


MD STARnet Data and Statistics
 ShareCompartir
ShareCompartir
The following data and statistics come from MD STARnet. Data from the MD STARnet sites cannot be generalized to the entire United States.
Prevalence and Survival
- The estimated prevalence of Duchenne and Becker muscular dystrophy (DBMD) was 1 in every 7,250 males aged 5 – 24 years.1
- The prevalence of DBMD among Non-Hispanic blacks was lower than the prevalence among Hispanics and Non-Hispanic whites.1
- The prevalence of Duchenne muscular dystrophy (DMD) was three times higher than the prevalence of Becker muscular dystrophy (BMD).1
Steroid Use
- Males with DBMD began treatment with steroids at an average age of 7 years.3
- Between about half and two-thirds of males (57% to 69%) with DBMD were treated with steroids.3
[Read Scientific Summary of the Article]
- Of males with DMD who were treated with steroids,
- About 6 in 10 (64%) took prednisone,
- About 2 in 10 (22%) took deflazacort, and
- About 1 in 10 (14%) took both prednisone and deflazacort at different times.4
- On average, males with DMD who had not taken steroids stopped walking at about age 10 years.4
- On average, males with DMD who took steroids for less than 3 years stopped walking at about age 9½ years.4
- On average, males with DMD who took steroids for more than 5 years stopped walking at about age 12 years.4
- Hispanic and non-Hispanic black males with DMD started steroid treatment less often than non-Hispanic white males.5
- Non-Hispanic black males with DMD started steroid treatment an average of one year later than non-Hispanic white males with DMD.5
- Families with a known history of DMD were less likely to choose steroid treatment than families without a history of DMD.5
Diagnosis
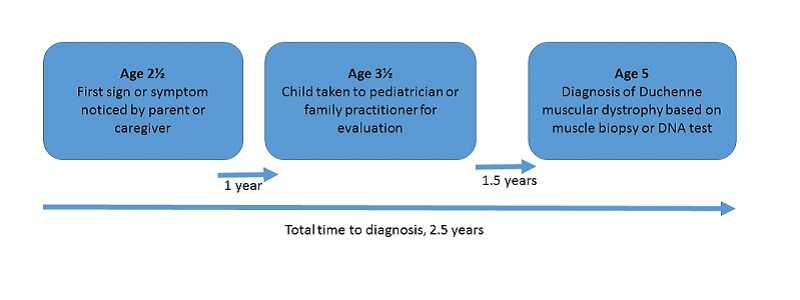
Among males with DMD who did not have a family history of muscular dystrophy:
- There was an average of 2½ years between when a parent or caregiver noticed the first signs and symptoms of DMD, and when a diagnosis of DMD was made based on a muscle biopsy or a DNA test.6
- The average age at diagnosis for DMD was 5 years.6
[Read Scientific Summary of the Article]
- On average, non-Hispanic black or Hispanic children were tested for DBMD at later ages than non-Hispanic white children.7
- On average, children non-Hispanic black or Hispanic children had creatine kinase (CK) testing about 1 year later and DNA testing about 2 years later than non-Hispanic white children.7
Wheelchair Use
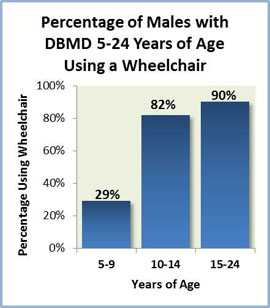
The proportion of males with DBMD who used a wheelchair varied by age:
Mental Health
- Just over 4 in 10 (45%) of the oldest males with DBMD in each family had one of three mental health concerns: behavioral concerns, depressed mood, or attention-deficit/hyperactivity disorder (ADHD).8
- Males with DBMD who took steroids were more than twice as likely to have behavioral concerns compared with their peers who did not take steroids.8
Basic Data
How we got these numbers:
- The tables below show data on males with Duchenne or Becker muscular dystrophy in five MD STARnet sites during the years 1982-2011. Incomplete records may cause the totals in each table to differ. Where there were fewer than 10 patients, the exact number of patients is withheld to protect patient confidentiality.
- These numbers represent males identified with definite or probable Duchenne or Becker muscular dystrophy, based on a rigorous set of criteria. This criteria are described in detail in Table 1 within the MD STARnet case definitions publication.
- Classifying someone as having Duchenne or Becker muscular dystrophy is based on when symptoms first appear, genetic testing results, muscle biopsy results, when an individual stopped walking, and steroid use. Those who could not be classified as having definite or probable Duchenne or Becker muscular dystrophy were excluded.
Type of Muscular Dystrophy
| Type | Arizona | Colorado | Georgia | Iowa | Western New York 12 counties |
Total |
|---|---|---|---|---|---|---|
| Duchenne | 183 | 172 | 193 | 100 | 87 | 735 |
| Becker | 19 | 18 | 35 | 16 | 18 | 106 |
Type of Mutation*
| Type | Arizona | Colorado | Georgia | Iowa | Western New York 12 counties |
Total |
|---|---|---|---|---|---|---|
| Deletion | 121 | 105 | 130 | 64 | 54 | 474 |
| Point Mutation | 19 | 39 | 21 | 23 | 15 | 117 |
| Duplication | 22 | 14 | 18 | 12 | <10 | ** |
* The type of mutation is based on genetic testing results when available in the medical record.
** The total is not reported to protect the confidentiality of patients in Western New York.
Medicaid Status by Age
| Status | Arizona | Colorado | Georgia | Iowa | Western New York 12 counties |
Total |
|---|---|---|---|---|---|---|
| Medicaid (under age 18 years) | 61 | 45 | 83 | 37 | 19 | 245 |
| Medicaid (18 years and above) | 33 | 42 | 29 | 28 | 19 | 151 |
| No Medicaid (under age 18 years) | 36 | 44 | 47 | 21 | 26 | 174 |
| No Medicaid (18 years and above) | <10 | <10 | 12 | <10 | 11 | 40 |
Age group is based on the person’s age at the last available insurance record between 2009 and 2012. Medicaid coverage is indicated by any listing of Medicaid or Children’s Health Insurance Program (CHIP) insurance in the medical record.
Age in Years (as of 12/31/2011) in All MD STARnet Sites
| Less Than 5 | 33 |
|---|---|
| 5-12 | 184 |
| 12-18 | 217 |
| 18 or more | 262 |
Race/Ethnicity in All MD STARnet Sites
| Non-Hispanic White | 501 |
|---|---|
| Non-Hispanic Black | 55 |
| Hispanic | 175 |
| Other* | 110 |
*The term “other” includes Asian, Hawaiian or other Pacific Islander, Native American, American Indian or Alaska Native, and multiracial classifications. Males without race/ethnicity information in the medical record are included in the “other” category.
For more information on MD STARnet see Research and Tracking.
References
- Romitti PA, Zhu Y, Puzhankara S, James KA, Nabukera SK, Zamba GK, Ciafaloni E, Cunniff C, Druschel CM, Mathews KD, Matthews DJ, Meaney FJ, Andrews JG, Conway KM, Fox DJ, Street N, Adams MM, Bolen J; MD STARnet. Prevalence of Duchenne and Becker muscular dystrophies in the United States. Pediatrics. 2015 Mar;135(3):513-21.
- Centers for Disease Control and Prevention (CDC). Prevalence of Duchenne/Becker muscular dystrophy among males aged 5-24 years – four states, 2007. MMWR Morb Mortal Wkly Rep. 2009 Oct 16;58(40):1119-22.
- Barber BJ, Andrews JG, Lu Z, West NA, Meaney FJ, Price ET, Gray A, Sheehan DW, Pandya S, Yang M, Cunniff C. Oral corticosteroids and onset of cardiomyopathy in Duchenne muscular dystrophy. J Pediatr. 2013 Oct;163(4):1080-4.e1.
- Kim S, Campbell KA, Fox DJ, Matthews DJ, Valdez R; MD STARnet. Corticosteroid treatments in males with Duchenne muscular dystrophy: Treatment duration and time to loss of ambulation. J Child Neurol. 2015 Sept;30(10):1275-80.
- Fox DJ, Kumar A, West N, DiRienzo AG, James KA, Oleszek J; Muscular Dystrophy Surveillance, Tracking, and Research Network (MD STARnet). Trends with corticosteroid use in males with Duchenne muscular dystrophy born 1982-2001. J Child Neurol. 2015 Jan;30(1):21-6.
- Ciafaloni E, Fox DJ, Pandya S, Westfield CP, Puzhankara S, Romitti PA, Mathews KD, Miller TM, Matthews DJ, Miller LA, Cunniff C, Druschel CM, Moxley RT. Delayed diagnosis in Duchenne muscular dystrophy: data from the Muscular Dystrophy Surveillance, Tracking, and Research Network (MD STARnet). J Pediatr. 2009 Sept;155(3):380-5.
- Holtzer C, Meany FJ, Andrews J, Ciafaloni E, Fox DJ, James KA, Lu Z, Miller L, Pandya S, Ouyang L, Cunniff C. Disparities in the diagnostic process of Duchenne and Becker muscular dystrophy. Genet Med. 2011 Nov;13(11):942-947.
- Caspers Conway K, Mathews KD, Paramsothy P, Oleszek J, Trout C, Zhang Y, Romitti PA; MD STARnet. Neurobehavioral concerns among males with dystrophinopathy using population-based surveillance data from the Muscular Dystrophy Surveillance, Tracking, and Research Network. J Dev Behav Pediatr. 2015 Jul-Aug;36(6):455-63.
- Page last reviewed: January 13, 2017
- Page last updated: July 19, 2016
- Content source: