

Depression and Smoking in the U.S. Household Population Aged 20 and Over, 2005-2008
 ShareCompartir
ShareCompartir
On This Page
- Key findings
- Adults with depression were more likely to be current cigarette smokers than those without depression.
- The percentage of adults who were current smokers increased as depression severity increased.
- Adult smokers with depression were more likely to be heavy smokers than adult smokers without depression.
- Adults with depression were more likely to have ever smoked than those without depression. Among ever smokers, adults with depression were less likely to have quit smoking than those without depression.
- Summary
- Definitions
- Data source and methods
- About the authors
- References
- Suggested citation
NCHS Data Brief No. 34, April 2010
PDF Version (879 KB)
Laura A. Pratt, Ph.D., and Debra J. Brody, M.P.H.
Key findings
Data from the National Health and Nutrition Examination Surveys, 2005-2008
- Adults aged 20 and over with depression were more likely to be cigarette smokers than those without depression.
- Women with depression had smoking rates similar to men with depression, while women without depression smoked less than men.
- The percentage of adults who were smokers increased as depression severity increased.
- Among adult smokers, those with depression smoked more heavily than those without depression. They were more likely to smoke their first cigarette within 5 minutes of awakening and to smoke more than one pack of cigarettes per day.
- Adults with depression were less likely to quit smoking than those without depression.
Depression is a chronic disease that often results in limitations in work, family, and social life (1). Persons with depression have higher rates of cardiovascular disease and diabetes and more risk behaviors for these diseases, such as smoking, poor diet, or lack of exercise, than persons without depression (2).
Since 1964, when the Surgeon General’s first Report on Smoking and Health was released (3), cigarette smoking among adults in the United States has been reduced by one-half. However, 21% of the adult population still smokes (4). Better understanding the characteristics of adults who continue to smoke and the relationship between smoking and depression may lead to improved tobacco cessation interventions (5).
Keywords: mental illness, tobacco, National Health and Nutrition Examination Survey
Adults with depression were more likely to be current cigarette smokers than those without depression.
1 All comparisons between depression and no depression are significant (p < 0.05).
NOTE: Access data table for Figure 1. [XLS – 20 KB] [CSV – 1 KB]
SOURCE: CDC/NCHS, National Health and Nutrition Examination Surveys, 2005-2008.
In every sex-age group, adults with depression were more likely to smoke than those without depression (Figure 1).
Over one-half of men with depression aged 40-54 were current smokers compared with 26% of men without depression of the same age.
Among women aged 40-54, of those with depression, 43% were smokers compared with 22% of those without depression.
Among adults with depression, men and women had similar rates of smoking, whereas among adults without depression, men were more likely to be smokers than women.
The percentage of adults who were current smokers increased as depression severity increased.
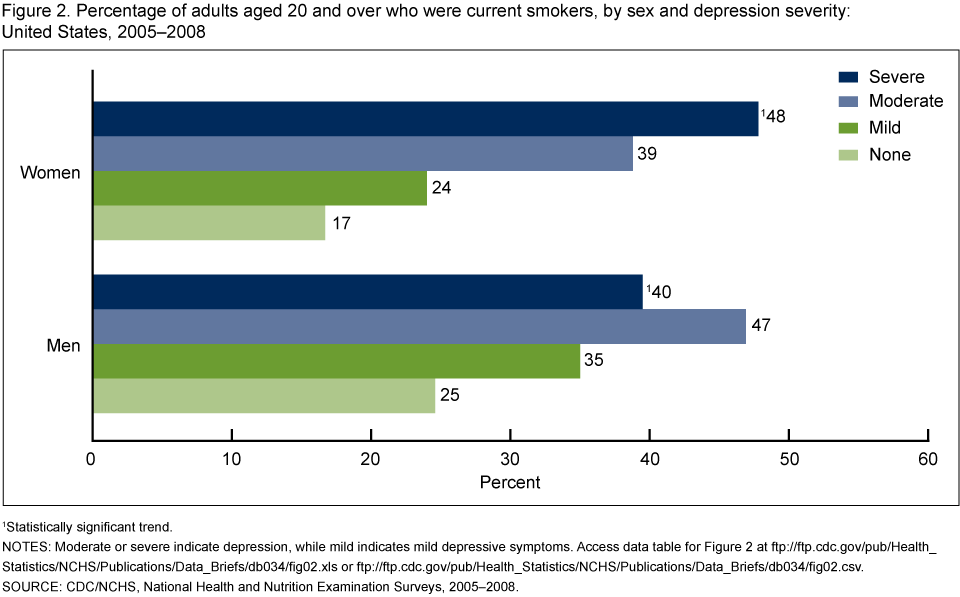
1 Statistically significant trend.
NOTES: Moderate or severe indicate depression, while mild indicates mild depressive symptoms. Access data table for Figure 2. [XLS – 20 KB] [CSV – 1 KB]
SOURCE: CDC/NCHS, National Health and Nutrition Examination Surveys, 2005-2008.
Adults with even mild depressive symptoms were more likely to smoke than adults with no depressive symptoms (Figure 2).
Among adults with moderate or severe depressive symptoms, women and men had similar high rates of smoking ranging from 39% to 48%.
More than one-quarter of men with mild or no depressive symptoms smoked, while less than one-fifth of women with mild or no depressive symptoms did so.
Adult smokers with depression were more likely to be heavy smokers than adult smokers without depression.
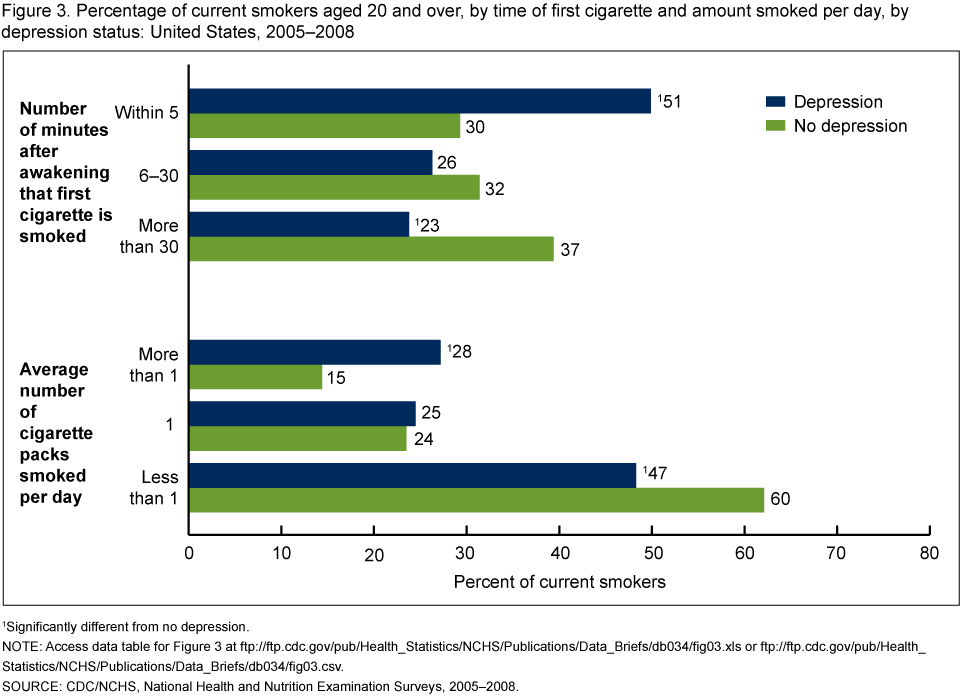
1 Significantly different from no depression.
NOTE: Access data table for Figure 3. [XLS – 20 KB] [CSV – 2 KB]
SOURCE: CDC/NCHS, National Health and Nutrition Examination Surveys, 2005-2008.
Slightly more than one-half of adult smokers with depression smoked their first cigarette of the day within 5 minutes of waking up, while 30% of smokers without depression smoked their first cigarette within 5 minutes of awakening (Figure 3).
Twenty-eight percent of adult smokers with depression smoked more than a pack of cigarettes per day, which was almost twice the rate for adult smokers without depression.
Adults with depression were more likely to have ever smoked than those without depression. Among ever smokers, adults with depression were less likely to have quit smoking than those without depression.
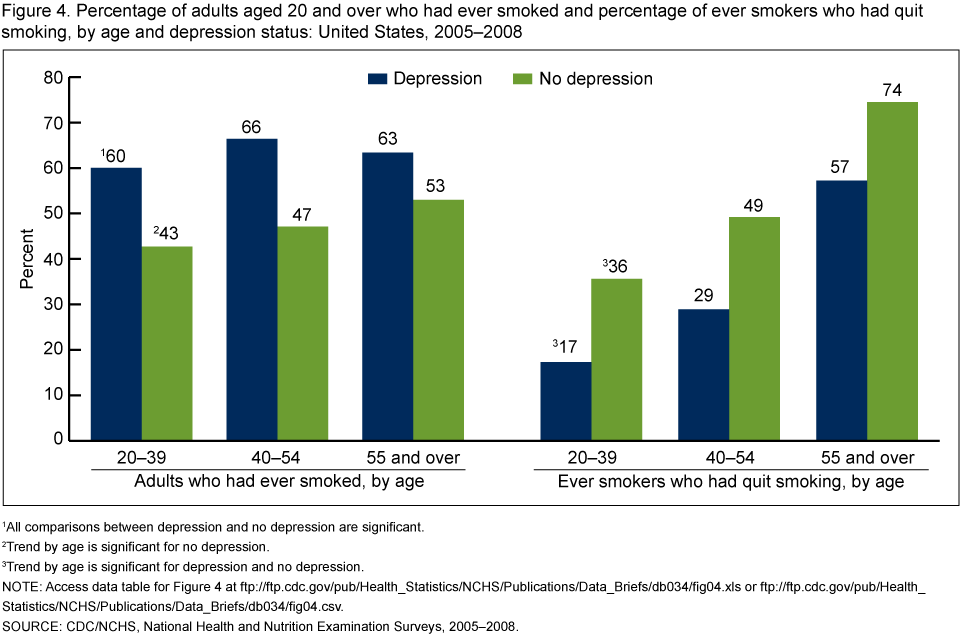
1 All comparisons between depression and no depression are significant.
2 Trend by age is significant for no depression.
3 Trend by age is significant for depression and no depression.
NOTE: Access data table for Figure 4. [XLS – 20 KB] [CSV – 1 KB]
SOURCE: CDC/NCHS, National Health and Nutrition Examination Surveys, 2005-2008.
Over 60% of adults with depression had smoked at some point in their lives (ever smokers), and the rate was similar across age groups. Among adults without depression, the proportion who were ever smokers ranged from 43% among those aged 20-39 to 53% among persons aged 55 and over (Figure 4).
In every age group, ever smokers with depression were less likely to have quit smoking than ever smokers without depression.
The percentage of ever smokers who no longer smoke increased with age both among persons with depression and persons without depression.
Among ever smokers aged 20-39 with depression, 17% had quit smoking, whereas 36% of persons in this age group without depression had quit smoking. Among ever smokers aged 55 and over with depression, 57% had quit smoking while almost 75% of persons in this age group without depression had quit.
Summary
About 7% of adults aged 20 and over had depression in 2005-2008, based on National Health and Nutrition Examination Survey (NHANES) data. Persons with depression were more likely to be current smokers than persons without depression. Almost one-half of adults under age 55 with current depression were current smokers, while less than one-quarter of people in this age group without depression were smokers.
The proportion of adults who were current smokers tended to increase with an increase in depression severity. Even persons with mild depressive symptoms below the threshold for the diagnosis of depression were more likely to be smokers than people with no depressive symptoms.
Adults with depression were more likely to smoke over a pack a day and smoke their first cigarette within 5 minutes of waking up than were adults without depression. Both of these are indicators of heavy smoking. Heavy smoking is highly correlated with inability to quit (6,7).
Those with depression had a higher rate of smoking initiation (ever smoking) as well as a lower quit rate. They were also heavier smokers than persons without depression. Individuals with other mental illnesses have similar smoking patterns (8,9). Studies have shown that persons with depression and other mental illnesses smoke a disproportionate share of all the cigarettes consumed in the United States (8).
The few studies that have examined ability to quit smoking in persons with depression have shown that with intensive treatment, persons with depression can quit smoking and remain abstinent. These intensive cessation services often use treatments that are also used for depression, including cognitive-behavioral therapy or antidepressant medications (5). Adults with depression and other mental illnesses are an important subgroup to target for tobacco cessation programs.
Definitions
Depression: Measured in NHANES using the Patient Health Questionnaire (PHQ-9), a 9-item screener that asks questions about the frequency of symptoms of depression over the past 2 weeks (10). In the PHQ-9, response categories “not at all,” “several days,” “more than half the days,” and “nearly every day” are given a score ranging from 0 (not at all) to 3 (more than half the days). A total score is calculated ranging from 0 to 27. Depression was defined as a PHQ-9 score of 10 or higher, a cut point that has been well validated and is commonly used in clinical studies that measure depression (10). No depression was defined as a PHQ-9 score of 0-9.
The PHQ-9 is based on the diagnostic criteria for major depressive disorder in the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition. Major depression includes mood symptoms such as feelings of sadness or irritability, loss of interest in usual activities, inability to experience pleasure, feelings of guilt or worthlessness, and thoughts of death or suicide, cognitive symptoms such as inability to concentrate and difficulty making decisions, and physical symptoms such as fatigue, lack of energy, feeling restless or slowed down, and changes in sleep, appetite, and activity levels (11).
In NHANES, it is possible that severely depressed persons disproportionately chose not to participate in the survey or health examination, which included administration of the PHQ-9. Because smoking rates increase with depression severity, it is possible that the prevalence estimates in this report may underestimate the actual prevalence rate of smoking among persons with depression. In addition, people who are being successfully treated for depression will not be identified by the PHQ-9 as depressed.
Because the PHQ-9 instrument assesses depression in the past 2 weeks only, the depression status of persons at the time of cigarette smoking initiation or time of quitting is not known.
Depression severity: Refers to the severity of depressive symptoms. The following four severity categories were defined based on the total score from the PHQ-9 screening instrument (10):
- None or minimal 0-4
- Mild 5-9
- Moderate 10-14
- Severe 15 or more
These depression severity categories are used in Figure 2. In Figures 1, 3, and 4, none or minimal and mild depressive symptoms (PHQ-9 scores of 0-9) correspond to “no depression,” while moderate and severe depressive symptoms (scores of 10 or more) correspond to “depression.”
Current smoker: Defined by the question, “Do you now smoke cigarettes?” Persons who responded “every day” or “some days” were included in the current smoker category. Persons who reported using only other forms of tobacco were not included in this definition.
Heavy smokers: Identified by two questions: “How soon after you wake up do you smoke? Would you say. . .five minutes, from six to thirty minutes, from more than 30 minutes to one hour, or more than one hour?” and “During the past 30 days, on the days that you smoked, how many cigarettes did you smoke per day?” The average number of cigarettes per day was then categorized as less than one pack per day (less than 20 cigarettes), a pack a day (20 cigarettes), and more than a pack a day. In population studies, these two questions are a common way to measure heavy smoking, which is highly related to nicotine dependence and ability to quit (6,7).
Ever smokers: Defined as answering “yes” to the question, “Have you smoked at least 100 cigarettes in your entire life?” Ever smokers include current and former smokers.
Former smokers or persons who have quit smoking: Defined as answering “yes” to the question, “Have you smoked at least 100 cigarettes in your entire life?” and “no” to the question, “Do you now smoke cigarettes?” The percentage of persons who have quit smoking is calculated using a “quit ratio” defined as the number of former smokers divided by the number of ever smokers (12).
Data source and methods
NHANES is a continuous survey of the civilian noninstitutionalized U.S. population conducted to assess the health and nutrition of Americans. Persons living in institutions, where rates of depression and smoking are higher than in the community, are not included in NHANES. Survey participants complete a household interview and visit a mobile examination center (MEC) for a physical examination and private interview. The annual interview and examination sample includes approximately 5,000 persons of all ages. In 2005-2006, non-Hispanic black persons, Mexican-American persons, adults aged 60 and over, and low income persons were oversampled to improve the statistical reliability of the estimates for these groups. In 2007-2008, the same groups were oversampled except that rather than oversampling only Mexican-American persons, all Hispanic persons were oversampled.
This report is based on the analysis of data from interviews in the household and in the MEC. The questions on cigarette smoking were asked in the household interview and the depression questions were asked in the MEC. Questions were administered in English and Spanish. Persons who reported using only forms of tobacco other than cigarettes were not considered smokers for this analysis.
The NHANES sample examination weights, which account for the differential probabilities of selection, nonresponse, and noncoverage, were used for all analyses. Standard errors of the percentages were estimated using Taylor series linearization, a method that incorporates the sample design and weights.
Differences between subgroups were evaluated using the univariate t statistic. A test for trends was done to evaluate changes in the estimates by depression severity and to test for trends by age in Figure 4. All significance tests were two-sided using p < 0.05 as the level of significance. All comparisons reported are statistically significant unless otherwise indicated. Data analyses were performed using SAS version 9.2 (SAS Institute, Cary, N.C.) and SUDAAN version 9.0 (RTI, Research Triangle Park, N.C.).
About the authors
Laura A. Pratt is with the Centers for Disease Control and Prevention’s National Center for Health Statistics, Office of Analysis and Epidemiology. Debra J. Brody is with the Centers for Disease Control and Prevention’s National Center for Health Statistics, Division of Health and Nutrition Examination Surveys.
References
- Wells KB, Stewart A, Hays RD, Burnam MA, Rogers W, Daniels M, et al. The functioning and well-being of depressed patients. Results from the Medical Outcomes Study. JAMA 262(7):914-9. 1989.
- Katon WJ. Clinical and health services relationships between major depression, depressive symptoms, and general medical illness. Biol Psychiatry 54(3):216-26. 2003.
- Office of the Surgeon General. Smoking and Health. Washington, DC: Public Health Service. 1964.
- National Center for Health Statistics. Health, United States, 2008, with chartbook. Hyattsville, MD: 2009.
- Ziedonis D, Hitsman B, Beckham JC, Zvolensky M, Adler LE, Audrain-McGovern J, et al. Tobacco use and cessation in psychiatric disorders: National Institute of Mental Health report. Nicotine Tob Res 10(12):1691-715. 2008.
- Heatherton TF, Kozlowski LT, Frecker RC, Rickert W, Robinson J. Measuring the heaviness of smoking: Using self-reported time to the first cigarette of the day and number of cigarettes smoked per day. Br J Addict 84(7):791-9. 1989.
- Hymowitz N, Cummings KM, Hyland A, Lynn WR, Pechacek TF, Hartwell TD. Predictors of smoking cessation in a cohort of adult smokers followed for five years. Tob Control 6 Suppl 2:S57-62. 1997.
- Lasser K, Boyd JW, Woolhandler S, Himmelstein DU, McCormick D, Bor DH. Smoking and mental illness: A population-based prevalence study. JAMA 284(20):2606-10. 2000.
- Grant BF, Hasin DS, Chou SP, Stinson FS, Dawson DA. Nicotine dependence and psychiatric disorders in the United States: Results from the National Epidemiological Survey on Alcohol and Related Conditions. Arch Gen Psychiatry 61(11):1107-15. 2004.
- Kroenke K, Spitzer RL, Williams JB. The PHQ-9: Validity of a brief depression severity measure. J Gen Intern Med 16:606-13. 2001.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition. Washington, DC: American Psychiatric Association. 2000.
- Anda RF, Williamson DF, Escobedo LG, Mast EE, Giovino GA, Remington PL. Depression and the dynamics of smoking: A national perspective. JAMA 264(12):1541-5. 1990.
Suggested citation
Pratt LA, Brody DJ. Depression and smoking in the U.S. household population aged 20 and over, 2005-2008. NCHS data brief, no 34. Hyattsville, MD: National Center for Health Statistics. 2010.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Edward J. Sondik, Ph.D., Director
Jennifer H. Madans, Ph.D., Associate Director for Science
Office of Analysis and Epidemiology
Linda T. Bilheimer, Ph.D., Director
- Page last reviewed: November 6, 2015
- Page last updated: April 14, 2010
- Content source: