

Use of the Internet for Health Information: United States, 2009
 ShareCompartir
ShareCompartir
On This Page
- Key findings
- Among adults aged 18 and over, women were more likely than men to have used the Internet for health information.
- Among adults aged 18–64, non-Hispanic white persons were almost twice as likely as Hispanic persons to have used the Internet for health information.
- Among adults aged 25–64, higher education was associated with increased use of the Internet for health information.
- Adults aged 18–64 with higher incomes were more likely to have used the Internet for health information than adults with lower incomes.
- Employed adults aged 18–64 were more likely than adults who were unemployed or not in the workforce to have used the Internet for health information.
- Using the Internet for health information was related to health insurance status.
- Summary
- Definitions
- Data source and methods
- About the authors
- References
- Suggested citation
NCHS Data Brief No. 66, July 2011
PDF Version (682 KB)
Robin A. Cohen, Ph.D.; and Patricia F. Adams
Key findings
Data from the National Health Interview Survey, 2009
- Among adults aged 18 and over, women were more likely than men to have used the Internet for health information.
- Among adults aged 18–64, non-Hispanic white persons were almost twice as likely as Hispanic persons to have used the Internet for health information.
- Adults aged 18–64 with higher incomes were more likely to have used the Internet for health information than adults with lower incomes.
- Employed adults aged 18–64 were more likely than adults who were unemployed or not in the workforce to have used the Internet for health information.
Research has shown that 74% of all U.S. adults use the Internet, and 61% have looked for health or medical information on the Internet (1). Additionally, 49% have accessed a website that provides information about a specific medical condition or problem. In 2009, the National Health Interview Survey (NHIS) became the first nationally representative household survey to collect data on the use of health information technology when the U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation sponsored 10 questions that asked about use of the Internet to look up health information, refill a prescription, schedule a medical appointment, learn about health topics in online chat groups, and e-mail a health care provider. This report provides estimates, using 2009 NHIS data, about adult use of the Internet for health information in the past 12 months, by selected sociodemographic characteristics.
Keywords: health information technology, Internet, National Health Interview Survey
Among adults aged 18 and over, women were more likely than men to have used the Internet for health information.
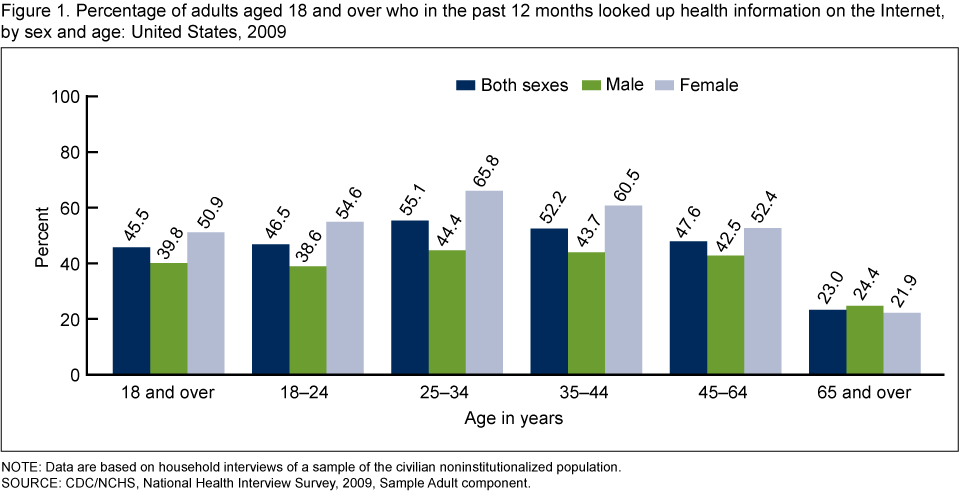
Women were more likely than men to have used the Internet for health information in the past 12 months for each age group except 65 and over (Figure 1).
The percentage of adults who used the Internet for health information was highest among women aged 25–34 (65.8%) and lowest among adults aged 65 and over (under 25%).
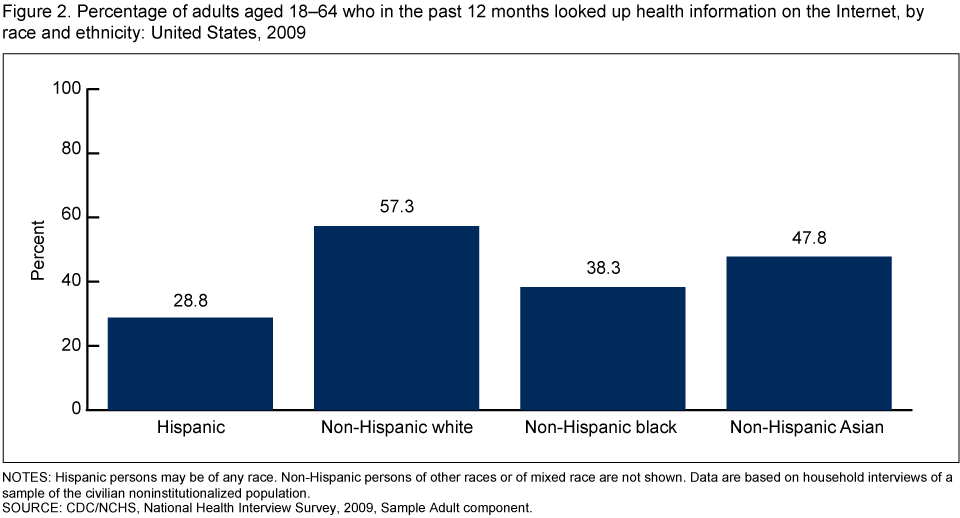
Among adults aged 18–64, non-Hispanic white persons were almost twice as likely as Hispanic persons to have used the Internet for health information.
Use of the Internet by adults aged 18–64 for health information in the past 12 months was highest for adults who were non-Hispanic white (57.3%), followed by non-Hispanic Asian (47.8%), non-Hispanic black (38.3%), and Hispanic (28.8%) (Figure 2).
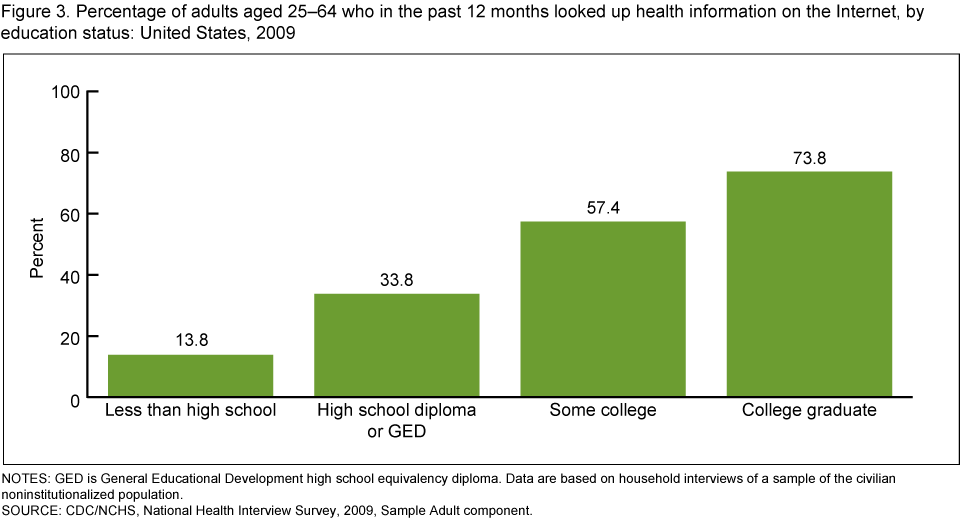
Among adults aged 25–64, higher education was associated with increased use of the Internet for health information.
Among adults aged 25–64, 73.8% of persons with at least a college degree used the Internet for health information in the past 12 months, while only 13.8% of those with less than a high school education did so (Figure 3).
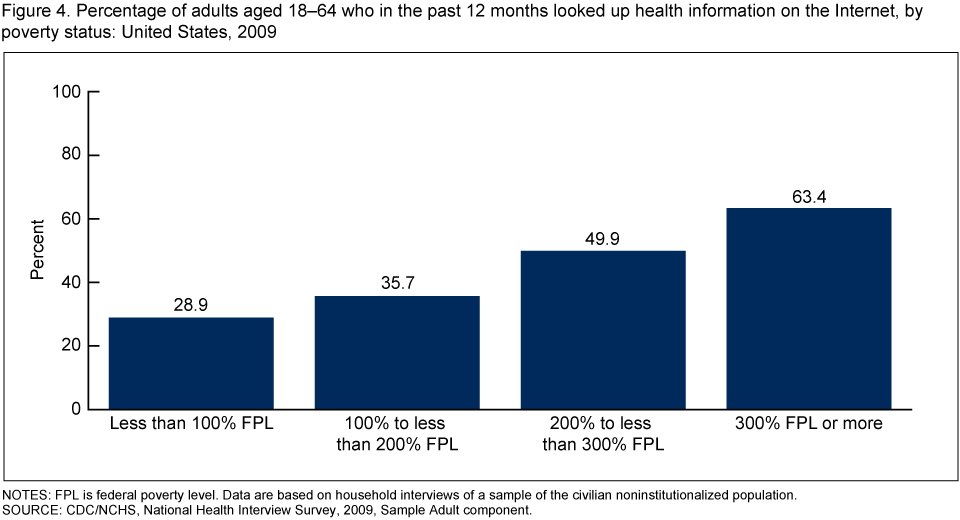
Adults aged 18–64 with higher incomes were more likely to have used the Internet for health information than adults with lower incomes.
Adults aged 18–64 with incomes at or above 300% of the federal poverty level (FPL) were more than twice as likely (63.4%) to have used the Internet for health information in the past 12 months compared with adults with incomes less than 100% of the FPL (28.9%) (Figure 4).
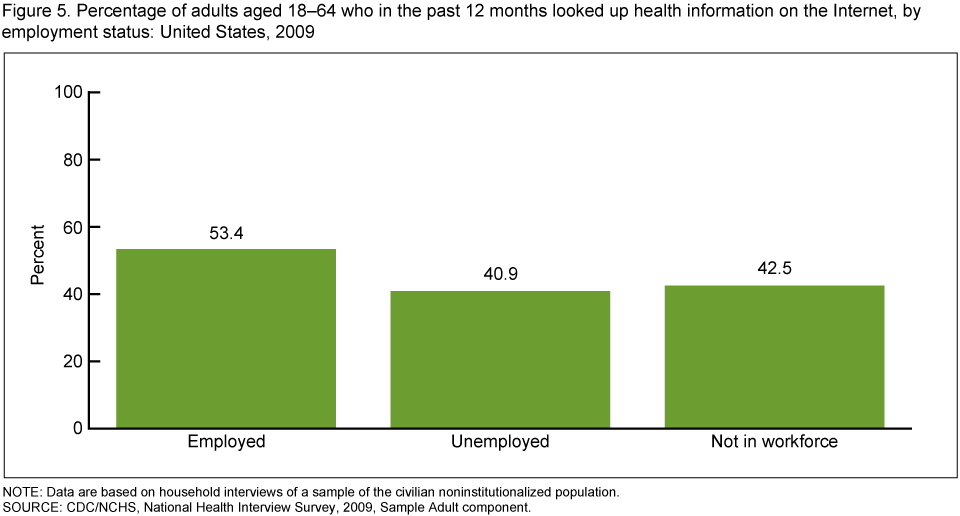
Employed adults aged 18–64 were more likely than adults who were unemployed or not in the workforce to have used the Internet for health information.
More than one-half (53.4%) of employed adults aged 18–64 used the Internet for health information in the past 12 months compared with 40.9% of unemployed adults and 42.5% of adults not in the workforce (Figure 5).
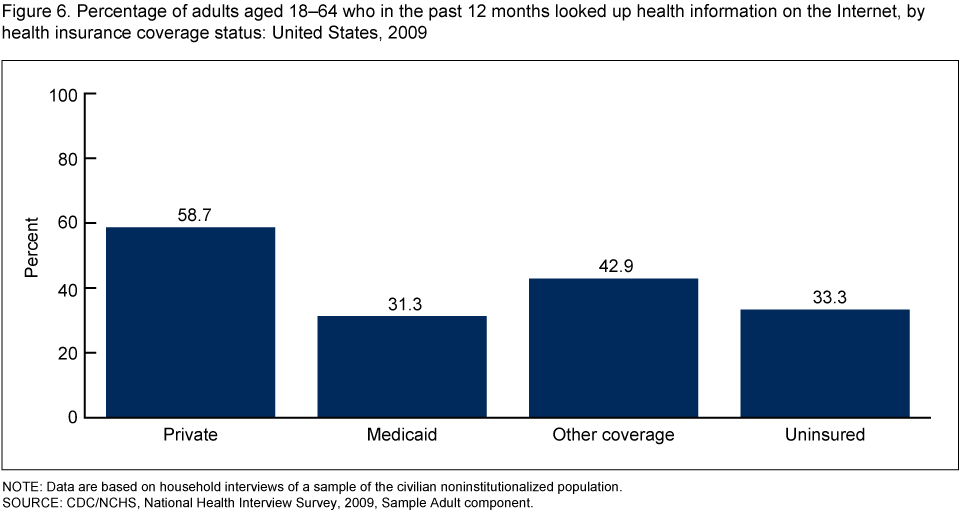
Using the Internet for health information was related to health insurance status.
Among adults aged 18–64, 58.7% of those with private health insurance coverage used the Internet for health information in the past 12 months compared with 31.3% of those on Medicaid and 33.3% of those with no insurance coverage (Figure 6).
Summary
Sociodemographic and socioeconomic factors were associated with adults who had used the Internet to look up health information. Greater use of the Internet for health information in the past 12 months among adults was associated with being ages 25–44, non-Hispanic white, employed, college educated, with income at or above 300% of the FPL, and having private health insurance.
The active involvement of consumers in managing their health care includes activities such as use of computers to access, retrieve, store, or share health care information. For consumers this may include using the Internet to look up health information, using e-mail or text messaging to communicate with health care providers or pharmacies, and having an electronic health record. As the percentage of adults in the United States using the Internet continues to grow, the Internet as a source of health information for consumers may become increasingly important. Although use of the Internet has the potential to improve consumer health by facilitating communication between providers and patients and among providers, previous research has found that many consumers are concerned about security and confidentiality issues related to scheduling medical appointments or accessing personal health records online (2).
Definitions
Looked up health information on the Internet in the past 12 months: Based on a positive response to both of the following questions: “Have you ever used computers for any of the following? … Looked up health information on the Internet” and “Did you look up health information on the Internet in the past 12 months?” Adults who answered “Refused” or “Don’t know” for either of these questions were excluded from the denominator for this analysis.
Poverty status and percentage of poverty level: Based on family income, family size, and the number of children in the family, and, for families with two or fewer adults, on the age of the adults in the family. The poverty level is based on definitions originally developed by the Social Security Administration. These include a set of income thresholds defining the FPL that vary by family size and composition. Families or individuals with incomes below their appropriate thresholds are classified as below the poverty level. These thresholds are updated annually by the U.S. Census Bureau to reflect changes in the Consumer Price Index for all urban consumers. For further information, visit the U.S. Census Bureau website. Estimates by poverty status are based on both reported and imputed family income. Family income information was completely missing for 5% of persons, and was only reported in broad categories for an additional 19% of persons in 2009. Therefore, family income was imputed for 24% of persons in 2009 using NHIS imputed income files (3). Note that NHIS asks respondents about their personal earnings and family income for the previous calendar year; therefore, U.S. Census Bureau poverty thresholds for the previous calendar year should be used when calculating poverty ratios for the current NHIS survey year. For example, the poverty ratios in the 2009 NHIS data files were calculated using the U.S. Census Bureau’s 2008 poverty thresholds (4).
Health insurance coverage: Defined broadly to include both public and private payers who cover medical expenditures incurred by a defined population in a variety of settings. This includes persons covered by private health insurance, whether offered through employment or purchased individually, and persons covered by public programs such as Medicare, Medicaid, Children’s Health Insurance Program (CHIP), and other state-sponsored programs. Persons with only Indian Health Service (IHS) coverage or having only a private plan that paid for one type of service such as accidents or dental care were not considered to be covered by health insurance. In this report, coverage is measured only on the day of the NHIS interview.
Private insurance: Indicated when respondents report that they were covered by private health insurance through an employer, union, or individual purchase. Private health insurance includes managed care such as health maintenance organizations and does not include military health plans.
Medicaid: Indicated when respondents report that they were covered by Medicaid. Individuals were also considered covered by Medicaid if they reported coverage by CHIP or other state-sponsored plans. In this analysis, health insurance categories are hierarchical, and adults covered by both private insurance and Medicaid were considered to have private insurance.
Other coverage: Includes persons who do not have private coverage or Medicaid (or other public coverage), but who have any type of military health plan (includes VA, TRICARE, and CHAMP–VA) or Medicare. This category also includes persons who are covered by other government programs.
Uninsured: Indicated when respondents report that they did not have coverage under private health insurance, Medicare, Medicaid, CHIP, another state-sponsored health plan, other government-sponsored programs, or a military health plan (TRICARE, VA, or CHAMP–VA). A person was also defined as uninsured if he or she had only IHS coverage or a private plan that paid for one type of service such as accidents or dental care.
Data source and methods
Data from the 2009 NHIS were used for this analysis. NHIS is conducted continuously throughout the year by interviewers of the U.S. Census Bureau for the Centers for Disease Control and Prevention’s (CDC) National Center for Health Statistics (NCHS). NHIS collects information about the health and health care of the civilian noninstitutionalized U.S. population. Interviews are conducted in respondents’ homes, but followups to complete interviews may be conducted over the telephone. In the Family component of the survey, family respondents are asked questions about everyone in the family, including questions about health insurance coverage. Questions on use of the Internet are from the Sample Adult component. In 2009, information was collected on a total of 27,731 persons aged 18 and over from the Sample Adult component of the survey. For further information about NHIS, including the questionnaire, visit the NHIS website.
NHIS is designed to yield a sample representative of the civilian noninstitutionalized population of the United States, and this analysis uses weights to produce national estimates. Data-weighting procedures are described in more detail elsewhere (5). Point estimates and estimates of corresponding variances for this analysis were calculated using SUDAAN software (6) to account for the complex sample design of NHIS. The Taylor series linearization method was chosen for variance estimation. Differences between percentages were evaluated using two-sided significance tests at the 0.05 level. Terms such as “higher than” and “less than” indicate statistically significant differences. Terms such as “similar” and “no difference” indicate that the statistics being compared were not significantly different. Lack of comment regarding the difference between any two statistics does not necessarily suggest that the difference was tested and found to be not significant.
About the authors
Robin A. Cohen and Patricia F. Adams are with CDC’s NCHS, Division of Health Interview Statistics.
References
- Fox S, Jones S. The social life of Internet users. Washington, DC: Pew Internet & American Life Project. 2009.
- The state of health information technology in California. Oakland, CA: California HealthCare Foundation. 2008.
- Schenker N, Raghunathan TE, Chiu PL, et al. Multiple imputation of family income and personal earnings in the National Health Interview Survey: Methods and examples [PDF – 813 KB].
- DeNavas-Walt C, Proctor BD, Smith JC. Income, poverty, and health insurance coverage in the United States: 2008 [PDF – 3 MB]. U.S. Census Bureau. Current population reports, P60–236. Washington, DC: U.S. Government Printing Office. 2009.
- Botman SL, Moore TF, Moriarity CL, Parsons VL. Design and estimation for the National Health Interview Survey, 1995–2004. National Center for Health Statistics. Vital Health Stat 2(130). 2000.
- Research Triangle Institute. SUDAAN (Release 10.0). Research Triangle Park, NC: Research Triangle Institute. 2008.
Suggested citation
Cohen RA, Adams PF. Use of the Internet for health information: United States, 2009. NCHS data brief, no 66. Hyattsville, MD: National Center for Health Statistics. 2011.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Edward J. Sondik, Ph.D., Director
Jennifer H. Madans, Ph.D., Associate Director for Science
Division of Health Interview Statistics
Jane F. Gentleman, Ph.D., Director
- Page last reviewed: November 6, 2015
- Page last updated: July 21, 2011
- Content source: