

Electronic Medical Record Adoption and Use in Home Health and Hospice
 ShareCompartir
ShareCompartir
On This Page
- Key findings
- Forty-one percent of all home health or hospice care providers had EMRs in 2007.
- Among providers with EMRs, almost all used components for patient demographics, and more than one-half used components for clinical notes, clinical decision support systems, or computerized physician order entry.
- Over one-half of providers with electronic medical records used three or fewer components.
- Providers with EMRs varied by profit status, ownership, and size.
- Summary
- Definitions
- Data source and methods
- About the authors
- References
- Suggested citation
NCHS Data Brief No. 45, September 2010
PDF Version (993 KB)
Anita Bercovitz, Ph.D.; Manisha Sengupta, Ph.D.; and Patricia Jamison, M.P.H.
Key findings
Data from the National Home and Hospice Care Survey, 2007
- In 2007, about 5,900 of the 14,500 providers of home health or hospice care (41%) had electronic medical records (EMRs), and an additional 2,200 (15%) planned to have EMRs within the next year. Providers who offered both hospice and home health care were more likely to have EMRs than providers offering only home health care, but did not differ from providers of hospice care only.
- Among providers with EMRs, 98% used components for recording patient demographics and 83% for clinical notes, and over one-half used clinical decision support systems or computerized physician order entry.
- Nonprofit and government providers, providers jointly owned or operated with other health care organizations, and providers with over 150 patients were more likely to have EMRs.
To promote the use of electronic health records (EHRs), the American Recovery and Reinvestment Act (ARRA) included financial incentives for meaningful users of EHRs (1). Although ARRA provisions and incentives apply primarily to physicians’ offices and hospitals, persons receiving home health and hospice care also receive care from physicians and hospitals. Coordination of care across sites of care through exchange of clinical information is one priority of ARRA (2). The increase in use of home health care from 1999 through 2007 (3) suggests that care coordination among other health providers and home health care will become increasingly important. Nationally representative data on electronic medical record (EMR) use by providers of home health and hospice care are limited. This report provides baseline estimates for EMR use by providers of home health or hospice care in 2007, prior to implementation of ARRA incentives.
Keywords: health information technology, long-term care, electronic health records
Forty-one percent of all home health or hospice care providers had EMRs in 2007.
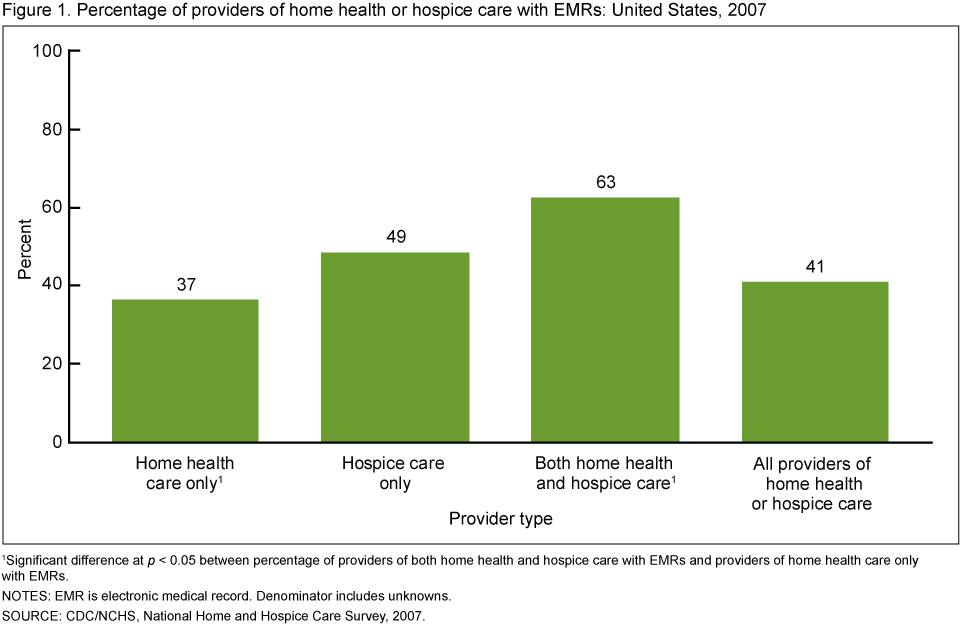
- Of the 14,500 providers of home health or hospice care in 2007, approximately 5,900 (41%) had EMRs (Figure 1) and an additional 2,200 (15%) had plans for acquiring EMRs within the next year.
- About 63% of providers offering both home health and hospice care had EMRs compared with 37% of providers offering home health care only. Forty-nine percent of providers of hospice care only had EMRs.
Among providers with EMRs, almost all used components for patient demographics, and more than one-half used components for clinical notes, clinical decision support systems, or computerized physician order entry.
- Of the 5,900 providers of home health or hospice care with EMRs, 98% used a component for patient demographics (Figure 2).
- Eighty-three percent of providers with EMRs used components for clinical notes, 57% for clinical decision support systems (CDSS), and 52% for computerized physician order entry (CPOE).
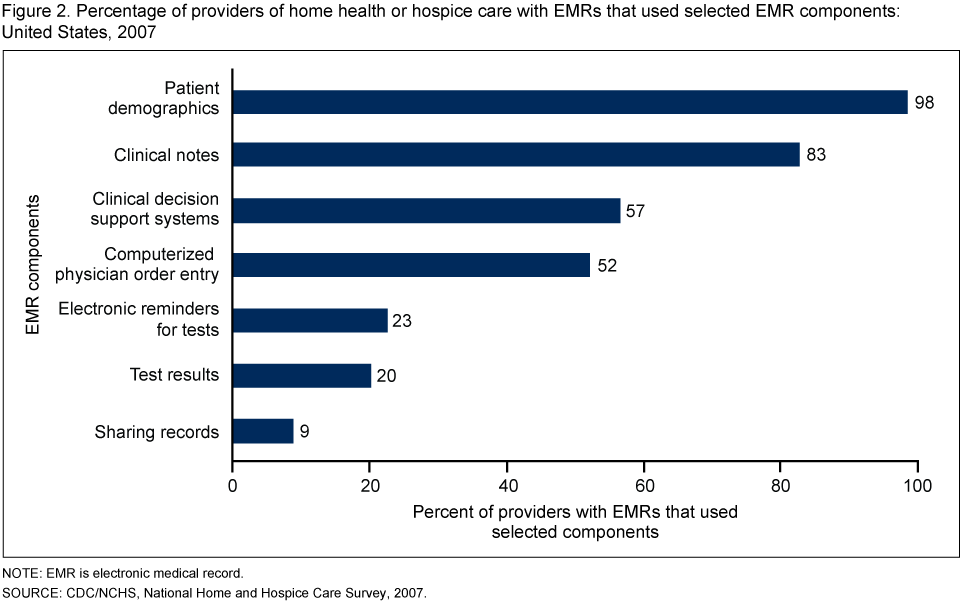
- Approximately one-fifth of providers with EMRs used components for test reminders (23%) and displaying test results (20%).
- Nine percent of providers with EMRs used the component for sharing records electronically with other agencies.
Over one-half of providers with electronic medical records used three or fewer components.
- Twenty-eight percent of providers with EMRs used one or two components, 28% used three components, 22% used four components, and 23% used five to eight components. No significant differences were found among the percentages of providers using differing numbers of components (Figure 3).

Providers with EMRs varied by profit status, ownership, and size.
- Nonprofit and government providers (68%) and providers that were jointly owned or operated by other health care organizations (62%) were more likely to have EMRs (see table)
- No significant differences existed in the proportion of providers with and without EMRs by whether: the providers were part of a chain; had contracts with managed care providers, assisted living facilities, skilled nursing facilities, or hospitals; or were located in a metropolitan statistical area (>see table).
- A greater proportion of providers with more than 150 patients had EMRs (60%) than providers with all other patient sizes (see table).
Table. Percentage of providers of home health or hospice care with selected provider characteristics, by whether had electronic medical records: United States, 2007
| Characteristic | Had EMR1 | No EMR1 |
|---|---|---|
| Total2 | 41 | 55 |
| Is provider part of a chain? | ||
| Yes | 33 | 65 |
| No | 45 | 50 |
| Is provider independent or owned by other organization?3 | ||
| Independent | 34 | 61 |
| Owned or operated by other organization4 | 62 | 38 |
| Is provider nonprofit or for profit?3 | ||
| Nonprofit or government owned | 68 | 29 |
| For profit | 26 | 68 |
| Does provider have a contract to provide services to: | ||
| Managed care providers – Yes | 49 | 47 |
| Assisted living facilities – Yes | 49 | 47 |
| Skilled nursing facility – Yes | 52 | 45 |
| Hospital – Yes | 45 | 51 |
| Is provider located in a metropolitan statistical area? | ||
| Yes | 40 | 54 |
| No5 | 44 | 55 |
| Total number of current patients6 | ||
| 0–50 | 34 | 62 |
| 51–100 | 39 | 57 |
| 101–150 | 33 | 66 |
| 151 or more | 60 | 34 |
1 At time of 2007 National Home and Hospice Care Survey.
2 Providers missing information on EMR are included in the denominator for calculating percentages. Percentages may not sum to 100 across rows due to missing data and rounding.
3 Significant difference among providers with EMRs by characteristic at p < 0.05.
4 Includes joint ownership or operation with outpatient medical or surgical center, managed care organization, hospital, skilled nursing facility, or other health care system.
5 Includes micropolitan statistical area and other.
6 Significant difference among providers with EMRs at p < 0.05 between providers with 151 or more current patients and all other patient categories.
NOTE: EMR is electronic medical record.
- No differences were found in whether providers had EMRs by their source of revenue, whether Medicare, Medicaid, private insurance, or patient out-of-pocket payments (results not shown).
Summary
Overall, 41% of providers of home health or hospice care had EMRs in 2007 and an additional 15% planned to obtain EMRs within the next year. This proportion was greater than the 35% of office-based physicians with EMRs in 2007 (4,5). Nonprofit and government providers, providers owned or operated with other health care organizations, and providers with over 150 patients were more likely to have EMRs. The association between size and having EMRs is similar to other studies among office-based physicians, hospitals, and nursing homes and a previous study of providers of home health or hospice care (5–8). Similarly, the association between joint ownership or operation and having an EMR is similar to other studies among physician groups jointly owned by other providers (9).
Of providers with EMRs, virtually all used a component for patient demographics (98%), 83% used components for clinical notes, 57% used CDSS, and 52% used CPOE. Over one-half (56%) of providers with EMRs used three or fewer components.
All EMR components included in this study are considered essential in achieving the improvements in quality and efficiency posited by use of EMRs, as highlighted in the proposed definition of meaningful use (2). However, less than one-half of providers of home health or hospice care had EMRs, and less than 10% of providers with EMRs used the component of sharing records with other agencies. To meet the ARRA priority to improve care coordination by electronic exchange of clinical information among providers across the spectrum of health care, EMR use among providers of home health or hospice care would need to increase significantly.
Definitions
EMRs and EHRs: Often used interchangeably to refer to electronic records of health-related information. However, one formal definition of an EMR is an electronic record based within one health care organization, while an EHR is interoperable and thus can be used by more than one health care organization (10).
Having an EMR: Based on agency self-report at time of the National Home and Hospice Care Survey (NHHCS) and is defined by a “yes” response to: “Does this agency currently have an Electronic Medical Records system? This is a computerized version of the patient’s medical information used in the management of the patient’s health care. Exclude electronic records used only for billing purposes and required documentation such as OASIS files.” If respondents answered “no” they were then asked, “Does this agency have plans to obtain an Electronic Medical Records System within the next year?”
Components of electronic medical records: Based on agency self-report of use of specific components at time of NHHCS. Specific component use is defined by a “used” response to: “With this agency’s current Electronic Medical Records system, please indicate for each component listed below, whether it is used, available but not used, or not available.” Components included CPOE for prescriptions, labs, and tests; test results (chest x-rays, labs, etc.); patient demographics; electronic reminders for tests (labs, imaging, etc.); CDSS for contraindications, allergies, guidelines, etc.; clinical notes; public health reporting (notifiable diseases); and sharing medical records electronically with other agencies. One agency (of the 1,036 that participated in the survey) reported having an EMR, but that all the components were not used although they were available.
Data source and methods
Data from the 2007 NHHCS were used for these analyses. The 2007 NHHCS used a stratified two-stage probability sample design. The first stage was the selection of home health and hospice care agencies from the sampling frame representing the universe of agencies providing home health and hospice care services in the United States. Agencies affiliated with hospitals, government entities, retirement centers, or similar institutions where the agencies maintained financial and patient records independent of the larger institution were included in the frame. The primary sampling strata of agencies were defined by agency type and metropolitan statistical area status. Within these sampling strata, agencies were sorted by census region, ownership, certification status, state, county, ZIP Code, and size (number of employees). For the 2007 NHHCS, 1,545 agencies were sampled with probability proportional to size. The unweighted response rate was 71%. The response rate weighted by the inverse of the probability of selection was 59% (11).
Differences among subgroups were evaluated using chi-square and t tests. All significance tests were two-sided using p < 0.05 as the level of significance. All comparisons reported in the text are statistically significant unless otherwise indicated. Data analyses were performed using the statistical packages SAS version 9.1 (SAS Institute, Cary, N.C.) and SUDAAN version 9.0 (Research Triangle Institute, Research Triangle Park, N.C.). Because estimates were rounded to the nearest hundred, individual estimates may not sum to totals.
About the authors
Anita Bercovitz and Manisha Sengupta are with the Centers for Disease Control and Prevention’s (CDC) National Center for Health Statistics (NCHS), Division of Health Care Statistics. Patricia Jamison is with CDC’s NCHS, Office of the Center Director.
References
- U.S. Department of Health and Human Services, Office of the National Coordinator for Health Information Technology. HealthIT.hhs.gov information related to the American Recovery and Reinvestment Act of 2009. [Accessed 6/10/10].
- U.S. Department of Health and Human Services. Medicare and Medicaid Programs; Electronic Health Record Incentive Program Final Rule. Federal Register 75(144):44314-588. 2010.
- Ng T, Harrington C, Kitchener M. Medicare and Medicaid in long-term care. Health Aff 29(1):22-88. 2010.
- Hsiao CJ, Beatty PC, Hing ES, et al. Electronic medical record/electronic health record use by office-based physicians: United States, 2008, and preliminary 2009. Health E-Stat. National Center for Health Statistics. 2009. [Accessed 6/24/10].
- Hing E, Hsiao CJ. Electronic medical record use by office-based physicians and their practices: United States, 2007. National health statistics reports; no 23. Hyattsville, MD: National Center for Health Statistics. 2010.
- Jha AK, DesRoches CM, Campbell EG, Donelan K, Rao SR, Ferris TG, et al. Use of electronic health records in U.S. hospitals. N Engl J Med 360(16):1628-38. 2009.
- Pearson WS, Bercovitz AR. Use of computerized medical records in home health and hospice agencies: United States, 2000. National Center for Health Statistics. Vital Health Stat 13(161). 2006.
- Resnick HE, Manard BB, Stone RI, Alwan M. Use of electronic information systems in nursing homes: United States, 2004. J Am Med Inform Assoc 16(2):179-86. 2009.
- Burt CW, Sisk JE. Which physicians and practices are using electronic medical records? Health Aff 24(5):1334-43. 2005.
- The National Alliance for Health Information Technology. Report to the Office of the National Coordinator for Health Information Technology on defining key health information technology terms [PDF – 376 KB]. 2008. [Accessed 6/10/10].
- Dwyer LL, Harris-Kojetin LD, Branden L, Shimizu IM. Redesign and operation of the National Home and Hospice Care Survey, 2007. National Center for Health Statistics. Vital Health Stat 1(53). 2010.
Suggested citation
Bercovitz A, Sengupta M, Jamison P. Electronic medical record adoption and use in home health and hospice. NCHS data brief, no 45. Hyattsville, MD: National Center for Health Statistics. 2010.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Edward J. Sondik, Ph.D., Director
Jennifer H. Madans, Ph.D., Associate Director for Science
Division of Health Care Statistics
Jane E. Sisk, Ph.D., Director
- Page last reviewed: November 6, 2015
- Page last updated: September 29, 2010
- Content source: