

Cigarette Smoking and Lung Obstruction Among Adults Aged 40–79: United States, 2007–2012
 ShareCompartir
ShareCompartir
On This Page
- Key findings
- What percentage of adults aged 40–79 with and without lung obstruction currently smoked cigarettes?
- Among adults aged 40–79 with lung obstruction, did men and women differ in the percentage who currently smoked cigarettes?
- Did cigarette smoking among adults aged 40–79 with lung obstruction differ by age?
- Did cigarette smoking among adults aged 40–79 with lung obstruction differ by race and Hispanic origin?
- Did cigarette smoking among adults aged 40–79 with lung obstruction differ by education?
- Summary
- Definitions
- Data source and methods
- About the authors
- References
- Suggested citation
NCHS Data Brief No. 181, January 2015
PDF Version (674 KB)
Ryne Paulose-Ram, Ph.D., M.A.; Timothy Tilert, B.S.; Charles F. Dillon, M.D., Ph.D.; and Debra J. Brody, M.P.H.
Key findings
Data from the National Health and Nutrition Examination Survey, 2007–2012
- During 2007–2012, 46.2% of adults aged 40–79 with lung obstruction currently smoked cigarettes. About 41% with mild and 55% with moderate or worse obstruction were current smokers.
- A similar percentage of men and women with lung obstruction, overall and at each level of severity, smoked cigarettes.
- A greater percentage of adults aged 40–59 with lung obstruction, overall and at each level of severity, smoked cigarettes than those aged 60–79.
- Cigarette smoking among adults with lung obstruction varied by race and Hispanic origin and by severity of obstruction.
- The percentage of adults with lung obstruction, overall and at each level of severity, who smoked cigarettes declined with increasing education.
Lung obstruction is characterized by blocked airflow, shortness of breath, and difficulty exhaling. The most common obstructive lung diseases are asthma and chronic obstructive pulmonary disease (COPD), which includes emphysema and chronic bronchitis. Approximately 15% of U.S. adults aged 40–79 have lung obstruction, with about one-third of those having moderate or worse obstruction (1). Smoking tobacco increases respiratory symptoms (2), lung function loss (3), and the rate of lung function decline (4–6). The benefits of smoking cessation are numerous for all adults (6) and especially for those with lung obstruction (5). This report presents national estimates of cigarette smoking among adults with measured lung obstruction for the period 2007–2012.
Keywords: obstructive lung disease, lung impairment, spirometry, COPD.
What percentage of adults aged 40–79 with and without lung obstruction currently smoked cigarettes?
In 2007–2012, approximately 46% of adults aged 40–79 with any lung obstruction were current cigarette smokers. This was more than double the percentage for those without lung obstruction who smoked cigarettes (19.8%) (Figure 1). Among adults with mild lung obstruction, 41.2% were current cigarette smokers, and among those with moderate or worse lung obstruction, more than one-half (55.0%) were current smokers.
Figure 1. Cigarette smoking among adults aged 40–79 with and without lung obstruction: United States, 2007–2012
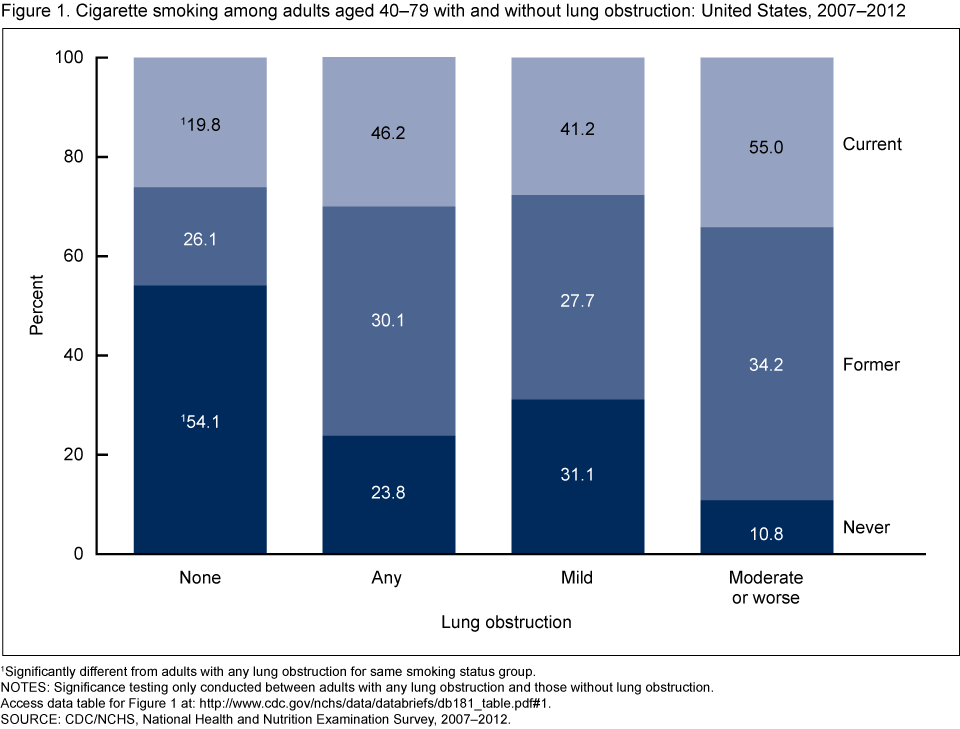
1Significantly different from adults with any lung obstruction for same smoking status group.
NOTES: Significance testing only conducted between adults with any lung obstruction and those without lung obstruction. Access data table for Figure 1
SOURCE: CDC/NCHS, National Health and Nutrition Examination Survey, 2007–2012.
Among adults aged 40–79 with lung obstruction, did men and women differ in the percentage who currently smoked cigarettes?
Among adults aged 40–79 with any lung obstruction, a similar percentage of men (49.3%) and women (42.6%) were current cigarette smokers (Figure 2). Rates of cigarette smoking for men and women also were similar at each level of obstruction severity.
Figure 2. Percentage of adults aged 40–79 with lung obstruction who currently smoked cigarettes, by sex and severity of obstruction: United States, 2007–2012
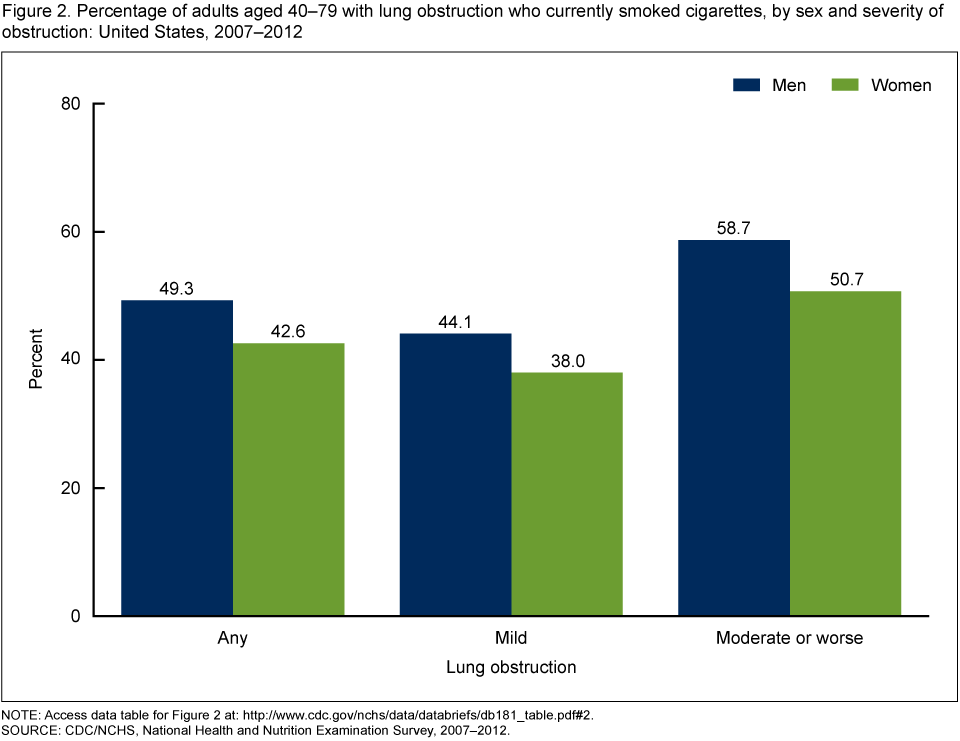
NOTE: Access data table for Figure 2
SOURCE: CDC/NCHS, National Health and Nutrition Examination Survey, 2007–2012.
Did cigarette smoking among adults aged 40–79 with lung obstruction differ by age?
The percentage of adults aged 40–59 with any lung obstruction who currently smoked cigarettes (50.8%) was higher than for those aged 60–79 (38.6%) (Figure 3). This difference by age also was similar for adults at each level of obstruction severity.
Figure 3. Percentage of adults aged 40–79 with lung obstruction who currently smoked cigarettes, by age group and severity of obstruction: United States, 2007–2012
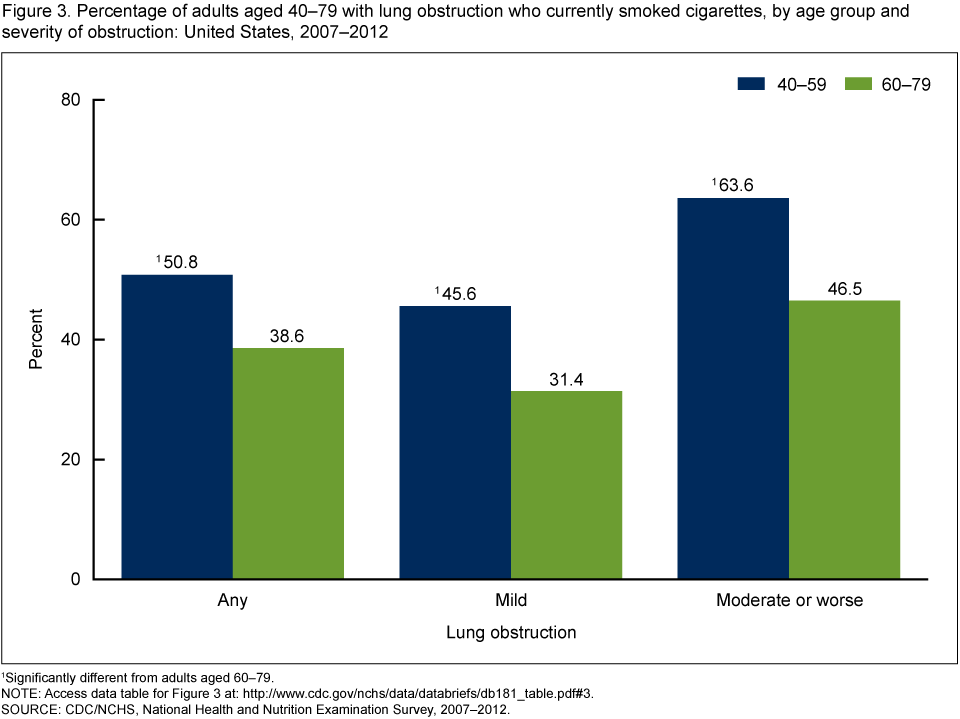
1Significantly different from adults aged 60–79.
NOTE: Access data table for Figure 3
SOURCE: CDC/NCHS, National Health and Nutrition Examination Survey, 2007–2012.
Did cigarette smoking among adults aged 40–79 with lung obstruction differ by race and Hispanic origin?
Current cigarette smoking among adults aged 40–79 with lung obstruction differed by race and Hispanic origin. Among adults with mild lung obstruction, a higher percentage of non-Hispanic black adults were current cigarette smokers (62.6%) than non-Hispanic white (38.2%) or Hispanic (31.9%) adults (Figure 4). For those with moderate or worse lung obstruction, however, a higher percentage of non-Hispanic white adults were current cigarette smokers (61.7%) compared with non-Hispanic black (45.2%) and Hispanic (24.9%) adults.
Figure 4. Age-adjusted percentage of adults aged 40–79 with lung obstruction who currently smoked cigarettes, by race and Hispanic origin and severity of obstruction: United States, 2007–2012
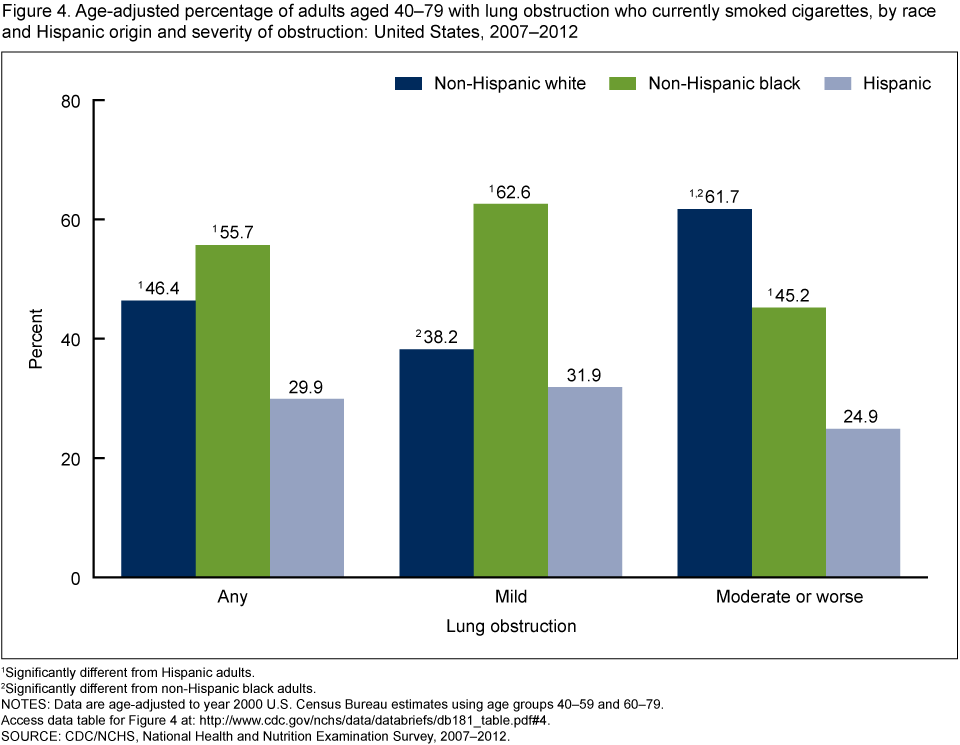
1Significantly different from Hispanic adults.
2Significantly different from non-Hispanic black adults.
NOTES: Data are age-adjusted to year 2000 U.S. Census Bureau estimates using age groups 40–59 and 60–79. Access data table for Figure 4
SOURCE: CDC/NCHS, National Health and Nutrition Examination Survey, 2007–2012.
Did cigarette smoking among adults aged 40–79 with lung obstruction differ by education?
Among adults aged 40–79, overall and at each level of obstruction severity, the percentage of adults who currently smoked declined with increasing levels of education (Figure 5). Of those with any lung obstruction, nearly two out of three adults with less than a high school degree were currently smoking, compared with 53.2% of high school graduates and 36.0% of those with at least some college education. Among adults with mild lung obstruction, almost 55% with less than a high school degree currently smoked cigarettes, whereas among those with moderate or worse lung obstruction, nearly 74% with less than a high school degree were current smokers.
Figure 5. Percentage of adults aged 40–79 with lung obstruction who currently smoked cigarettes, by education and severity of obstruction: United States, 2007–2012
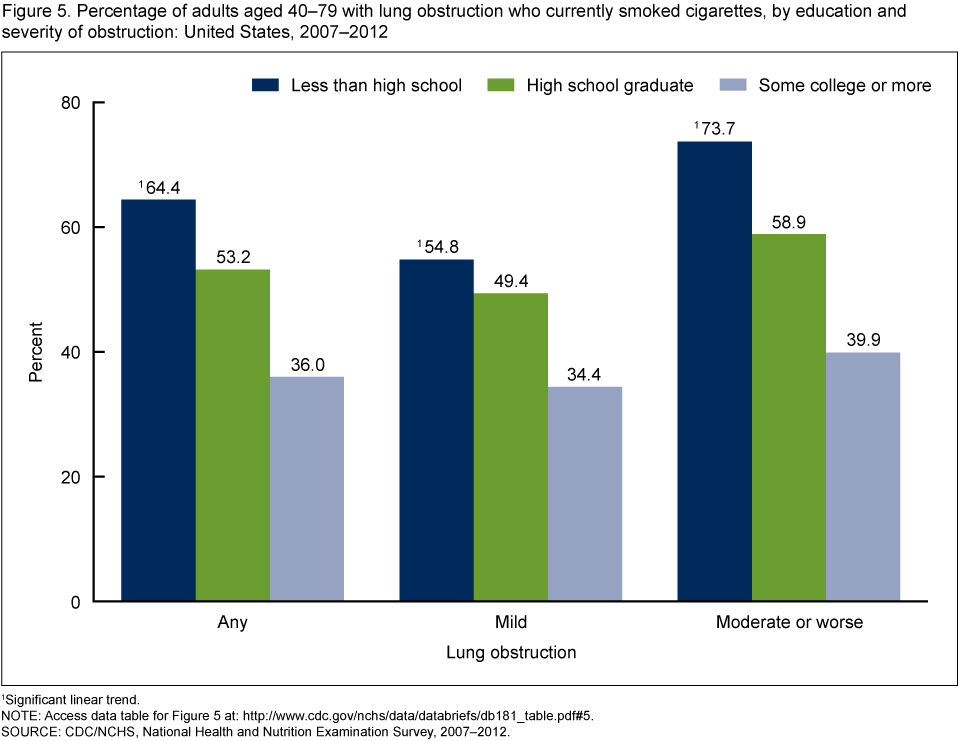
1Significant linear trend.
NOTE: Access data table for Figure 5
SOURCE: CDC/NCHS, National Health and Nutrition Examination Survey, 2007–2012.
Summary
During 2007–2012, about 46% of U.S. adults aged 40–79 with lung obstruction currently smoked cigarettes. This was more than double the smoking rate for those without lung obstruction (19.8%).
In the United States, a greater percentage of men (20.5%) than women (15.3%) were current cigarette smokers in 2013 (7). Some studies (8,9) have suggested that women are more susceptible than men to the effects of tobacco smoke. Since 2000, the number of women dying from COPD has exceeded the number of men dying from the disease (10). In the present report, a similar percentage of men and women overall, and at each level of lung obstruction severity, currently smoked cigarettes.
Notable differences were seen in smoking rates by race and Hispanic origin. Among adults aged 40–79 with mild lung obstruction, a significantly greater percentage of non-Hispanic black adults currently smoked cigarettes compared with the two other race and Hispanic origin groups. With moderate or worse lung obstruction, however, a significantly greater percentage of non-Hispanic white adults currently smoked cigarettes compared with those in the other race and Hispanic origin groups.
Smoking rates among those with lung obstruction also varied by education, with progressively higher rates of smoking among those with decreasing levels of education. This inverse relationship between smoking and education level is consistent across all severity levels of lung obstruction.
Smoking tobacco can increase respiratory symptoms (2), loss of lung function (3), and the progression of COPD (4–6). The data presented here show that during 2007–2012, almost one-half of U.S. adults aged 40–79 with lung obstruction currently smoked cigarettes.
Definitions
Lung obstruction: Based on lung function values obtained from a pre-bronchodilator spirometry examination, lung obstruction was defined as a forced expiratory volume in the first second (FEV1) to forced vital capacity (FVC) ratio less than the lower limit of normal (11). Persons were also defined as having lung obstruction based on a positive response to use of daytime supplemental oxygen and ever having been diagnosed with emphysema or still having chronic bronchitis. As defined here, approximately 14.7% of U.S. adults aged 40–79 had measured lung obstruction in 2007–2012 (1).
Severity of lung obstruction: Mild lung obstruction was defined as an FEV1 greater than 70% predicted among those with lung obstruction. Moderate or worse lung obstruction was defined as an FEV1 less than or equal to 70% predicted among those with lung obstruction (11). Persons who were identified as having lung obstruction based on supplemental oxygen use were defined as having moderate or worse lung obstruction. Applying these definitions, approximately 9.4% of U.S. adults aged 40–79 had mild lung obstruction and 5.3% had moderate or worse lung obstruction in 2007–2012 (1).
Smoking status: A current smoker reported smoking at least 100 cigarettes in his or her lifetime, and at the time of the household interview reported currently smoking every day or some days, or was defined by a measured serum cotinine value greater than 10 ng/mL (12) (cotinine is a metabolite of nicotine that reflects recent exposure). A former smoker reported smoking at least 100 cigarettes during his or her lifetime but currently did not smoke. A never smoker reported smoking fewer than 100 cigarettes during his or her lifetime.
Data source and methods
Data from the National Health and Nutrition Examination Surveys (NHANES) 2007–2012 were used for these analyses. NHANES is a cross-sectional survey designed to monitor the health and nutritional status of the civilian noninstitutionalized resident population of the United States. The survey consists of interviews conducted in participants’ homes and standardized physical examinations conducted in mobile examination centers (MECs), where blood and urine specimens are collected.
The NHANES sample is selected through a complex, multistage probability design. Data collection is based on a representative sample covering all ages of the target population. During 2007–2010, non-Hispanic black and Hispanic persons were oversampled to obtain more reliable estimates of the health of these population subgroups. During 2011–2012, non-Hispanic Asian persons were also oversampled. Public-use data files are released in 2-year cycles.
During NHANES 2007–2012, spirometry data were collected in the MEC from survey participants aged 6–79 years. Details of the NHANES spirometry examination procedures and data collection are available elsewhere (13). Lung obstruction may be defined using multiple criteria. This report uses American Thoracic Society/European Respiratory Society (ATS/ERS) diagnostic criteria and follows the data and analytic methodology used by Tilert et al. (1).
Examination sample weights were used to account for differential probabilities of selection, nonresponse, and noncoverage and were incorporated into the estimation process. Standard errors of the percentages were estimated using Taylor series linearization, a method that incorporates the sample weights and accounts for the complex survey design. Estimates for race and Hispanic origin were age-adjusted by the direct method to the year 2000 projected U.S. standard population using two age groups: 40–59 and 60–79. Differences between groups were tested using Student’s t statistic at the p < 0.05 significance level. To test for linear trends, the null hypothesis of a nonlinear trend was examined using orthogonal polynomials. Statistical analyses were conducted using STATA, version 12.1 (StataCorp, College Station, Tex.).
About the authors
Ryne Paulose-Ram, Timothy Tilert, Charles F. Dillon, and Debra J. Brody are with CDC’s National Center for Health Statistics, Division of Health and Nutrition Examination Surveys.
References
- Tilert T, Paulose-Ram R, Brody DJ. Lung obstruction among adults aged 40–79: United States, 2007–2012. NCHS data brief, no 180. Hyattsville, MD: National Center for Health Statistics. 2014.
- Kanner RE, Connett JE, Williams DE, Buist AS. Effects of randomized assignment to a smoking cessation intervention and changes in smoking habits on respiratory symptoms in smokers with early chronic obstructive pulmonary disease: The Lung Health Study. Am J Med 106(4):410–6. 1999.
- Anthonisen NR, Connett JE, Murray RP. Smoking and lung function of Lung Health Study participants after 11 years. Am J Respir Crit Care Med 166(5):675–9. 2002.
- Anthonisen NR, Connett JE, Kiley JP, Altose MD, Bailey WC, Buist AS, et al. Effects of smoking intervention and the use of an inhaled anticholinergic bronchodilator on the rate of decline of FEV1: The Lung Health Study. JAMA 272(19):1497–505. 1994.
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management, and prevention of COPD (updated 2014). January 2014.
- HHS. The health consequences of smoking—50 years of progress: A report of the Surgeon General. Atlanta, GA: CDC, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health. Printed with corrections, January 2014.
- Schiller JS, Ward BW, Freeman G. Early release of selected estimates based on data from the 2013 National Health Interview Survey. National Center for Health Statistics. June 2014.
- Foreman MG, Zhang L, Murphy J, Hansel NN, Make B, Hokanson JE, et al. Early-onset chronic obstructive pulmonary disease is associated with female sex, maternal factors, and African American race in the COPDGene Study. Am J Respir Crit Care Med 184(4):414–20. 2011.
- Dransfield MT, Davis JJ, Gerald LB, Bailey WC. Racial and gender differences in susceptibility to tobacco smoke among patients with chronic obstructive pulmonary disease. Respir Med 100(6):1110–6. 2006.
- Dance A. Health impact: Breathless. Nature 489(7417):S2–3. 2012.
- Pellegrino R, Viegi G, Brusasco V, Crapo RO, Burgos F, Casaburi R, et al. Interpretative strategies for lung function tests. Eur Respir J 26(5):948–68. 2005.
- Hukkanen J, Jacob P III, Benowitz NL. Metabolism and disposition kinetics of nicotine. Pharmacol Rev 57(1):79–115. 2005.
- NCHS. National Health and Nutrition Examination Survey: Respiratory health spirometry procedures manual. 2011.
Suggested citation
Paulose-Ram R, Tilert T, Dillon CF, Brody DJ. Cigarette smoking and lung obstruction among adults aged 40–79: United States, 2007–2012. NCHS data brief, no 181. Hyattsville, MD: National Center for Health Statistics. 2015.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Charles J. Rothwell, M.S., M.B.A., Director
Jennifer H. Madans, Ph.D., Associate Director for Science
Division of Health and Nutrition Examination Surveys
Kathryn S. Porter, M.D., M.S., Director
- Page last reviewed: November 6, 2015
- Page last updated: January 7, 2015
- Content source: