activities while en-route. 38 During this incident, some mutual aid departments could not communicate with the IC or the municipal dispatch center on either their portable or mobile radios.
REFERENCES
- Routely JG, Chiaramonte M, Crawford B, Piringer P, Roche K, Sendelbach T [2007]. City of Charleston Post Incident Assessment and Review Team: Phase 1 Report. October 16, 2007.
- Routely JG, Chiaramonte M, Crawford B, Piringer P, Roche K, Sendelbach T [2008]. City of Charleston Post Incident Assessment and Review Team: Phase II Report. May 15, 2008.
- South Carolina Department of Labor, Licensing and Regulation [2009]. S. C. Occupational Safety and Health Administration (OSHA) http://www.llr.state.sc.us/ Date accessed: February 5, 2009. (Link Updated 1/8/2013)
- South Carolina Department of Labor, Licensing and Regulation [2007]. Report of S.C. OSHA findings in June 18, 2007 Charleston Super Sofa Fire. Columbia, SC: Department of Labor, Licensing and Regulation. http://media.charleston.net/pdf/OSHAreport.pdf Date accessed: February 5, 2009. (Link no longer available 4/9/2013)
- State of South Carolina [2007]. Settlement Agreement. Columbia, SC: State of South Carolina, County of Richland. http://media.charleston.net/2007/pdf/settlement_agreement_120307.pdf Date accessed: February 5, 2009. (Link no longer available 4/9/2013)
- NFPA [2008]. NFPA 1001: Standard for Firefighter Professional Qualifications. 2008 ed. Quincy, MA: National Fire Protection Association.
- NFPA [2004]. NFPA 1975 Standard on station / work uniforms for fire and emergency services. Quincy, MA: National Fire Protection Association.
- OSHA [1998]. 29 CFR Parts 1910 and 1926 Respiratory Protection; Final Rule. Federal Register Notice 1218-AA05. Vol. 63, No. 5. January 8, 1998. U.S. Department of Labor, Occupational Safety and Health Administration. Washington DC.
- NFPA [2008]. NFPA 1852 Standard on Selection, Care, and Maintenance of Open-Circuit Self-Contained Breathing Apparatus (SCBA). Quincy, MA: National Fire Protection Association.
- Weather Underground [2008]. Weather history for incident location in SC, June 18, 2007. http://www.wunderground.com/history/airport/KCHS/2007/6/18/DailyHistory.html?req_city=Charleston&req_state=SC&req_statename=South+Carolina (Link updated 4/2/2009) Date accessed: October 29, 2008.
- Clarke C, Zak MJ [1999]. Fatalities to law enforcement officers and firefighters, 1992-1997. Compensation and Working Conditions, 1999.
- Arocena P, Nunez I, Villanueva M [2008]. The impact of prevention measures and organizational factors on occupational injuries. Safety Science 46: 1369-1384.
- Aksom T, Hadikusumo [2008]. Critical success factors influencing safety program performance in Thai construction projects. Safety Science 46: 709-727.
- Mearns K, Whitaker SM, Flin R [2003]. Safety climate, safety management practice and safety performance in offshore environments. Safety Science 41: 641-680.
- Shannon HS, Robson LS, Sale JM [2001]. Creating safer and healthier workplaces: role of organizational factors and injury rates. American Journal of Industrial Medicine 40: 319-334.
- Vredenburgh A [2002]. Organizational safety: which management practices are most effective in reducing employee injury rates? J Safety Research 33: 259-276.
- Shannon HS, Mayr J, Haines T [1997]. Overview of the relationship between organizational and workplace factors and injury rates. Safety Science 26: 201-217.
- NFPA [2007]. NFPA 1500: Standard on Fire Department Occupational Safety and Health Program. Quincy, MA: National Fire Protection Association
- IFSTA [2008]. Essentials of fire fighting, 5th ed. Oklahoma State University. Stillwater, OK: Fire Protection Publications, International Fire Service Training Association.
- Dodson D [2007]. Fire Department Incident Safety Officer. 2nd Edition. New York: Thomson Delmar Learning.
- NFPA [2008]. NFPA 1561 Standard on Emergency Services Incident Management System, 2008 Edition. Quincy, MA: National Fire Protection Association.
- OSHA [1996]. The National Response Team's Integrated Contingency Plan Guidance; Federal Register Notice 61:28641-28664, June 5, 1996. Posted as a guidance document on the Occupational Health and Safety Administration website https://www.osha.gov/pls/oshaweb/owadisp.show_document?p_table=FEDERAL_REGISTER&p_id=13550. Date accessed: October 29, 2008.
- NFPA [2008]. NFPA 1021: Standard for Fire Officer Professional Qualifications. 2003 ed. Quincy, MA: National Fire Protection Association.
- NFPA [2008]. NFPA 1521. Standard for Fire Department Safety Officer. 2008 Edition. Quincy, MA: National Fire Protection Association.
- Dunn V [1992]. Safety and Survival on the Fireground. Saddle Brook NJ: Fire Engineering Books and Videos.
- Dunn V [2000]. Command and Control of Fires and Emergencies. Saddle Brook NJ: Fire Engineering Book and Videos.
- Brunacini AV [1985]. Fire command. Quincy, MA: National Fire Protection Association.
- Dunn V [1998]. Risk management and lightweight truss construction. New York: WNYF, Official training publication of the New York City Fire Department, 1st issue.
- NIOSH [1999]. NIOSH Alert: Request for assistance in preventing injuries and deaths of fire fighters due to structural collapse. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health. (NIOSH) Publication No. 99-146.
- Dunn, V. [2007]. Strategy of Firefighting. Saddlebrook NJ: Penn Well Publishing Co. p- 162.
- Dunn, V. [1988]. Collapse of Burning Buildings: A Guide to Fireground Safety. Saddle Brook, NJ: Fire Engineering Books and Videos.
- International Fire Service Training Association (IFSTA) [2000]. Model Procedures Guide for Structural Firefighting. 2nd Edition. Stillwater, OK: Fire Protection Publications.
- NIOSH [2005]. Career fire fighter dies and two career captains are injured while fighting night club arson fire Texas. Morgantown, WV: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, Fatality Assessment and Control Evaluation (FACE) Report F200414, p. 6.
- International Fire Service Training Association (IFSTA)[2002]. Fireground support operations. 4th Edition. Stillwater, OK: Fire Protection Publications.
- Kipp JD and Loflin ME [1996]. Emergency incident risk management. New York, NY: Van Nostrand Reinhold, p. 253.
- Foley S. [1998]. NFPA 1500, Fire department occupational health and safety standards handbook. 1st ed. Quincy, MA: National Fire Protection Association (chapter 3).
- Dodson, D [2005]. The art of first-due. Fire Engineering. March 2005, pp. 135-141.
- NFPA [2004]. NFPA 1710 Standard for the Organization and Deployment of Fire Suppression Operations, Emergency Medical Operations, and Special Operations to the Public by Career Fire Departments. 2004 Edition. Quincy, MA: National Fire Protection Association.
- Klaene BJ and Sanders RE [2000]. Structural fire fighting. Quincy, MA: National Fire Protection Association.
- NFPA [2003]. NFPA 1620: Recommended practice for pre-incident planning. Quincy, MA: National Fire Protection Association.
- Brunacini A, Brunacini N [2004]. Command Safety: The ICs role in protecting firefighters. Peoria, AZ: Across the Street Productions, Inc.
- National Incident Management System Consortium [2007]. Incident Command System (ICS) Model Procedures Guide for Incidents Involving Structure Fire Fighting, High-Rise, Multi-Casualty, Highway, and Managing Large-Scale Incidents Using NIMS-ICS. First Edition. Oklahoma State University. Fire Protection Publications.
- IFSTA [1999]. Pumping Apparatus Driver/Operator Handbook. 1st ed. Fire Protection Publications. International Fire Service Training Association.
- IFSTA [2004]. Fire Hose Practices. 8th ed. Stillwater, OK: Fire Protection Publications, Oklahoma State University. International Fire Service Training Association.
- Carter W, Childress D, Coleman R, et al. [2000]. Firefighters Handbook: Essentials of firefighting and emergency response. Albany, NY: Delmar Thompson Learning.
- Hoffman, JJ [2002]. MAYDAY-MAYDAY-MAYDAY. Fire Department Safety Officers Association Health and Safety for Fire and Emergency Service Personnel 13(4):8.
- Angulo RA, Clark BA, Auch S [2004]. You called Mayday! Now what? Fire Engineering, Sept 2004, Vol. 157, No. 9, pp. 93-95.
- DiBernardo JP [2003]. A missing firefighter: Give the Mayday. Firehouse, Nov 2003, pp. 68-70.
- Sendelbach TE [2004]. Managing the fireground Mayday: The critical link to firefighter survival. http://www.firehouse.com/node/73134. (Link Updated 1/19/2010 - no longer available 1/8/2013) Date accessed: October 29, 2008.
- Miles J, Tobin J [2004]. Training notebook: Mayday and urgent messages. Fire Engineering, April 2004, Vol. 157, No. 4, pp. 22.
- NFPA [2008]. NFPA 1002 Standard for Fire Apparatus Driver/Operator Professional Qualifications. 2009 ed. Quincy, MA: National Fire Protection Association.
- NFPA [2008]. NFPA 1851 Standard on Selection, Care, and Maintenance of Structural Fire Fighting Protective Ensembles. Quincy, MA: National Fire Protection Association.
- NFPA [2007]. NFPA 1971 Standard on Protective Ensembles for Structural Fire Fighting and Proximity Fire Fighting, 2007 Edition. Quincy, MA: National Fire Protection Association.
- NFPA [2007]. NFPA 1981 Standard on Open-Circuit Self-Contained Breathing Apparatus for Fire and Emergency Services, 2007 Edition . Quincy, MA: National Fire Protection Association.
- NFPA [2007]. NFPA 1982 Standard on Personal Alert Safety Systems (PASS), 2007 Edition. Quincy, MA: National Fire Protection Association.
- NIOSH [2001]. Supermarket Fire Claims the Life of One Career Fire Fighter and Critically Injures Another Career Fire Fighter – Arizona. Morgantown, WV: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, Fatality Assessment and Control Evaluation (FACE) Report F2001-13.
- NFPA [2006]. NFPA 1404 Standard for Fire Service Respiratory Protection Training. Quincy, MA: National Fire Protection Association.
- Bernocco S, Gagliano M, Phippips C, and Jose P. [2008]. Is your department complying with the NFPA 1404 air management policy? Fire Engineering. Vol 161, No 2. February. Pp 103-108.
- Peterson JA and Merinar TR [1997]. Respirator Maintenance Program Recommendations for the Fire Service. Journal of the International Society for Respiratory Protection. Vol 15, Issues III & IV. Fall/Winter 1997.
- Corbin DE [2000]. Seeing is believing. Dallas, TX: Occupational Safety and Health, Aug 69(8): 60-67.
- NIOSH [2005]. NIOSH alert: preventing injuries and deaths of fire fighters due to truss system failures. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, DHHS (NIOSH) Publication No. 2005-132.
- Dunn V [2001]. The deadly lightweight truss. Firehouse. Jan:16-20.
- Brannigan FL [1999]. Building construction for the fire service. 3rd ed. Quincy, MA: National Fire Protection Association, pp. 517-563.
- USFA [2008]. Emergency Incident Rehabilitation Manual for Firefighters and Other Emergency Responders. U.S. Department of Homeland Security, U.S. Fire Administration. February 2008.
- USFA [2008]. Press Release: USFA Releases New Emergency Incident Rehabilitation Manual for Firefighters and Other Emergency Responders http://www.usfa.fema.gov/media/press/2008releases/031208.shtm. Date accessed: October 29, 2008. (Link Updated 1/17/2013)
- 72 Fed Reg 51735 [2007]. Emergency Response and Preparedness. Occupational Safety and Health Administration, Request for Information. Federal Register: September 11, 2007. Volume 72, Number 175. Page 51735-51743.
- NIOSH [2007]. Comments of the National Institute for Occupational Safety and Health on the Occupational Safety and Health Administration Request for Information: Emergency Response and Preparedness, Docket No. H-010. November 26, 2007. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, Cincinnati, Ohio. (Link Updated 1/14/2010)
- Davis WD, Donnelly MK, and Selepak MJ [2006]. Testing of portable radios in a fire fighting environment. NIST Technical Note 1477. National Institute of Standards and Technology. Gaithersburg, MD. Building and Fire Research Laboratory.
- USFA/FEMA [1999]. Improving firefighter communications. USFA-TR-099. Emmitsburg. MD: United States Fire Administration.
- TriData Corporation [2003]. Current status, knowledge gaps, and research needs pertaining to fire fighter radio communication systems. Report prepared for NIOSH. Arlington, VA: TriData Corporation.
- NIST [2007]. Advanced fire service technologies program. Proceedings of the 2007 NIST Annual Fire Conference. National Institute of Standards and Technology, Building and Fire Research Laboratory. Gaithersburg, MD.
- NIST [2008]. Wireless Sensor Research at NIST. National Institute of Standards and Technology, Building and Fire Research Laboratory. Gaithersburg, MD http://www.bfrl.nist.gov/WirelessSensor/. Date accessed October 29, 2008. (Link no longer available 12/6/2012)
- NFPA [1997]. Fire Protection Handbook, 18th ed. Quincy, MA: National Fire Protection Association. 1-42.
- BSRIA [2008]. New European standard for smoke extraction fans. Press Release. https://www.bsria.co.uk/services/design/mock-up-testing/test-and-certification/ (Link updated 10/28/2013 - no longer available 5/13/2015) Building Services Research and Information Association of Great Britain. Date accessed: October 29 2008.
INVESTIGATOR INFORMATION
This investigation was conducted by Timothy Merinar, Safety Engineer, Matt Bowyer, General Engineer, Jay Tarley, Safety and Occupational Health Specialist, and J. Scott Jackson, Occupational Nurse Practitioner, with the NIOSH Fire Fighter Fatality Investigation and Prevention Program. Stacy Wertman, Safety and Occupational Health Specialist, NIOSH, Division of Safety Research, provided technical support. This report was authored by Timothy Merinar. Jeffrey O. Stull, President, International Personnel Protection, Inc., conducted a forensic evaluation of the personal protective equipment (PPE), protective clothing and station uniforms worn by the victims. Expert technical reviews were provided by Chief Alan Brunacini (retired), Phoenix Fire Department; I. David Daniels, Fire Chief / Emergency Services Administrator, Renton Washington; Assistant Chief Vincent Dunn (retired), Fire Department of New York; Battalion Chief John Salka, Fire Department of New York and President of Fire Command Training; Gordon Routley, fire service consultant and FRT Project Leader; Kevin Roche, Phoenix Fire Department and FRT member; Nelson Bryner, National Institute of Standards and Technology (NIST), and Ken Farmer, U.S. Fire Administration (USFA).
Special thanks to Nelson Bryner, Paul Fuss, and Glenn Forney of NIST for their assistance during this investigation and to Lee Baughman, South Carolina OSHA, for his assistance at the site. The investigators would also like to thank the fire department, the International Association of Fire Fighters local union, local mutual aid departments, the county coroner, the city Director, Safety Management Division, and the city police department for their assistance during this investigation. Finally, a very special thank you to all the fire fighters who provided valuable information during this investigation.
photos and diagrams

|

|
Photo 2. Time approximately 1930 hours. Note how smoke has changed to dark black color indicating it is rich with products of incomplete combustion. Note Ladder 5 and Engine 11 in front of structure as well as fire department vehicle in lower left corner. The top of Engine 10 is just visible over the fence at the lower right. |

|
Photo 3. Time approximately 1934 hours. Note lack of any fire personnel in front of structure. At this point, the E-11, L-5, E-16, E-15, E-19, and E-6 crews are inside the showroom. Also note how the color of smoke column appears different from previous photo which may be due to the angle of the photograph and position of the sun. |

|
Photo 4. Last surviving members of the initial attack crews exit showroom at approximately 1935 hours. |
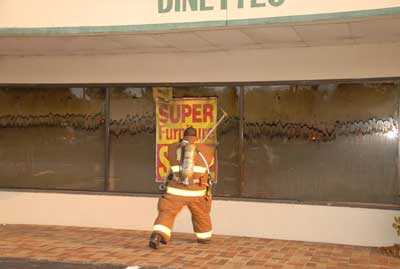
|
Photo 5. Time approximately 1935 hours. Mutual aid fire fighter breaking showroom front window. Photo taken just prior to mutual aid department making rescue attempt in front showroom. Note the heavy tar stains on the windows indicating the smoke inside the showroom is rich with flammable products of incomplete combustion. |

|
Photo 6. Time approximately 1936 hours. Note turbulent dark gray smoke rolling out of the showroom as the front windows are being knocked out. Mutual aid crew is assembling for search and rescue attempt. |

|
Photo 7. Time approximately 1938 hours. Photo shows conditions at front of showroom just before the interior search and rescue attempts were halted due to the interior conditions. |

|
Photo 8. Time approximately 1938 hours. Photo taken less than a minute after rescue crews are forced out of the showroom by the interior conditions. Note fire rolling out the showroom windows. |

|
Photo 9. Storage racks in warehouse post fire. Storage racks were filled with various furniture and mattress items. Note the extent to which the storage racks filled the warehouse which gives an indication of the volume of merchandise and the fuel load inside the 15,600 square foot warehouse. The warehouse measured approximately 130 ft. by 120 ft. and was 29 ft from floor to roof. |

|
Photo 10. Time approximately 1942 hours. Engine 10 and Engine 12 crews battle fire in warehouse from outside. |

|
Photo 11. Time approximately 1925 hours. Note traffic on major highway in front of incident site driving over 2 ½ inch supply line. The hose line runs from Engine 12 (to left of photo) to Engine 10 (to right of photo. Photo shows mutual aid crew members arriving on scene. |
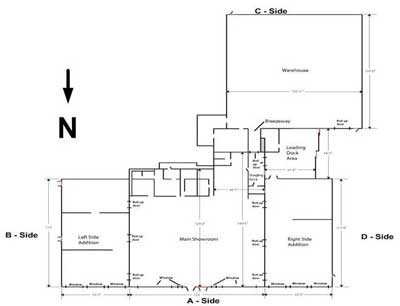
|

|
Diagram 2. Location of Engine 10 and Engine 11, supply lines and hose lines pulled at different times during the incident. Note accumulation of trash at loading dock on the day photo was taken, 3 months prior to the incident. Note the absence of ventilation ductworks or other roof penetrations over the showroom, thus no path for smoke and hot gases to escape. From aerial photo taken in March 2007 |

|
Diagram 3: Note location where mutual aid crew cut through exterior wall to extricate male employee trapped inside the warehouse. From aerial photo taken in 2007. (copyright Pictometry International used with permission of Pictometry) |
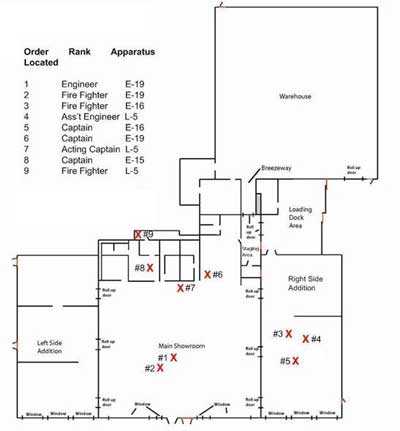
|
Diagram 4. Approximate location of the 9 victims. |
Appendix I
Recruit Class Schedule
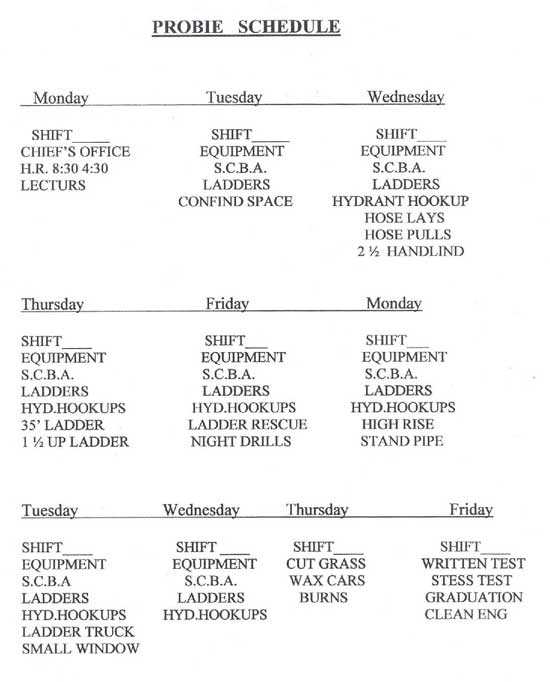
|
Appendix II
Appendix II
Engine 11 Inspection Report
Dated
December 16, 2008.
The fire department reported that no change had been made to
Engine 11 since the day of the fire.
 |
 |
Appendix III
Appendix III
Pre-plan Inspection Form
Pre-plan inspection form for the incident location. Note that names, addresses, phone numbers and other identifiers have been removed. Page 1 of 2.
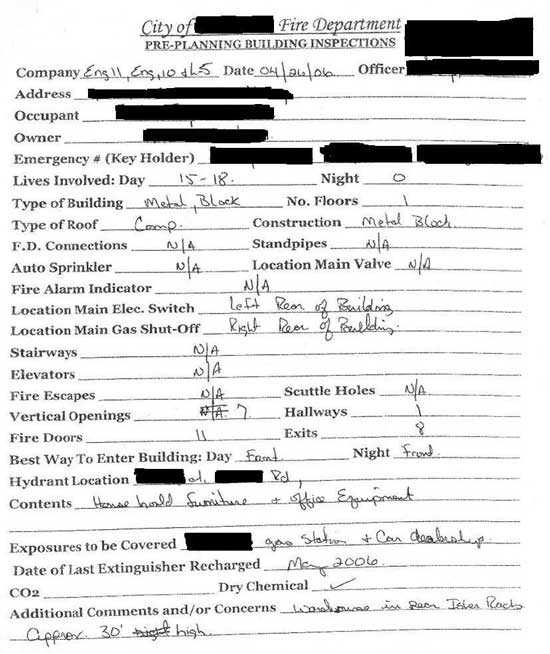
|
Pre-plan inspection form, page 2 of 2
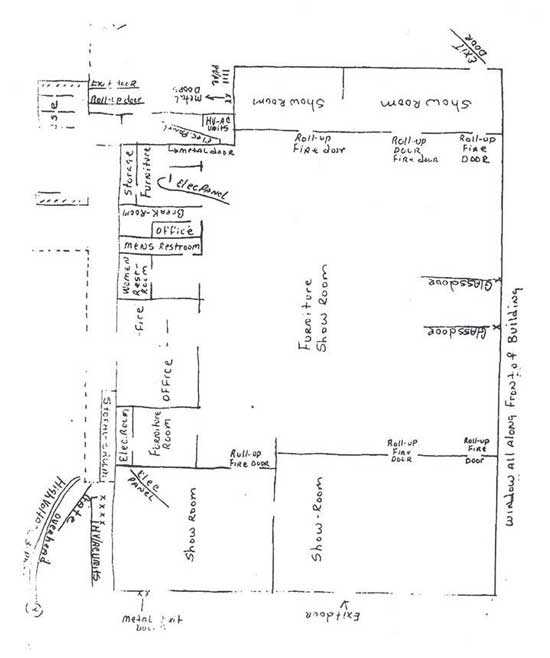
|
Appendix IV
Appendix IV
For a copy of the complete PPE Evaluation Report, contact
NIOSH Fire Fighter Fatality Investigation and Prevention Program
304-285-5916
Appendix V
Appendix V
Additional Photos




|
The National Institute for Occupational Safety and Health (NIOSH), an institute within the Centers for Disease Control and Prevention (CDC), is the federal agency responsible for conducting research and making recommendations for the prevention of work-related injury and illness. In fiscal year 1998, the Congress appropriated funds to NIOSH to conduct a fire fighter initiative. NIOSH initiated the Fire Fighter Fatality Investigation and Prevention Program to examine deaths of fire fighters in the line of duty so that fire departments, fire fighters, fire service organizations, safety experts and researchers could learn from these incidents. The primary goal of these investigations is for NIOSH to make recommendations to prevent similar occurrences. These NIOSH investigations are intended to reduce or prevent future fire fighter deaths and are completely separate from the rulemaking, enforcement and inspection activities of any other federal or state agency. Under its program, NIOSH investigators interview persons with knowledge of the incident and review available records to develop a description of the conditions and circumstances leading to the deaths in order to provide a context for the agencys recommendations. The NIOSH summary of these conditions and circumstances in its reports is not intended as a legal statement of facts. This summary, as well as the conclusions and recommendations made by NIOSH, should not be used for the purpose of litigation or the adjudication of any claim. To request additional copies of this report (specify the case number shown in the shield above), for other fatality investigation reports, or further information, visit the Program Website at
www.cdc.gov/niosh/fire/ or call toll free 1-800-CDC-INFO (1-800-232-4636).
|
This page was last updated on 02/11/09.
- Page last reviewed: November 18, 2015
- Page last updated: October 15, 2014
- Content source:
- National Institute for Occupational Safety and Health Division of Safety Research