

Goals & Strategy for Development of a Comprehensive Waterborne Burden Disease Estimate
 ShareCompartir
ShareCompartir
The goal of developing a waterborne disease burden estimate is to provide a measure of illness, hospitalizations, deaths, and healthcare costs associated with waterborne diseases and syndromes in the U.S., considering all types of water exposures and disease outcomes.
Looking at All Waterborne Diseases
Waterborne diseases can affect a variety of body systems, and there is a need to develop an estimate that includes all types of waterborne disease, not just acute gastrointestinal illness (AGI, includes vomiting and diarrhea).
Waterborne diseases can cause more than gastrointestinal illnesses. There is a whole spectrum of illnesses that can be spread through water, including ear, eye, skin, respiratory, and wound infections. Waterborne diseases and syndromes can affect multiple body systems and overall physical health.
Attributing Illnesses to Sources
Many pathogens that cause waterborne disease can also be transmitted by other sources, such as through contaminated foods or contact with infected animals or people. It is important that a waterborne disease burden estimate be consistent with all possible sources of illness.
The process of estimating the specific source responsible for illness is called attribution. The attribution process will result in an estimate of what percentage of illness is due to each possible source (food, water, infected animals and people, or other sources.) This percentage may vary for each pathogen since some pathogens are primarily spread by water and others are only partially spread by water. For example, Salmonella is more likely to be spread by contaminated food, while some amebae, such as Naegleria fowleri, are primarily spread through water.
Once an illness is attributed to a water exposure, a secondary aim is to determine the source of the water exposure. This is challenging because a person may be exposed to numerous water sources in a short time period (for example, it is likely for a person to be exposed to drinking and environmental water sources in the same day.)
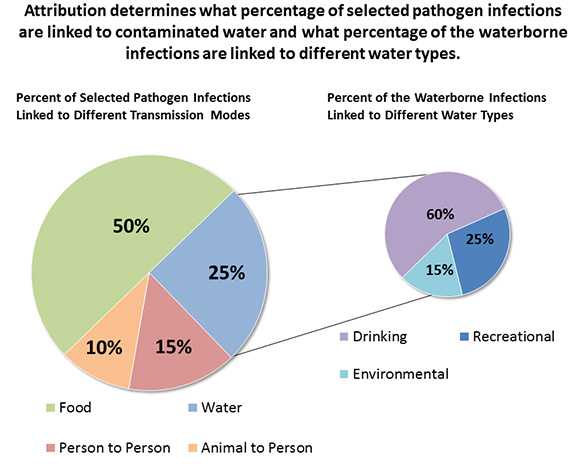
These figures show the type of information attribution will illustrate. They are an example and do not come from existing data.
It is often difficult to determine the specific water source responsible for the illness, or whether water is responsible at all. Not everyone who is exposed to a waterborne pathogen will become sick, and people usually do not know what made them sick. Ongoing studies and partnerships with other researchers will likely be needed to help expand and improve the analytical methods and evidence base.
Strategy for Developing a Waterborne Disease Burden Estimate
Take advantage of large, publicly available databases
Death certificates, administrative (insurance claims) databases, and nationally representative surveys of health care providers are useful for estimating waterborne disease because these sources provide large, nationally representative samples. Since these data sources are based on national insurance claims and health care provider records, the illness estimates can approximate the U.S. population without being adjusted to account for individuals that are not detected or diagnosed. Multiple pathogens can be compared using a single data source, and the different data sources can be compared to each other to verify results and account for the limitations of each data source. Some of these data sources also provide information on patient characteristics, which can be used to determine which populations are more vulnerable to waterborne disease.
CDC's Waterborne Disease Outbreak Surveillance System (WBDOSS) is a helpful tool for monitoring illness trends, determining exposure routes and risk factors, and planning for interventions. However, since not all outbreaks are recognized, investigated, or reported, and there is no way to know how many outbreaks go undetected, this data source cannot be used to estimate the amount of waterborne illness in the U.S.
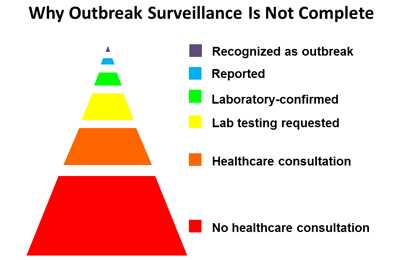
The outbreak surveillance pyramid illustrates why outbreak surveillance data does not include all waterborne disease. Most people do not seek health care for their illnesses, and even among individuals who seek care, many do not have any laboratory testing. Laboratory testing does not always identify a pathogen, and even when a specific pathogen is identified, physicians may not report all illnesses to public health departments. Further, it may not be evident that patients are connected to a common exposure, so many outbreaks go undetected and unreported.
In addition to systematic challenges with outbreak reporting, these data do not measure sporadic (infections not linked to an outbreak) cases of waterborne illness, which provide an important contribution to the burden of waterborne illness in the U.S.
Focus on a subset of pathogens and diagnoses with the best data
The waterborne disease burden estimate will focus on partially and primarily waterborne pathogens that are 1) largely driving waterborne illness in the U.S. and 2) likely to be reported to a healthcare professional. Pathogen selection was informed by previous studies and national outbreak data.
The following pathogens will be used to estimate the burden of waterborne disease in the U.S. Some of these pathogens are more likely to be transmitted by water (for example, Naegleria fowleri or Legionella) than others (for example, Salmonella or E. coli.) The attribution process will determine the percentage of pathogen infections that are due to contaminated water.
Partial pathogen list for burden estimate:
- Cryptosporidium
- Giardia
- Otitis Externa
- Naegleria fowleri
- Legionella
- Acanthamoeba
- Nontuberculous Mycobacterium
- Campylobacter
- E. coli (toxigenic)/HUS
- Norovirus
- Shigella sonnei
- Salmonella
- Hepatitis A
- Vibrio
- Pseudomonas
Initially focus on compiling numbers of outcomes
CDC researchers published a manuscript in 2012 describing the frequency and costs of hospitalizations and outpatient visits for ten waterborne diseases 1. Future publications will build on this analysis to include the frequency and costs of emergency room visits for selected waterborne diseases. An additional step will be to estimate the annual number of hospitalizations, deaths, and community illnesses for these selected waterborne diseases and syndromes. These analyses will determine the baseline level of potentially waterborne illness in the U.S. and will inform which pathogens are responsible for the most illnesses and the greatest health care costs. After establishing the number of illnesses, it will be possible to focus on the how much of this illness is spread via water (attribution).
Address data challenges and limitations
There are limitations to using death certificates, administrative (insurance claims) data, and health surveys.
- Estimates may be conservative since not all infected people seek health care.
- Estimates are not corrected for people who seek care but are not diagnosed by health care providers.
- There may be inconsistencies when comparing results from multiple data sources.
- Billing and diagnosis codes may not always reflect the true clinical picture.
Form research partnerships to tackle analytical challenges
Developing a comprehensive waterborne disease burden estimate will require building on the existing evidence base and forming strong partnerships with researchers throughout the water and public health sectors.
The 2012 Water and Health Conference , hosted by the Institute for the Environment and the Water Institute at the University of North Carolina at Chapel Hill, provided a forum for public health, environmental health, and water industry representatives to discuss the benefits and strategies for developing a waterborne disease burden estimate. More than 40 participants attended the waterborne disease burden workshop and requested continued involvement and communication about the project. These multidisciplinary public health agency and research partnerships are essential to improving analytical methods needed to address
References
- Collier SA, Stockman LJ, Hicks LA, Garrison LE, Zhou FJ, Beach MJ. Direct healthcare costs of selected diseases primarily or partially transmitted by water. Epidemiol Infect. 2012;140(11):2003-13.
- Page last reviewed: October 3, 2016
- Page last updated: October 3, 2016
- Content source: