

Spotlight on Year 1
 ShareCompartir
ShareCompartir
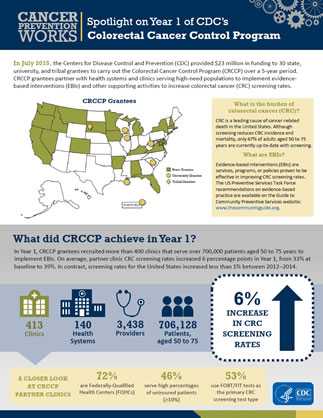
In July 2015, the Centers for Disease Control and Prevention (CDC) provided $23 million in funding to 30 state, university, and tribal grantees to carry out the Colorectal Cancer Control Program (CRCCP) over a 5-year period. CRCCP grantees partner with health systems and clinics serving high-need populations to implement evidence-based interventions (EBIs) and other supporting activities to increase colorectal cancer (CRC) screening rates.
What is the burden of colorectal cancer?
CRC is a leading cause of cancer-related death in the United States. Although screening reduces CRC incidence and mortality, only 67% of adults aged 50 to 75 years are currently up-to-date with screening.
What are EBIs?
Evidence-based interventions (EBIs) are services, programs, or policies proven to be effective in improving CRC screening rates. The U.S. Preventive Services Task Force recommendations on evidence-based practice are available on the Guide to Community Preventive Services website: www.thecommunityguide.org.
What did CRCCP achieve in Year 1?
In Year 1, CRCCP grantees recruited more than 400 clinics that serve more than 700,000 patients aged 50 to 75 years to implement EBIs. On average, partner clinic CRC screening rates increased 6 percentage points in Year 1, from 33% at baseline to 39%. In contrast, screening rates for the United States increased less than 1% between 2012 and 2014.
A closer look at CRCCP partner clinics—
- 72% are federally qualified health centers
- 46% serve high percentages of uninsured patients (10% or more)
- 53% use fecal occult blood tests (FOBT) or fecal immunochemical tests (FIT) as the primary CRC screening test type
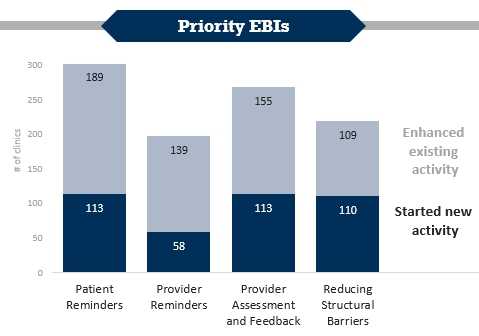
During Year 1, patient reminders were started in 113 clinics and enhanced in 189; provider reminders were started in 58 clinics and enhanced in 139; provider assessment and feedback were started in 113 clinics and enhanced in 155; and efforts to reduce structural barriers were started in 110 clinics and enhanced in 109.
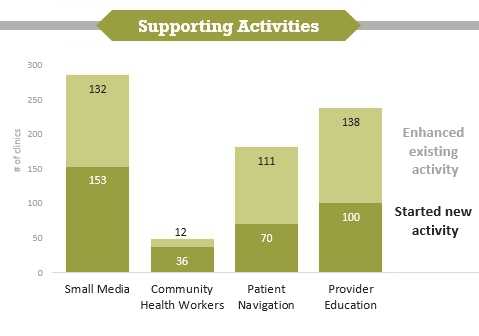
During Year 1, small media promotions were started in 153 clinics and enhanced in 132; partnership with community health workers was started in 36 clinics and enhanced in 12; patient navigation was started in 70 clinics and enhanced in 111; and provider education efforts were started in 100 clinics and enhanced in 138.
How did CRCCP increase screening rates in Year 1?
To increase CRC screening, CRCCP grantees work with clinics to start or enhance up to four priority EBIs (shown in blue) identified on the Guide to Community Preventive Services website. Four other supporting activities (shown in green) are also used in conjunction with EBIs to increase CRC screening. In Year 1, grantees most often used CRCCP resources towards patient reminder systems. These systems were newly started in 113 clinics and, for 189 clinics where patient reminders were already in place, they were enhanced to make them more effective.
In addition to clinics, CRCCP grantees work with other organizations to implement their programs. Partners conducted a variety of activities in Year 1. The five most frequently reported activities were—
- Provider education and professional development.
- Quality improvement.
- Health information technology to improve electronic health record systems.
- Patient reminders.
- Small media.
What have we learned?
- Grantees successfully launched this evidence-based, public health model for increasing CRC screening rates in clinics serving high-need populations.
- The CRCCP has the potential for significant impact as grantees continue to recruit new clinics.
- Partnerships are important to successful CRCCP implementation.
- Grantees must work closely with clinics to improve electronic health records and reliability of screening rate data.
- Page last reviewed: June 22, 2017
- Page last updated: June 22, 2017
- Content source:
- Maintained By: