

Perception of Weight Status in U.S. Children and Adolescents Aged 8–15 Years, 2005–2012
 ShareCompartir
ShareCompartir
On This Page
- Key findings
- Are there differences in weight status misperception between children and adolescents by sex and age?
- Are there differences in weight status misperception among children and adolescents by race and Hispanic origin?
- Are there differences in weight status misperception among children and adolescents by sex and body mass index?
- Are there differences in weight status misperception among children and adolescents by family income-to-poverty ratio (FIPR)?
- Summary
- Definitions
- Data source and methods
- About the authors
- References
- Suggested citation
NCHS Data Brief No. 158, July 2014
PDF Version (636 KB)
Neda Sarafrazi, Ph.D.; Jeffery P. Hughes, M.P.H.; Lori Borrud, Ph.D.; Vicki Burt, Sc.M., R.N.; and
Ryne Paulose-Ram, Ph.D., M.A.
Key findings
Data from the National Health and Nutrition Examination Survey, 2005–2012
- About 30% of children and adolescents aged 8–15 years in the United States misperceive their weight status. Weight status misperception is more common among boys (32.3%) than girls (28.0%).
- About one-third of Mexican-American (34.0%) and non-Hispanic black (34.4%) children and adolescents misperceive their weight status compared with non-Hispanic white children and adolescents (27.7%).
- Approximately 81% of overweight boys and 71% of overweight girls believe they are about the right weight.
- Nearly 48% of obese boys and 36% of obese girls consider themselves to be about the right weight.
Childhood obesity is a major public health problem associated with many adverse health outcomes in adulthood (1). During 2011–2012, nearly 17% of children and adolescents were obese (2). Weight status misperception occurs when the child’s perception of their weight status differs from their actual weight status based on measured height and weight. Accurate weight status self-perception has been linked to appropriate weight control behaviors in youth. The National Health and Nutrition Examination Survey (NHANES) data for children and adolescents aged 8–15 years offers an opportunity to examine weight perception status in this age group.
Keywords: weight perception, youth, overweight, obesity
Are there differences in weight status misperception between children and adolescents by sex and age?
During 2005–2012, 30.2% of children and adolescents misperceived their weight status. Overall, weight status misperception was more common among boys (32.3%) than girls (28.0%).
Figure 1. Weight status misperception among children and adolescents aged 8–15 years, by sex and age: United States, 2005–2012
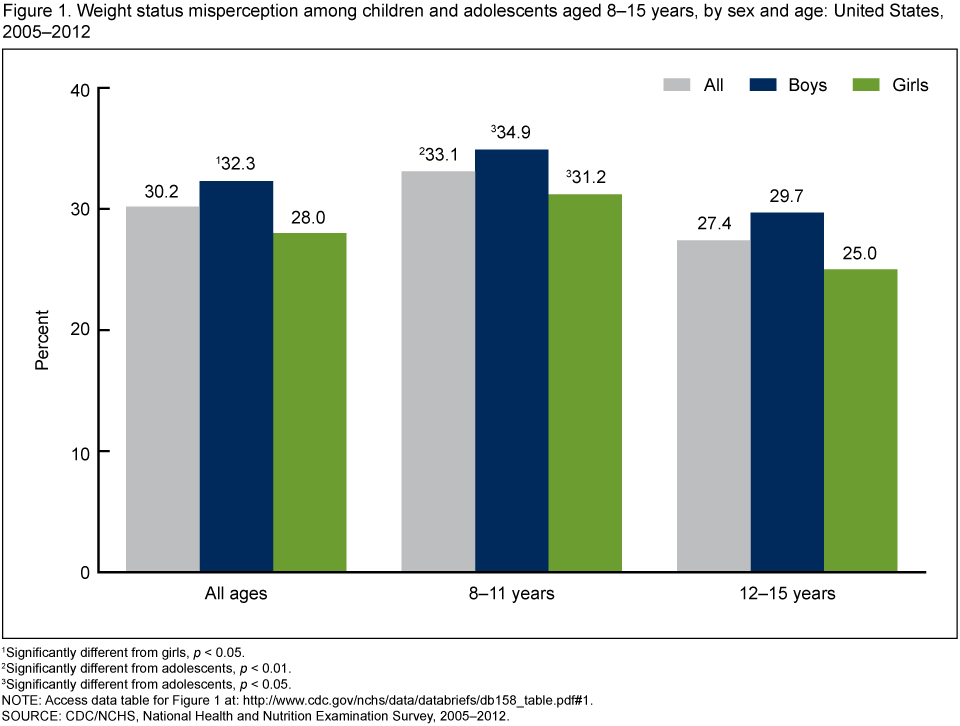
1Significantly different from girls, p < 0.05.
2Significantly different from adolescents, p < 0.01.
3Significantly different from adolescents, p < 0.05.
NOTE: Access data table for Figure 1 [PDF – 136KB].
SOURCE: CDC/NCHS, National Health and Nutrition Examination Survey, 2005–2012.
About 33% of children aged 8–11 years and about 27% of adolescents aged 12–15 years misperceived their weight status. Weight status misperception was significantly higher among children compared with adolescents (p < 0.05). This was true for both boys and girls (Figure 1).
Are there differences in weight status misperception among children and adolescents by race and Hispanic origin?
The prevalence of weight status misperception was lowest among non-Hispanic white (27.7%) children and adolescents compared with non-Hispanic black (34.4%) and Mexican-American (34.0%) children and adolescents. This was true for both boys and girls (p < 0.05) (Figure 2).
Figure 2. Weight status misperception among children and adolescents aged 8–15 years, by race and Hispanic origin: United States, 2005–2012
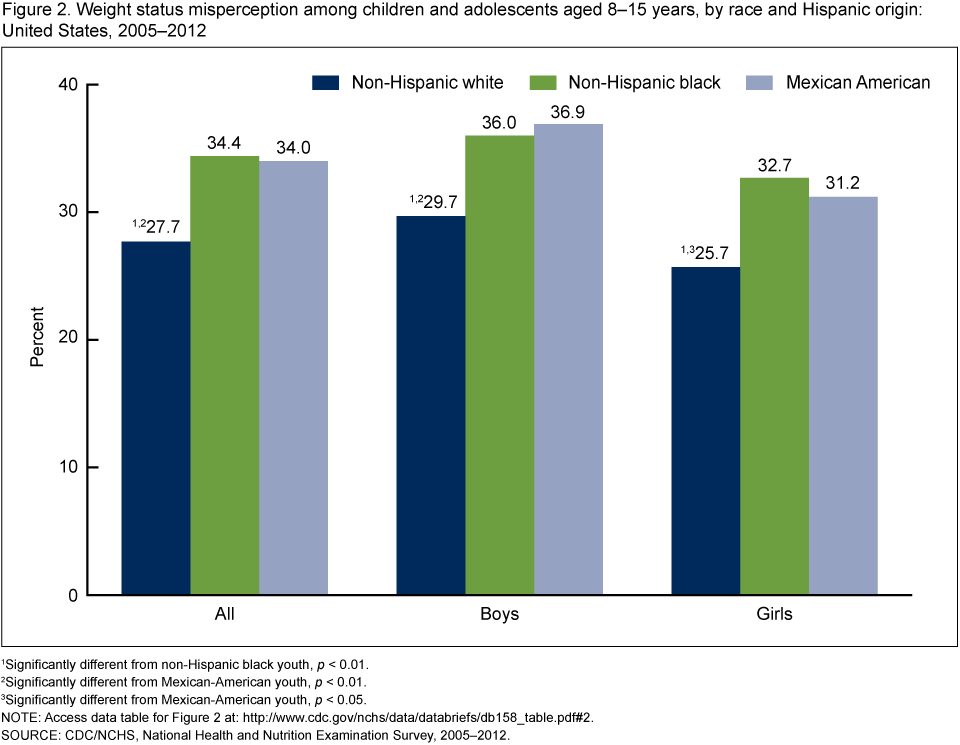
1Significantly different from non-Hispanic black youth, p < 0.01.
2Significantly different from Mexican-American youth, p < 0.01.
3Significantly different from Mexican-American youth, p < 0.05.
NOTE: Access data table for Figure 2 [PDF – 136KB].
SOURCE: CDC/NCHS, National Health and Nutrition Examination Survey, 2005–2012.
Are there differences in weight status misperception among children and adolescents by sex and body mass index?
Weight status misperception varies by body mass index: 87.4% of normal weight youth, 76.0% of overweight youth, and 41.9% of obese youth considered themselves to be about the right weight (Figure 3).
This overall pattern was similar for boys and girls. About 81% of overweight boys and 71% of overweight girls believed that they were about the right weight, and about 48% of obese boys and 36% of obese girls considered themselves to be about the right weight.
Figure 3. Weight status misperception among children and adolescents aged 8–15 years, by sex and body mass index category: United States, 2005–2012
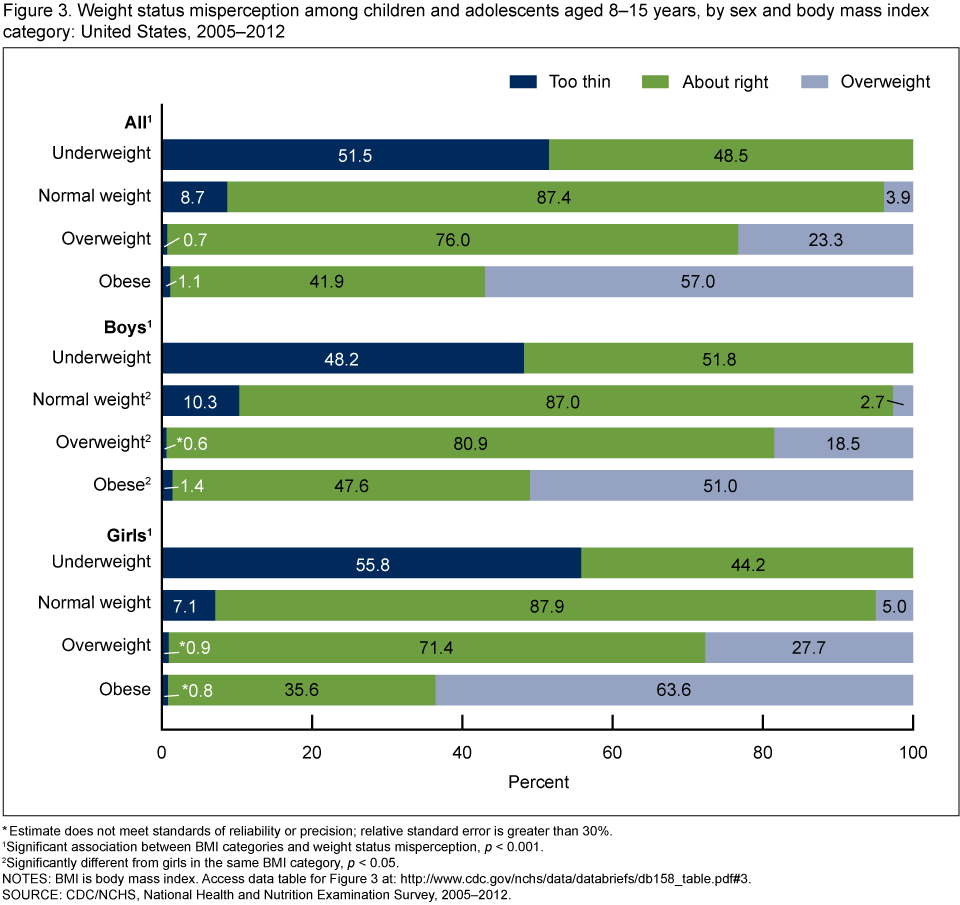
* Estimate does not meet standards of reliability or precision; relative standard error is greater than 30%.
1Significant association between BMI categories and weight status misperception, p < 0.001.
2Significantly different from girls in the same BMI category, p < 0.05.
NOTES: BMI is body mass index. Access data table for Figure 3 [PDF – 136KB].
SOURCE: CDC/NCHS, National Health and Nutrition Examination Survey, 2005–2012.
Are there differences in weight status misperception among children and adolescents by family income-to-poverty ratio (FIPR)?
Overall, the prevalence of weight status misperception was lowest among children and adolescents from higher (350% or more of the FIPR) income (26.3%) families compared with those from middle (130%–349% of the FIPR) income (30.7%) or lower (less than 130% of the FIPR) income (32.5%) families (Figure 4). A similar decreasing trend in weight status misperception with increasing poverty level was seen for girls, but not for boys.
Figure 4. Weight status misperception among boys and girls aged 8–15 years, by family income-to-poverty ratio: United States, 2005–2012
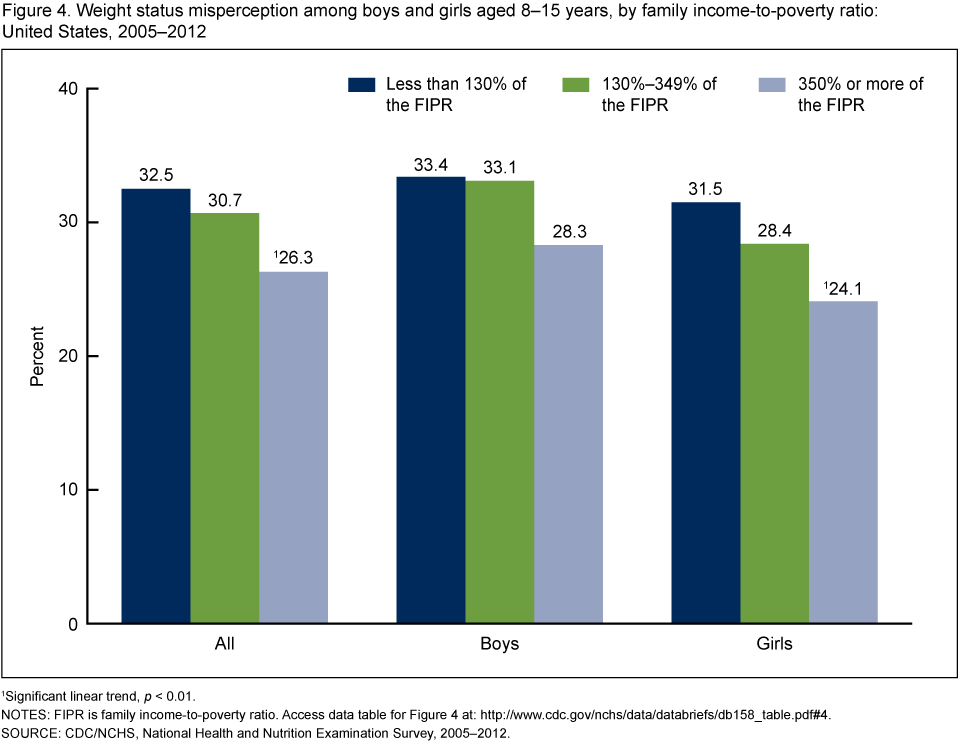
1Significant linear trend, p < 0.01.
NOTES: FIPR is family income-to-poverty ratio. Access data table for Figure 4 [PDF – 136KB].
SOURCE: CDC/NCHS, National Health and Nutrition Examination Survey, 2005–2012.
Summary
During 2005–2012, approximately 30% of children and adolescents aged 8–15 years, corresponding to an estimated 9.1 million children and adolescents in the United States, misperceived their weight status. More than 2 million healthy weight children and adolescents considered themselves to be too thin or too fat. Weight status misperception was more prevalent among overweight boys than girls: Approximately 81% of overweight boys and 71% of overweight girls believed that they were about the right weight.
Weight status misperception varied by sociodemographic characteristics. The prevalence of weight status misperception was higher among boys (32.3%) than girls (28.0%) and lowest among non-Hispanic white (27.7%) children and adolescents compared with non-Hispanic black (34.4%) and Mexican-American (34.0%) children and adolescents. There were also significant differences by income level among boys and girls, with weight misperception significantly less among higher-income families compared with lower-income families.
Accurate self-perception of weight status has been linked to appropriate weight control behaviors in youth. Understanding the prevalence of weight status misperception among U.S. children and adolescents may help inform public health interventions.
Definitions
Underweight: Children and adolescents with age- and sex-specific body mass index (BMI) less than the 5th percentile of the 2000 CDC growth chart were considered underweight (3). BMI was calculated as weight in kilograms divided by height in meters squared, rounded to one decimal place.
Normal weight: Children and adolescents with age- and sex-specific BMI greater than or equal to the 5th and less than the 85th percentile of the 2000 CDC growth chart were considered normal weight (3).
Overweight: Children and adolescents with age- and sex-specific BMI greater than or equal to the 85th and less than the 95th percentile of the 2000 CDC growth chart were considered overweight (3).
Obese: Children and adolescents with age- and sex-specific BMI greater than or equal to the 95th percentile of the 2000 CDC growth chart were considered obese
(3).
Self-perceived weight status: Children were asked the following question by trained interviewers at the NHANES mobile examination center: “Do you consider yourself now to be fat or overweight, too thin, or about the right weight?”
Weight status misperception: Underweight individuals who considered themselves to be “about the right weight” or “overweight” were classified as having a weight status misperception. Normal weight individuals who considered themselves to be “overweight” or “underweight” were classified as having a weight status misperception. Overweight or obese individuals who considered themselves to be “underweight” or “about the right weight” were classified as having a weight status misperception.
Family income-to-poverty ratio: Calculated by dividing family income by a poverty measure specific for family size. The U.S. Department of Health and Human Services’ poverty guidelines were used as the poverty measure to calculate FIPR (4). FIPR accounts for inflation. Income eligibility for participation in the Supplemental Nutrition Assistance Program or SNAP is 130% of the FIPR (< 130% FIPR) (5). Larger FIPRs indicate greater income.
Data source and methods
Data from NHANES were used for these analyses. NHANES is a cross-sectional survey designed to assess the health and nutritional status of the civilian noninstitutionalized U.S. population (6). The survey consists of in-home interviews and standardized physical examinations in mobile examination centers.
The NHANES sample is selected through a complex, multistage design that includes selection of primary sampling units (counties), household segments within the counties, households within the segments, and sample persons from selected households. The sample design includes oversampling to obtain reliable estimates of health and nutritional measures for population subgroups. In 1999, NHANES became a continuous survey. Public-use data files are released in 2-year cycles.
Survey examination weights, which account for the differential probabilities of selection, nonresponse, and noncoverage, were incorporated into the estimation process. The standard errors of the percentages were estimated using Taylor series linearization, a method that incorporates the sample weights and sample design. Differences between groups were evaluated using a Wald chi-square or two-tailed t test, as appropriate, with a p less than 0.05 significance level. Statistical analyses were conducted using SAS version 9.3 (SAS Institute Inc., Cary, N.C.) and SUDAAN version 10.0.1 (RTI International, Research Triangle Park, N.C.).
About the authors
Neda Sarafrazi, Jeffery P. Hughes, Lori Borrud, Vicki Burt, and Ryne Paulose-Ram are with CDC’s National Center for Health Statistics, Division of Health and Nutrition Examination Surveys.
References
- Freedman DS, Mei Z, Srinivasan SR, Berenson GS, Dietz WH. Cardiovascular risk factors and excess adiposity among overweight children and adolescents: The Bogalusa Heart Study. J Pediatr 150(1):12–17.e2. 2007.
- Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of childhood and adult obesity in the United States, 2011–2012. JAMA 311(8):806–14. 2014.
- Kuczmarski RJ, Ogden CL, Guo SS, et al. 2000 CDC growth charts for the United States: Methods and development. National Center for Health Statistics. Vital Health Stat 11(246). 2002.
- U.S. Department of Health and Human Services. Poverty guidelines, research, and measurement. 2012.
- U.S. Department of Agriculture. Supplemental Nutrition Assistance Program (SNAP): Eligibility.
- National Center for Health Statistics. 2011–2012 National Health and Nutrition Examination Survey.
Suggested citation
Sarafrazi N, Hughes JP, Borrud L, et al. Perception of weight status in U.S. children and adolescents aged 8–15 years, 2005–2012. NCHS data brief, no 158. Hyattsville, MD: National Center for Health Statistics. 2014.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Charles J. Rothwell, M.S., M.B.A., Director
Jennifer H. Madans, Ph.D., Associate Director for Science
Division of Health and Nutrition Examination Surveys
Kathryn S. Porter, M.D., M.S., Director
- Page last reviewed: November 6, 2015
- Page last updated: July 23, 2014
- Content source: