


Coenurosis
 ShareCompartir
ShareCompartir
[Taenia multiceps] [Taenia serialis]
Causal Agents
Coenurosis is infection by the metacestode larval stage (coenurus) of Taenia multiceps and T. serialis.
Life Cycle
The definitive hosts for Taenia multiceps and T. serialis are members of the family Canidae. Many canids can serve as definitive hosts for T. multiceps, but only dogs and foxes can serve as hosts for T. serialis. Eggs and gravid proglottids are shed in feces into the environment  , where they are ingested by an intermediate host
, where they are ingested by an intermediate host  . Many animals may serve as intermediate hosts, including rodents, rabbits, horses, cattle, sheep and goats. Eggs hatch in the intestine, and oncospheres are released
. Many animals may serve as intermediate hosts, including rodents, rabbits, horses, cattle, sheep and goats. Eggs hatch in the intestine, and oncospheres are released  that circulate in blood until they lodge in suitable organs (including skeletal muscle, eyes, brain and subcutaneous tissue). After about three months, oncospheres develop into coenuri. The definitive host becomes infected by ingesting the tissue of an infected intermediate host containing a coenurus
that circulate in blood until they lodge in suitable organs (including skeletal muscle, eyes, brain and subcutaneous tissue). After about three months, oncospheres develop into coenuri. The definitive host becomes infected by ingesting the tissue of an infected intermediate host containing a coenurus  . The adult cestodes reside in the small intestine of the definitive host
. The adult cestodes reside in the small intestine of the definitive host ,
,  . Humans become infected after the accidental ingestion of eggs on fomites or in food and water contaminated with dog feces
. Humans become infected after the accidental ingestion of eggs on fomites or in food and water contaminated with dog feces  . Eggs hatch in the intestine, and oncospheres are released
. Eggs hatch in the intestine, and oncospheres are released  that circulate in blood until they lodge in suitable organs and after about three months develop into coenuri
that circulate in blood until they lodge in suitable organs and after about three months develop into coenuri  . Coenuri of T. multiceps are usually found in the eyes and brain; those of T. serialis are usually found in subcutaneous tissue.
. Coenuri of T. multiceps are usually found in the eyes and brain; those of T. serialis are usually found in subcutaneous tissue.
Geographic Distribution
Widespread; most of the cases are from Africa, although cases also appear in sheep-raising areas of Europe, South America, the United States and Canada.
Clinical Presentation
Coenuri in the skin or subcutaneous tissue usually present as painless nodules. The lesions are often fluctuant and tender. Most subcutaneous nodules manifest on the trunk, sclera, subconjuctiva, neck, shoulders, head and limbs. Coenuri in the neck may affect neck movement and swallowing. Clinically, coenuri may mimic lymphomas, lipomas, pseudotumors, or neurofibromas. Coenuri in the central nervous system may cause headache, fever and vomiting. Localizing neurologic symptoms may also develop, including nerve palsies, jacksonian epilepsy, pachymeningitis, obstructive or communicating hydrocephalus, and intracranial arteritis with transient hemiparesis. Coenuri in the eye cause both intraocular and orbital infections, and patients may present with varying degrees of visual impairment. If not removed, coenuri in the eye may cause painful inflammation, glaucoma and eventually blindness.
Gross coenurus specimens.

Figure A: Large, polycephalic coenurus removed from the shoulder of a baboon (Papio sp.).

Figure B: Close-up of a coenurus of T. multiceps removed from the eye of a patient, broken open to show multiple protoscoleces.
Coenuri in tissue specimens, stained with hematoxylin and eosin (H&E).
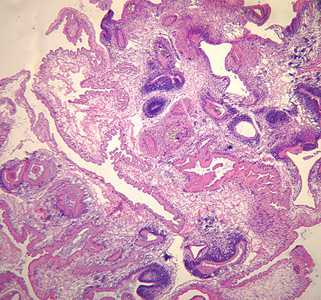
Figure A: Coenurus removed from a subcutaneous nodule in the shoulder area of a patient, stained with hematoxylin and eosin (H&E). Image taken at 50x magnification. Although the species was not identified in this case, the pathology is consistent with T. serialis.
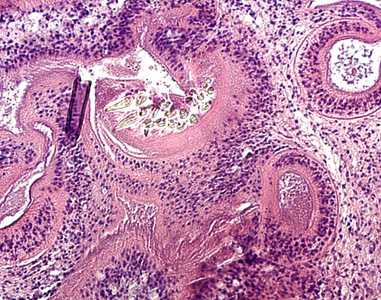
Figure B: Higher magnification (200x) of the coenurus in Figure A.
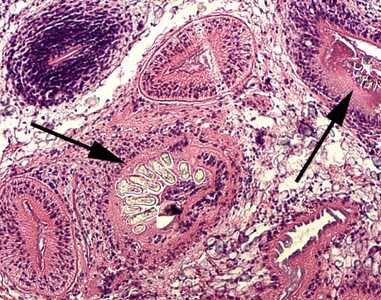
Figure C: Higher magnification (200x) of the same specimen shown in Figures A and B. The black arrows point to hooklets in the protoscoleces.
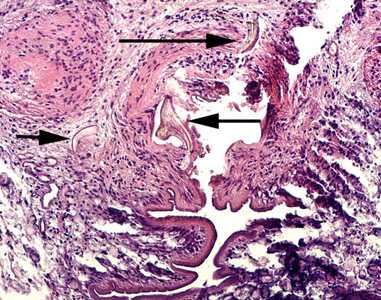
Figure D: Higher magnification (200x) of the same specimen shown in Figures A and B. The black arrows point to hooklets in the protoscoleces.
Coenurus in an eye specimens, stained with hematoxylin and eosin (H&E).

Figure A: Cross-section of a human eye, showing multiple protoscoleces within a coenurus.
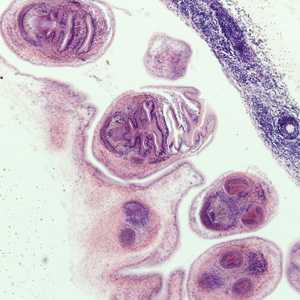
Figure B: Higher magnification (200x) of the coenurus in Figure A.
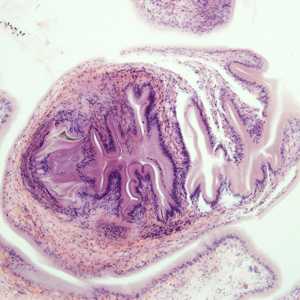
Figure C: Higher magnification (200x) of protoscoleces shown in Figures A and B.
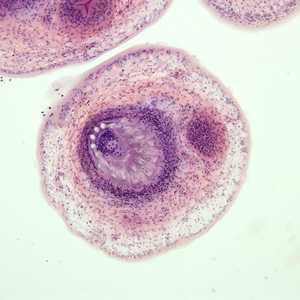
Figure D: Higher magnification (200x) of protoscoleces shown in Figures A and B.
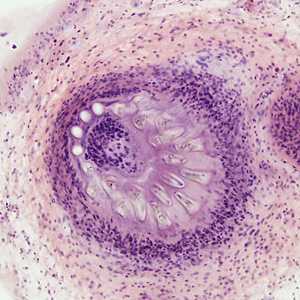
Figure E: Higher magnification of the protoscolex in Figure D, showing multiple hooklets.
Laboratory Diagnosis
Diagnosis is made by the observation of coenuri in biopsy or autopsy specimens. Coenuri are usually readily distinguished from cysticerci by the presence of multiple protoscoleces.
Treatment Information
Surgical excision is the usual treatment for intracranial coenurosis. There have also been reports of successful removal of coenuri from patients' eyes, resulting in a recovery of sight. Coenuri are susceptible to praziquantel and there are reports of patients treated with a combination of surgical intervention and antiparasitics. Praziquantel, however, can produce toxic endophthalmitis and loss of vision in intraocular coenurosis.
DPDx is an education resource designed for health professionals and laboratory scientists. For an overview including prevention and control visit www.cdc.gov/parasites/.
- Page last reviewed: May 3, 2016
- Page last updated: May 3, 2016
- Content source:
- Global Health – Division of Parasitic Diseases and Malaria
- Notice: Linking to a non-federal site does not constitute an endorsement by HHS, CDC or any of its employees of the sponsors or the information and products presented on the site.
- Maintained By: