


Case #394 - April 2015
 ShareCompartir
ShareCompartir
A 17-year-old female presented with a crusted nodule on her left cheek two months after traveling to Israel. She admitted to camping outdoors and being bitten by insects on her face during the trip. No other symptoms were noted. A biopsy was obtained from the periphery of the nodule, placed in a sterile vial with transport media, and sent to the CDC for diagnostic work-up. Upon receipt, a touch-prep smear was prepared, fixed with methanol, stained with Giemsa, and examined. Figures A–C show was observed at 1000x magnification with oil. What is your diagnosis? Based on what criteria? What other testing, if any, would you recommend?
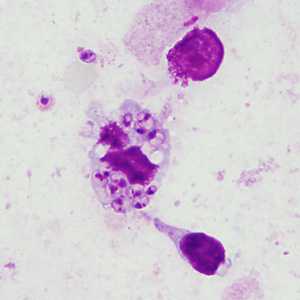
Figure A
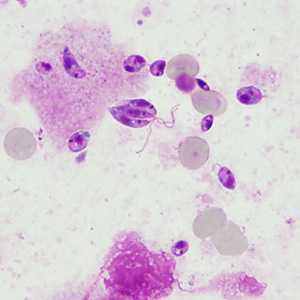
Figure B
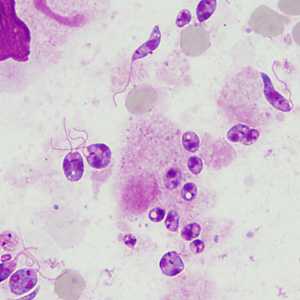
Figure C
Case Answer
This was a case of cutaneous leishmaniasis caused by Leishmania major. The genus-level diagnosis was based on the observation of amastigotes and promastigotes on the Giemsa-stained touch-prep smear. The species-level identification was based on subsequent molecular analysis, as Leishmania spp. cannot be differentiated by the morphology of the amastigotes.
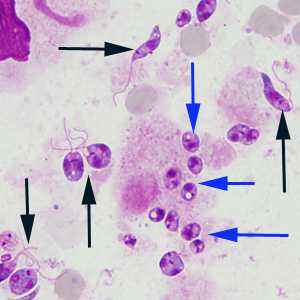
Amastigotes (blue arrows Figure C) are characterized as being small spherical to ovoid structures approximately 1-5 micrometers in length by 1-2 micrometers wide. In addition, both a nucleus and a kinetoplast should be visualized before reporting as positive. When there is a delay in shipping and/or processing, amastigotes may transform into promastigotes (black arrows Figure C) if the ambient temperature is similar to that found in the gut of the sand fly vector (Phlebotomus spp. and Lutzomyia spp.). Promastigotes are larger, elongated or spindle-shaped and have a flagellum projecting from the anterior end. Promastigote formation is never seen in Trypanosoma cruzi, the causative agent of Chagas disease and the only other organism that produces amastigotes in human tissue.
More on: leishmaniasis
Images presented in the monthly case studies are from specimens submitted for diagnosis or archiving. On rare occasions, clinical histories given may be partly fictitious.
DPDx is an education resource designed for health professionals and laboratory scientists. For an overview including prevention and control visit www.cdc.gov/parasites/.
- Page last reviewed: August 24, 2016
- Page last updated: August 24, 2016
- Content source:
- Global Health – Division of Parasitic Diseases and Malaria
- Notice: Linking to a non-federal site does not constitute an endorsement by HHS, CDC or any of its employees of the sponsors or the information and products presented on the site.
- Maintained By: