

Physician Office Visits by Children for Well and Problem-focused Care: United States, 2012
 ShareCompartir
ShareCompartir
On This Page
- Key findings
- Physician office visit rates for all visits and for well and problem-focused care were lower for children aged 6–17 than for children aged 5 and under.
- Visit rates to general pediatricians were higher compared with visit rates to other primary care physicians and medical and surgical specialists for both types of visits.
- Across age groups, well-care visits had recommended weight, height, and blood pressure measurements recorded more frequently compared with problem-focused visits.
- Summary
- Definitions
- Data source and methods
- About the authors
- References
- Suggested citation
NCHS Data Brief No. 248, May 2016
PDF Version (316 KB)
Sayeedha G. Uddin, M.D., M.P.H.; Kathleen S. O’Connor, M.P.H.; and Jill J. Ashman, Ph.D.
Key findings
Data from the National Ambulatory Medical Care Survey, 2012
- Physician office visit rates for well care were lower for school-aged (those aged 6–11 years) children (31 per 100 population) and adolescents aged 12–17 years (29 per 100 population) than for younger children (349 and 74 per 100 population for children under age 1 year and 1–5 years, respectively).
- Visit rates for well and problem-focused care were highest for general pediatricians (59 and 173 per 100 population) compared with other primary (7 and 25 per 100 population) and specialty care providers (1 and 24 per 100 population) across all age groups.
- Among school-aged and adolescent children, a higher percentage of well-care visits had recommended height, weight, and blood pressure measurements recorded, compared with visits for problem-focused care.
Office visits by children can be for well or problem-focused care. Well-care visits for children routinely include assessment of emotional and social development, in addition to physical health and development (1). Problem-focused visits do not routinely include these comprehensive assessments. Receipt of well care is tracked nationally as a measure of health care quality (2). This report describes physician office visits for well and problem-focused care among children under age 18 years. This analysis complements the information on children’s visits contained in the National Ambulatory Medical Care Survey (NAMCS) 2012 online tables (3).
Keywords: well-child care, ambulatory care, National Ambulatory Medical Care Survey
Physician office visit rates for all visits and for well and problem-focused care were lower for children aged 6–17 than for children aged 5 and under.
- In 2012, there were approximately 171 million visits to physician offices made by children under age 18, for an overall visit rate of 232 visits per 100 population (Figure 1).
- The rate of problem-focused visits (173 per 100 population) was higher than the rate of well-care visits (59 per 100 population).
- The visit rates for well care (349 per 100 population) and problem-focused care (359 per 100 population) did not differ for children under age 1, but the rates for this group were higher than for older children.
- The visit rates for children aged 1–5 for both well care and problem-focused care were higher than the rates for older children.
- The rates of well-care and problem-focused visits (31 and 139 per 100 population, respectively) for children aged 6–11 were similar to the rates for children aged 12–17 (29 and 153 per 100 population, respectively).
- Among children at least age 1, rates of problem-focused visits were higher than those of well-care visits (203 per 100 population for problem-focused visits compared with 74 per 100 population for well-care visits for those aged 1–5; 139 per 100 population compared with 31 per 100 population for those aged 6–11; and 153 per 100 population compared with 29 per 100 population for those aged 12–17).
Figure 1. Physician office visit rates for children under age 18 years, by age group and visit type: United States, 2012
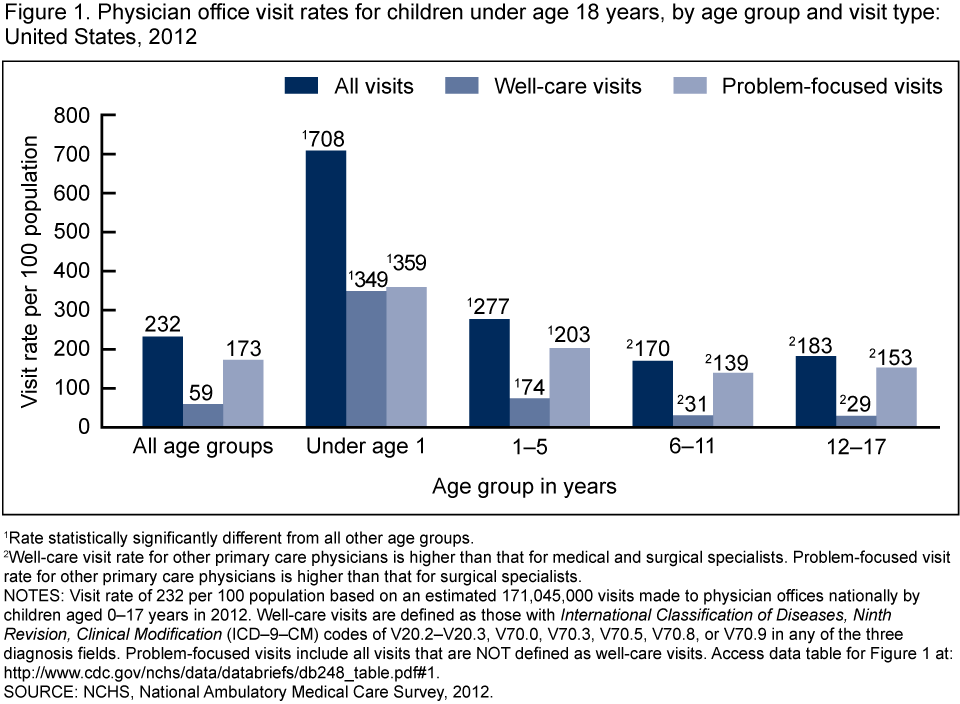
1Rate statistically significantly different from all other age groups.
2Well-care visit rate for other primary care physicians is higher than that for medical and surgical specialists. Problem-focused visit rate for other primary care physicians is higher than that for surgical specialists.
NOTES: Visit rate of 232 per 100 population based on an estimated 171,045,000 visits made to physician offices nationally by children aged 0–17 years in 2012. Well-care visits are defined as those with International Classification of Diseases, Ninth Revision, Clinical Modification (ICD–9–CM) codes of V20.2–V20.3, V70.0, V70.3, V70.5, V70.8, or V70.9 in any of the three diagnosis fields. Problem-focused visits include all visits that are NOT defined as well-care visits. Access data table for Figure 1.
SOURCE: NCHS, National Ambulatory Medical Care Survey, 2012.
Visit rates to general pediatricians were higher compared with visit rates to other primary care physicians and medical and surgical specialists for both types of visits.
- The rates of both well-care (51 per 100 population) and problem-focused visits (105 per 100 population) were highest for general pediatricians compared with all other physician specialties (Figure 2).
- The rate of well-care visits was higher for other primary care physicians (7 per 100 population) compared with medical specialists (1 per 100 population) and surgical specialists (estimate does not meet standards of reliability or precision).
- The rate of problem-focused care visits was higher for other primary care physicians (25 per 100 population) compared with surgical specialists (19 per 100 population).
- The rates of visits for problem-focused care were similar between medical (24 per 100 population) and surgical specialists (19 per 100 population).
Figure 2. Physician office visit rates, by physician specialty and visit type for children under age 18 years: United States, 2012
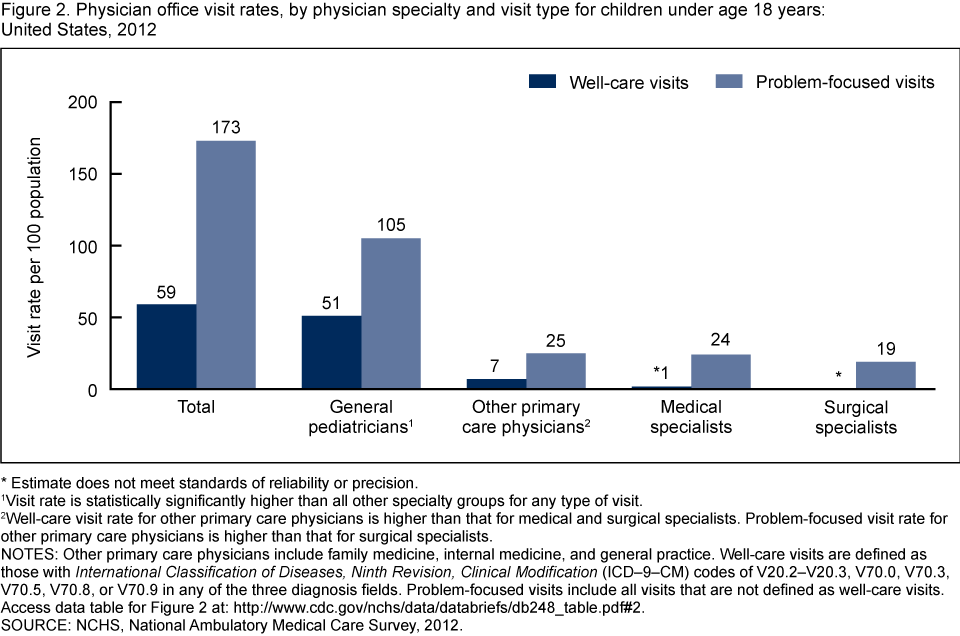
*Estimate does not meet standards of reliability or precision.
1Visit rate is statistically significantly higher than all other specialty groups for any type of visit.
2Well-care visit rate for other primary care physicians is higher than that for medical and surgical specialists. Problem-focused visit rate for other primary care physicians is higher than that for surgical specialists.
NOTES: Other primary care physicians include family medicine, internal medicine, and general practice. Well-care visits are defined as those with International Classification of Diseases, Ninth Revision, Clinical Modification (ICD–9–CM) codes of V20.2–V20.3, V70.0, V70.3, V70.5, V70.8, or V70.9 in any of the three diagnosis fields. Problem-focused visits include all visits that are not defined as well-care visits. Access data table for Figure 2.
SOURCE: NCHS, National Ambulatory Medical Care Survey, 2012.
Across age groups, well-care visits had recommended weight, height, and blood pressure measurements recorded more frequently compared with problem-focused visits.
- The percentage of visits with recommended weight, height, and blood pressure measurement recorded was higher for well-care visits compared with problem-focused visits for both age groups 6–11 years and 12–17 years (Figure 3).
- Weight was recorded at a lower percentage of problem-focused visits for children aged 12–17 (75%) compared with children aged 6–11 (83%). No difference was observed in the percentage of well-care visits with weight recorded for children aged 6–11 (97%) compared with children aged 12–17 (97%).
- No differences were observed in the percentage of well-care visits with height measurement recorded for children aged 6–11 relative to children aged 12–17 (92% compared with 94%, respectively), and for problem-focused visits (50% compared with 52%, respectively).
- Blood pressure measurement was recorded for a greater percentage of visits made by children aged 12–17 relative to children aged 6–11 for both well-care visits and problem-focused visits (93% compared with 82%, and 50% compared with 39%, respectively).
Figure 3. Percentage of physician office visits by children aged 6–17 years with recommended weight, height, and blood pressure measurement recorded, by age group and type of visit: United States, 2012
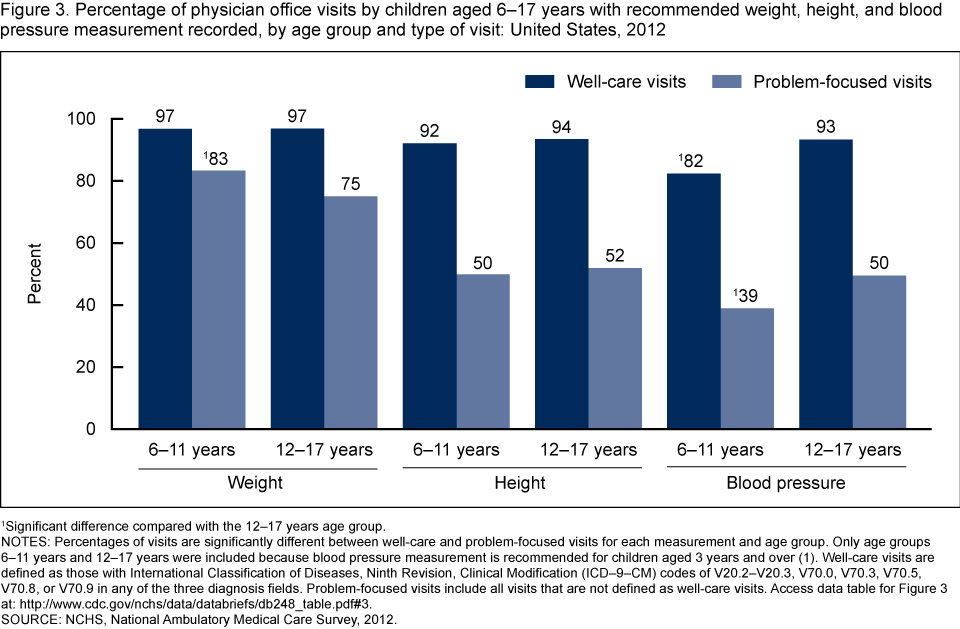
1Significant difference compared with the 12–17 years age group.
NOTES: Percentages of visits are significantly different between well-care and problem-focused visits for each measurement and age group. Only age groups 6–11 years and 12–17 years were included because blood pressure measurement is recommended for children aged 3 years and over (1). Well-care visits are defined as those with International Classification of Diseases, Ninth Revision, Clinical Modification (ICD–9–CM) codes of V20.2–V20.3, V70.0, V70.3, V70.5, V70.8, or V70.9 in any of the three diagnosis fields. Problem-focused visits include all visits that are not defined as well-care visits. Access data table for Figure 3.
SOURCE: NCHS, National Ambulatory Medical Care Survey, 2012.
Summary
Consistent with other studies (2,4), visit rates for well care were generally lower for older children. The visit rates for school-aged children and adolescents were similar. General pediatricians provide the majority of care to children, including both well-care and problem-focused care visits. Recommended measurement of height, weight, and blood pressure (1) were more often documented during well-care visits, emphasizing the importance of this type of visit.
Definitions
Well-care visits: Defined as those with International Classification of Diseases, Ninth Revision, Clinical Modification (ICD–9–CM) (5) codes of V20.2–V20.3, V70.0, V70.3, V70.5, V70.8, or V70.9 in any of the three diagnosis fields. These visits can include care for illness or problems.
Problem-focused visit: Includes all visits that are not defined as well-care visits (see above).
Medical specialist: Includes all specialties not defined as primary care or surgical care. For a complete listing, see the 2012 Documentation (6).
Surgical specialist: Includes all specialties related to surgical care (including obstetrics and gynecology). For a complete listing, see the 2012 Documentation (6).
Other primary care specialist: Includes specialties related to general and family medicine and internal medicine. For a complete listing, see the 2012 Documentation (6).
Data source and methods
Data for this report are from NAMCS, conducted by the National Center for Health Statistics (NCHS). NAMCS is an annual, nationally representative survey of office-based physicians and visits to their offices (6). The target universe of NAMCS is physicians classified as providing direct patient care in office-based practices. Radiologists, anesthesiologists, and pathologists are excluded, as are physicians in community health centers. In 2012, the NAMCS survey design changed, and the sample size was increased five-fold to allow for state-level estimates in the 34 most populous states (6,7). This sampling design change may affect trending NAMCS 2011 data with 2012 data. The sample included 9,574 in-scope physicians (6). The unweighted physician response rate was 58.7% (59.7% weighted). Participating physicians provided 76,330 visit records. The unweighted visit response rate for the 2012 survey was 39.3% (39.4% weighted). A detailed analysis of nonresponse bias was conducted by NCHS. After adjustment for nonresponse by state, census division, metropolitan status, and physician specialty categories, no or negligible biases were observed among physicians providing visit data (7).
Population estimates and standard errors were calculated in Stata/SE 13.1 software (8) to account for the complex sample design. Two-sided statistical tests at the 0.05 level were used to compare estimates and rates, and to test for significance.
About the authors
Sayeedha G. Uddin, Kathleen S. O’Connor, and Jill J. Ashman are with the National Center for Health Statistics, Division of Health Care Statistics.
References
- American Academy of Pediatrics. Recommendations for Preventive Pediatric Health Care. 2016.
- National Committee for Quality Assurance. Healthcare Effectiveness Data and Information Set: Child and adolescent well-care visits.
- NCHS. National Ambulatory Medical Care Survey: 2012 state and national summary tables.
- Freid VM, Makuc DM, Rooks RN. Ambulatory health care visits by children: Principal diagnosis and place of visit. National Center for Health Statistics. Vital Health Stat 13(137). 1998.
- NCHS. Classification of diseases, functioning, and disability. International Classification of Diseases, Ninth Revision, Clinical Modification (ICD–9–CM).
- NCHS. 2012 NAMCS microdata file documentation. Hyattsville, MD. 2015.
- Hing E, Shimizu IM, Talwalkar A. Nonresponse bias in estimates from the 2012 National Ambulatory Medical Care Survey. Vital Health Stat 2(171). 2016.
- StataCorp LP. Stata/SE (Release 13.1 for Windows) [computer software]. Revised December 19, 2014.
Suggested citation
Uddin SG, O’Connor KS, Ashman JJ. Physician office visits by children for well and problem-focused care: United States, 2012. NCHS data brief, no 248. Hyattsville, MD: National Center for Health Statistics. 2016.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Charles J. Rothwell, M.S., M.B.A., Director
Nathaniel Schenker, Ph.D., Deputy Director
Jennifer H. Madans, Ph.D., Associate Director for Science
Division of Health Care Statistics
Clarice Brown, M.S., Director
Alexander Strashny, Ph.D., Associate Director for Science
- Page last reviewed: May 20, 2016
- Page last updated: May 20, 2016
- Content source: