


Scabies
 ShareCompartir
ShareCompartir
[Sarcoptes scabiei]
Causal Agents
Sarcoptes scabiei var. hominis, the human itch mite, is in the arthropod class Arachnida, subclass Acari, family Sarcoptidae. The mites burrow into the upper layer of the skin but never below the stratum corneum. The burrows appear as tiny raised serpentine lines that are grayish or skin-colored and can be a centimeter or more in length. Other races of scabies mites may cause infestations in other mammals, such as domestic cats, dogs, pigs, and horses. It should be noted that races of mites found on other animals may cause a self-limited infestation in humans with temporary itching due to dermatitis; however they do not multiply on the human host.
Life Cycle
Sarcoptes scabiei undergoes four stages in its life cycle: egg, larva, nymph and adult. Females deposit 2-3 eggs per day as they burrow under the skin  . Eggs are oval and 0.10 to 0.15 mm in length
. Eggs are oval and 0.10 to 0.15 mm in length  and hatch in 3 to 4 days. After the eggs hatch, the larvae migrate to the skin surface and burrow into the intact stratum corneum to construct almost invisible, short burrows called molting pouches. The larval stage, which emerges from the eggs, has only 3 pairs of legs
and hatch in 3 to 4 days. After the eggs hatch, the larvae migrate to the skin surface and burrow into the intact stratum corneum to construct almost invisible, short burrows called molting pouches. The larval stage, which emerges from the eggs, has only 3 pairs of legs  and lasts about 3 to 4 days. After the larvae molt, the resulting nymphs have 4 pairs of legs
and lasts about 3 to 4 days. After the larvae molt, the resulting nymphs have 4 pairs of legs  . This form molts into slightly larger nymphs before molting into adults. Larvae and nymphs may often be found in molting pouches or in hair follicles and look similar to adults, only smaller. Adults are round, sac-like eyeless mites. Females are 0.30 to 0.45 mm long and 0.25 to 0.35 mm wide, and males are slightly more than half that size. Mating occurs after the active male penetrates the molting pouch of the adult female
. This form molts into slightly larger nymphs before molting into adults. Larvae and nymphs may often be found in molting pouches or in hair follicles and look similar to adults, only smaller. Adults are round, sac-like eyeless mites. Females are 0.30 to 0.45 mm long and 0.25 to 0.35 mm wide, and males are slightly more than half that size. Mating occurs after the active male penetrates the molting pouch of the adult female  . Mating takes place only once and leaves the female fertile for the rest of her life. Impregnated females leave their molting pouches and wander on the surface of the skin until they find a suitable site for a permanent burrow. While on the skin's surface, mites hold onto the skin using sucker-like pulvilli attached to the two most anterior pairs of legs. When the impregnated female mite finds a suitable location, it begins to make its characteristic serpentine burrow, laying eggs in the process. After the impregnated female burrows into the skin, she remains there and continues to lengthen her burrow and lay eggs for the rest of her life (1-2 months). Under the most favorable of conditions, about 10% of her eggs eventually give rise to adult mites. Males are rarely seen; they make temporary shallow pits in the skin to feed until they locate a female's burrow and mate.
. Mating takes place only once and leaves the female fertile for the rest of her life. Impregnated females leave their molting pouches and wander on the surface of the skin until they find a suitable site for a permanent burrow. While on the skin's surface, mites hold onto the skin using sucker-like pulvilli attached to the two most anterior pairs of legs. When the impregnated female mite finds a suitable location, it begins to make its characteristic serpentine burrow, laying eggs in the process. After the impregnated female burrows into the skin, she remains there and continues to lengthen her burrow and lay eggs for the rest of her life (1-2 months). Under the most favorable of conditions, about 10% of her eggs eventually give rise to adult mites. Males are rarely seen; they make temporary shallow pits in the skin to feed until they locate a female's burrow and mate.
Transmission occurs primarily by the transfer of the impregnated females during person-to-person, skin-to-skin contact. Occasionally transmission may occur via fomites (e.g., bedding or clothing). Human scabies mites often are found between the fingers and on the wrists.
Geographic Distribution
Scabies mites are distributed worldwide, affecting all races and socioeconomic classes in all climates.
Clinical Presentation
When a person is infested with scabies mites for the first time, symptoms may not appear for up to two months after becoming infested; however, an infested person can still transmit scabies during this time. If a person has had scabies before, they become sensitized to mites and symptoms generally occur much sooner, within 1 to 4 days. Mites burrowing under the skin cause a rash, which is most frequently found on the hands, particularly the webbing between the fingers; the folds of the wrist, elbow or knee; the penis; the breast; and/or the shoulder blades. Except in crusted (Norwegian) scabies, burrows and mites may be as few as 10-15 in number and can be difficult to find. A papular "scabies rash" may be seen in skin areas such as the buttocks, scapular region and abdomen, where female mites are absent; this may be a result of sensitization from a previous infection. Severe itching, especially at night and frequently over much of the body, including areas where mites are undetectable, is the most-common symptom of scabies. A more severe form of scabies that is more common among persons who are immunocompromised, elderly, or institutionalized is called crusted (Norwegian) scabies and is characterized by vesicles and formation of thick crusts over the skin, accompanied by abundant mites but only slight itching. Complications due to infestation are usually caused by secondary bacterial infections.
Sarcoptes scabiei mites.
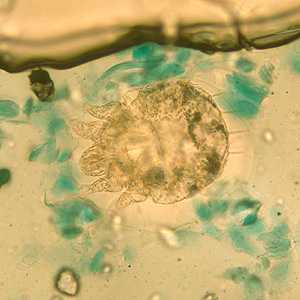
Figure A: Sarcoptes scabiei mite in a skin scraping, stained with lactophenol cotton-blue.
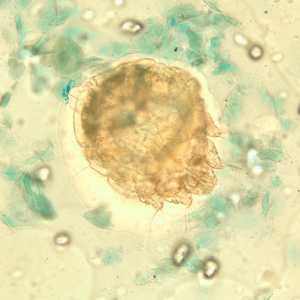
Figure B: Sarcoptes scabiei mite in a skin scraping, stained with lactophenol cotton-blue.
Sarcoptes scabiei mites in tissue specimens.
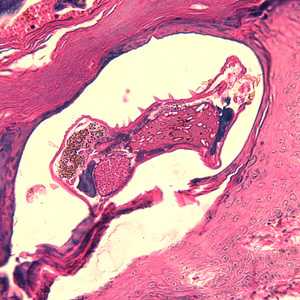
Figure A: Sarcoptes scabiei mite in a skin biopsy, stained with H&E.
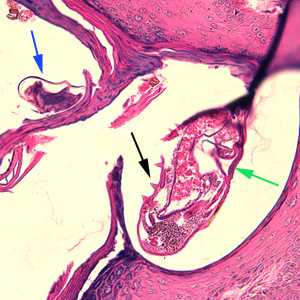
Figure B: Sarcoptes scabiei mites in a skin biopsy, stained with H&E. In this figure, both an adult (green arrow) and an egg (blue arrow) can be observed. Note also the presence of cuticular spines (black arrow) on the adult.
Follicle mites (Demodex spp.)

Figure A: Adult Demodex mite. Image courtesy of Dr. CSBR Prasad, Vindhya Clinic and Diagnostic Lab, India.

Figure B: Close-up of the anterior end of the mite in Figure A, showing the mouthparts (gnathosoma) and legs (podosoma).
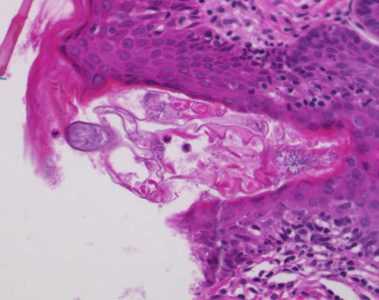
Figure C: Cross-sections of skin showing Demodex mite, stained with hematoxylin and eosin (H&E). Images courtesy of the Westchester Medical Center, Valhalla, NY. NY.
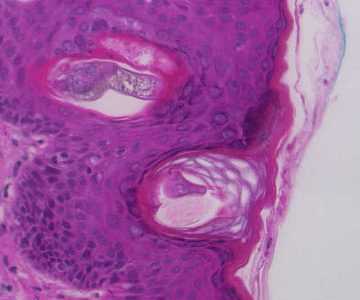
Figure D: Cross-sections of skin showing Demodex mites, stained with hematoxylin and eosin (H&E). Images courtesy of the Westchester Medical Center, Valhalla, NY.
Laboratory Diagnosis
Most diagnoses of scabies infestation are made based upon the appearance and distribution of the rash and the presence of burrows. Whenever possible scabies should be confirmed by isolating the mites, ova or feces in a skin scraping. Scrapings should be made at the burrows, especially on the hands between the fingers and the folds of the wrist. Alternatively, mites can be extracted from a burrow by gently pricking open the burrow with a needle and working it toward the end where the mite is living. The extracted mite then can be identified by microscopy.
The following is a suggested method for collecting and examining skin scrapings:
Scrapings are best performed at the end of the burrows in non-excoriated and non-inflamed areas using a sterile scalpel blade containing a drop of mineral oil. The mineral oil enhances the adherence of the mites to the blade and can then be transferred to a glass slide. An additional 1-2 drops of mineral oil can be added to the slide, followed by a coverslip for microscopic examination. Skin scrapings should be screened at 40x or 100x magnification and then evaluated at 200 to 400x magnification for confirmation.
Treatment Information
Products used to kill scabies mites are called scabicides. No "over-the-counter" (non-prescription) products have been tested and approved to treat human scabies.
The following medications for the treatment of scabies are available only by prescription.
-
Permethrin cream 5%
Brand name product: Elimite*
Permethrin is approved by the US Food and Drug Administration (FDA) for the treatment of scabies in persons who are at least 2 months of age. Permethrin is a synthetic pyrethroid similar to naturally occurring pyrethrins which are extracts from the chrysanthemum flower. Permethrin is safe and effective when used as directed. Permethrin kills the scabies mite and eggs. Permethrin is the drug of choice for the treatment of scabies. Two (or more) applications, each about a week apart, may be necessary to eliminate all mites, particularly when treating crusted (Norwegian) scabies.
-
Crotamiton lotion 10% and Crotamiton cream 10%
Brand name products: Eurax*; Crotan*
Crotamiton is approved by the US Food and Drug Administration (FDA) for the treatment of scabies in adults; it is considered safe when used as directed. Crotamiton is not FDA-approved for use in children. Frequent treatment failure has been reported with crotamiton.
-
Lindane lotion 1%
Brand name products: None available
Lindane is an organochloride. Although FDA-approved for the treatment of scabies, lindane is not recommended as a first-line therapy. Overuse, misuse, or accidentally swallowing lindane can be toxic to the brain and other parts of the nervous system; its use should be restricted to patients who have failed treatment with or cannot tolerate other medications that pose less risk. Lindane should not be used to treat premature infants, persons with a seizure disorder, women who are pregnant or breast-feeding, persons who have very irritated skin or sores where the lindane will be applied, infants, children, the elderly, and persons who weigh less than 110 pounds.
-
Ivermectin
Brand name product: Stromectol*
Ivermectin is an oral antiparasitic agent approved for the treatment of worm infestations. Evidence suggests that oral ivermectin may be a safe and effective treatment for scabies; however, ivermectin is not FDA-approved for this use. Oral ivermectin has been reported effective in the treatment of crusted scabies; its use should be considered for patients who have failed treatment with or who cannot tolerate FDA-approved topical medications for the treatment of scabies. The dosage of ivermectin is 200 mcg/kg orally. It should be taken on an empty stomach with water. A total of two or more doses at least 7 days apart may be necessary to eliminate a scabies infestation. The safety of ivermectin in children weighing less than 15 kg and in pregnant women has not been established.
* Use of trade names is for identification only and does not imply endorsement by the Public Health Service or by the U.S. Department of Health and Human Services.
DPDx is an education resource designed for health professionals and laboratory scientists. For an overview including prevention and control visit www.cdc.gov/parasites/.
- Page last reviewed: May 3, 2016
- Page last updated: May 3, 2016
- Content source:
- Global Health – Division of Parasitic Diseases and Malaria
- Notice: Linking to a non-federal site does not constitute an endorsement by HHS, CDC or any of its employees of the sponsors or the information and products presented on the site.
- Maintained By: