

Overview
 ShareCompartir
ShareCompartir
Introduction
The CASPER methodology is modeled after the World Health Organization’s (WHO’s) Expanded Program on Immunization (EPI) adaptation of traditional epidemiologic techniques in the 1970s to identify needs and estimate immunization status of communities in developing countries1. The modified cluster sampling methodology used for CASPER involves two-stages (30 clusters selected probability proportional to size and seven households interviewed within each cluster) and provides estimates for the population2. In 2009, the Centers for Disease Control and Prevention (CDC) developed the CASPER Toolkit [PDF - 2.56 MB] to standardize the assessment methodology and provide a CASPER guidance document for public health practitioners and emergency management officials. The CASPER Toolkit provides guidelines on questionnaire development, methodology, sample selection, training, data collection, analysis, and report writing to assist personnel from any local, state, regional, tribal, or federal public health departments in conducting CASPER. The goal of this website is to supplement the CASPER toolkit by providing a summary of CASPER as well as additional information.
What is in the CASPER toolkit?
The CASPER toolkit offers guidelines on the four major phases of CASPER: preparing for the CASPER, conducting the CASPER, analyzing the data, and writing the report. It is intended to assist those in conducting a CASPER by providing a standardized, step-by-step guide and includes forms, standard questions, and examples necessary to conduct a successful CASPER. You may download the most recent version of the CASPER toolkit [PDF - 2.56 MB].
Why is this information important? What is the benefit of CASPER?
Disasters are a serious disruption of the functioning of society causing widespread human, material, or environmental losses that exceeds the local capacity to respond and calls for external assistance3. The United States is facing an increase in frequency and magnitude of disasters 4; many of which are responsible for negative impacts. Information is key during a disaster response; information sent to the right people, at the right place, at the right time, is an optimal weapon for any successful response5. CASPER seeks to address this issue by providing valid information rapidly about the general and health needs of a community to decision-makers. CASPER is generalizable (providing population estimates), timely, relatively low cost, reported in a simple format, and flexible.
During a disaster response, CASPER provides situational awareness about the community to decision-makers. It can confirm (or contradict) rumors or anecdotal reports, identify immediate needs in the community (e.g., food, water, medication), provide estimates on the scope and magnitude of the needs, and help establish priorities. Other potential benefits include the following:
- Local officials may use the results to strengthen relief efforts, such as management of resources
- Monitor changes in community needs
- Reassure residents that they are not being forgotten
- Raise visibility of emergency management and public health in the community
- Justify requests for outside assistance or funding
- Evaluate the effectiveness of response activities
CASPER is also beneficial in non-disaster situations. It can be used during the preparedness phase to provide situational awareness on how the community is preparing for a disaster (such as estimates on the number of households with an emergency plan or kit) and strengthen planning efforts. CASPER can determine current health status; assess public health perceptions; estimate community awareness, opinions, and concerns regarding the impact of a new project (e.g., transportation route, new power plant); and be used as part of the community assessment requirements for certain grants and accreditations.
CASPER data has been impactful in the past from resource allocation and support for funding of projects or services to targeting messages and future planning. To learn more about previous CASPERs, view the Interactive map of CASPERs or the Past CASPERs section.
What are some considerations prior to conducting a CASPER?
Prior to conducting a CASPER, you should decide if CASPER provides an appropriate sampling methodology on the basis of the objectives, timeframe, and available resources. The preferred sampling methodology for CASPER is the two-stage cluster sampling design in which 30 clusters are selected proportional to the number of households in the cluster and then 7 households are selected systematically for interviews for in each of the 30 clusters. A clear understanding of how the CASPER information will be used, who the relevant stakeholders are, other information obtained in the area, and needed and available resources is important prior to moving forward with your CASPER. For more information, please see CASPER toolkit, Section 2.3 [PDF] or contact the Health Studies Branch.
How do I get started?
If you are interested in conducting a CASPER the CDC Health Studies Branch (HSB) provides scientific consultation, technical assistance, and disaster epidemiology training to
- local, state, regional, tribal, territorial, or foreign health departments,
- federal agencies,
- non-governmental organizations,
- professional interest groups,
- international organizations,
- academic institutions, and
- foreign governments.
To learn more about requesting HSB assistance, please visit HSB’s Disaster Training and Response webpage. Additionally, if you would like more you can check out the CASPER Online Learning Tool for an overview of the CASPER methodology, its uses, and the local capabilities required to conduct a CASPER.
CASPER Phases
There are four phases in a CASPER: preparing for the CASPER, conducting the CASPER in the field, analyzing the data, and writing the report.
Prepare for the CASPER
Prior to conducting a CASPER, you should decide if CASPER provides an appropriate sampling methodology on the basis of the objectives, timeframe, and available resources. One must consider the stakeholders, what forms and approvals are necessary, and who will be the lead of the questionnaire development, organizing interview teams, analyzing data, and writing the report.
Every CASPER will have different objectives. However, clear objectives are essential in determining the sampling frame and focusing the questionnaire. Once your objectives have been defined, the sampling frame – that is, the population from which the sample is drawn – must be identified. Remember, at the completion of the CASPER, the results will be descriptive of the entire chosen sampling frame. For more information on defining the sampling frame and the CASPER methodology, please click HERE.
The final step for preparing a CASPER is to develop the data collection forms and materials. There are four standard data collection forms: the consent script, the questionnaire, the tracking form, and the confidential referral form. Verbal consent is sufficient for CASPER. Your consent script should follow your local IRB guidance. When developing the questionnaire, determine the scope and nature of the questions and identify the critical information needed based on your objectives. This will help keep you questionnaire short (1-2 pages), ideally limiting the interview to 15 minutes. Remember that all questions will be asked at the household level! For examples of questionnaires and sample questions, please click HERE. Once you have developed your forms and questionnaire, conduct a mock interview (e.g., with coworkers) to identify any potential issues and estimate the length of time it will take to complete the interview. The final step is to develop the questionnaire database. We recommend using EpiInfo 7.
For more information, please see CASPER Toolkit, Section 3 [PDF]. For tips on developing a questionnaire database in EpiInfo 7, please click HERE.
Conducting the CASPER in the field
CASPER is conducted via face-to-face interviews in the field. Advantages of this method include a higher response rate, increase your organizations visibility, and distribute health information or other material (such as resource lists) to the community. It is advisable to let the local police department and media know that you will be conducting the CASPER in the community. This increases safety for the teams and also may increase the likelihood of the community members opening the door. Click here for examples of press releases from past CASPERs.
A Just-In-Time training should be conducted for the interview team members either one day in advance or the morning of the first day of the CASPER. This is one of the most important aspects of conducting a CASPER and is essential to its success as inaccurately collecting or reporting data can jeopardize the results and misrepresent the prevalence of injuries or illnesses and the extent of resources needed in the community. Training should provide the interview team members with an understanding of the objectives and method of CASPER, the roles and responsibilities of team members, safety instructions, interview tips, and briefing on logistics such as meeting times. Special attention should be paid to selecting households to interview. We advise systematic sampling. Click HERE for a sample agenda of a Just-In-Time training [PDF].
Once teams are trained, they can head into the field to conduct the CASPER. Always keeping in mind their safety while adhering the methodology, being respectful to the community and each other, and understanding their personal limitations. The interview teams are responsible for the validity, data quality, representativeness, and timeliness of the CASPER so encourage them to ask questions prior to going into the field to conduct the interviews.
For more information, please see CASPER Toolkit, Section 4 [PDF].
Analyzing the data
We recommend using EpiInfo 7 for questionnaire data entry and analysis; however, any statistical software package that allows for weighting data is acceptable. CASPER uses a two-stage sampling design to first select 30 clusters with probability proportional to the number of households in the cluster (first stage) and then 7 households are selected at random from within their cluster (second stage). Population estimates can then be inferred by calculating a sampling weight for each cluster by adding a weight variable to each surveyed household by using the following formula:

The numerator is therefore the total number of households in the selected sampling frame and will be the same for every assessed household. The denominator will potentially differ for each assessed household. If sampling has been 100% successful and interviews were completed in seven households for all 30 clusters, the denominator would be 210 (i.e., 7 * 30). Likely, obtaining seven interviews in each cluster will not be possible and, therefore, the denominator will differ for each household depending on the cluster which the household was selected. Households from the same cluster will have the same weight, but weights will differ between clusters.
Once weights are assigned, weighted frequencies, percents, and 95% confidence intervals can be calculated for each of the interview questions. Applying weights provides projected estimates that can be generalized to every household in the sampling frame. For a tutorial on frequencies, percents, and 95% confidence intervals in EpiInfo, please click here. Remember that weighted analysis does not account for the changes that may occur in the number of households between the time of the census and the time of the CASPER. Therefore, despite attempts to present unbiased estimates, the frequencies reported might lack precision.
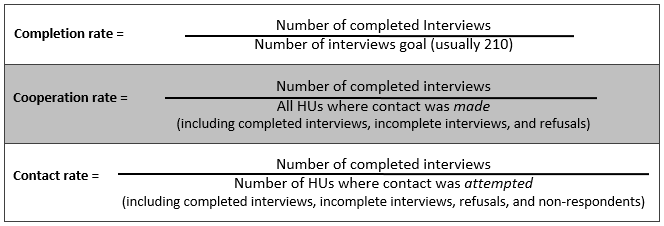
Data from the tracking form should be entered in a spreadsheet for calculation of the contact, cooperation, and completion response rates. These response rates help determine the representativeness of the sample to the population within the sampling frame. The contact rate (the percentage of households that complete an interview after contact is attempted), indicates the representativeness of the sample to the population, with lower rates indicating that the field teams had to attempt interviews at many households to obtain the results. The cooperation rate (the percentage of households that complete an interview after contact has been made), represents both the eligibility and willingness of the community to complete the CASPER interview. And the completion rate (the percentage of completed interviews compared to the ideal number of completed interviews), represents how close interview teams came to collecting the goal of 210. A completion rate below 80% (n=168) represents an unacceptably low number to represent the sampling frame. To compile the tracking form data, tally the responses to each row on the tracking form based on the final designation of the household (e.g., if both “no answer” and “door was answered” for a single household was selected since the interviewer had to return to the household, the final designation of “door was answered” would be entered into the spreadsheet). Below are the formulas for the three response rates:
For more information, please see CASPER Toolkit, Section 5 [PDF].
Writing the report
The final phase of CASPER is writing the report. This is an important phase because it is the delivery of the information collected from the CASPER. Several aspects of the report can be completed during the preparation phase of the CASPER—deciding who will write the report, gathering background information for the report, and creating table shells. Completing such aspects early will ensure a more timely report and enable the CASPER team to deliver a preliminary report within 36 hours of data collection. It is advisable that two reports be developed: (1) a preliminary report or presentation provided to key stakeholders within a day or two after data collection, and (2) a final report that may be more widely distributed at a later time. Consideration should be given to the best way to present the results (e.g., oral presentation) for the preliminary report in a timely matter. This is a good opportunity to discuss implementation of the recommendations, next steps, and lessons learned.
For more information, please see CASPER Toolkit, Section 6 [PDF].
Remember that HSB is available for technical assistance and support throughout all phases of a CASPER.
Footnotes
1 Henderson RH, Sundaresan T. Cluster sampling to assess immunization coverage: a review of experience with a simplified sampling method. Bull World Health Organ. 1982 60(2):253-60.
2 Malilay J, Flannders WD, Brogan D. A modified cluster-sampling method for post-disaster rapid assessment of needs. Bulletin of the World Health Organization. 1996 74(4):399-405.
3 The United Nation Office for Disaster Risk Reduction (UNISDR). Terminology: Disaster. Available at https://www.unisdr.org/we/inform/terminology#letter-d
4 FEMA Disaster Declarations. Available at https://www.fema.gov/disasters
5 United States Congress. A failure of initiative: Final report of the select bipartisan committee to investigate the preparation for and response to Hurricane Katrina. Available at https://www.gpo.gov/fdsys/pkg/CRPT-109hrpt377/pdf/CRPT-109hrpt377.pdf [PDF - 29 MB]
- Page last reviewed: February 17, 2016
- Page last updated: February 17, 2016
- Content source: